

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
South Korea showed remarkable success in controlling the spread of severe acute respiratory syndrome virus 2 (SARS-CoV-2) until the emergence of the SARS-CoV-2 B.1.617.2 variant (delta). The cumulative incidence of COVID-19 in children aged 0–19 years was 245 per 100,000 as of July 17, 2021.1 The true incidence may not be far from the reported incidence considering the vigorous contact tracing and the low seroprevalence of SARS-CoV-2–specific antibodies in South Korea. SARS-CoV-2 seropositive rates in the Korean population who had not been diagnosed previously with COVID-19 were low at 0.17% in 1,200 children and adults between May and July 2021 and 0.25% in 3,473 healthy adult men aged < 30 years during June 2021.2 After the delta variant became dominant in mid-July 2021,3 the number of SARS-CoV-2-infected children increased beyond what was seen in the previous waves. South Korea started vaccinating children 12- to 17-year-olds against COVID-19 in mid-October 2021. As of December 31, 2021, 74.0% of 12- to 17-year-olds received the first dose, and 49.8% completed the second dose. However, since the prevalence of SARS-CoV-2 infection had been low and vaccination began late in 2021, most Korean children had no preexisting immunity to SARS-CoV-2 at the time of their COVID-19 diagnosis.
In a Korean study analyzing critical COVID-19 among children from January 2020 to October 2021, seven of eight critically severe cases occurred during delta predominance.4 However, there has been little evidence that the delta variant increases the risk of severe COVID-19 in children.5678 Nevertheless, since these studies were conducted where SARS-CoV-2 seroprevalence was substantial due to infection and vaccination, the severity of the delta variant might be underestimated. Therefore, we conducted a multicenter study on the clinical features and outcomes of COVID-19 that occurred in the predelta-predominant and delta-predominant periods in Korean children, who were mostly SARS-CoV-2-naïve at the time of infection.
METHODS
Setting
This is a multicenter retrospective cohort study of patients with polymerase chain reaction-confirmed SARS-CoV-2 infection hospitalized at 8 hospitals in South Korea (Eulji University Hospital in Seoul, National Medical Center in Seoul, Seoul National University Children’s Hospital in Seoul, Inha University Hospital in Incheon, Seoul National University Bundang Hospital in Seongnam, Chungbuk National University Hospital in Cheongju, Pusan National University Hospital in Busan, and Jeju National University Hospital in Jeju). Patients 0–18 years of age hospitalized with COVID-19 between January and December 2021 were eligible for inclusion. Cases of multisystem inflammatory syndrome in children were excluded. Demographic and clinical data were retrospectively collected.
Definitions
We used two different approaches for the classification of COVID-19 severity. First, we classified cases as either hospitalization with medical needs or hospitalization for isolation because many were admitted for isolation. For this categorization, the principal investigator reviewed the clinical course of each patient and attempted to discern whether COVID-19 symptoms alone would have resulted in hospitalization. Those with prolonged fever (fever > 3 days), poor feeding or dehydration requiring intravenous fluid, the need for intravenous medications for treating COVID-19 symptoms or complications, new-onset or aggravated seizures, respiratory distress, or unstable vital signs or altered mental status and neonates with fever ≥ 38.0°C were classified as hospitalized with medical needs. The remaining cases were classified as hospitalization for isolation.
Second, we classified cases as mild, moderate, severe, or critical COVID-19 with regard to pneumonia presence and illness severity. Pneumonia was defined when there was consolidation on chest radiographs or any infiltration with compatible clinical features. Mild COVID-19 was defined as SARS-CoV-2 infection without pneumonia. Moderate COVID-19 was defined as pneumonia with an oxygen saturation (SpO2) ≥ 94% on room air. Severe COVID-19 was defined as pneumonia with SpO2 < 94% on room air and the need for respiratory support, therapeutic remdesivir, and/or corticosteroids. Critical illness was defined as respiratory failure and/or the need for intensive care regardless of pneumonia severity.
A 7-day threshold for defining vaccination status was used as previous literature has suggested.91011 Fully vaccinated were defined as those who completed their primary series ≥ 7 days before a positive SARS-CoV-2 test associated with their hospitalization. Those who received only 1 vaccine dose ≥ 7 days before the SARS-CoV-2 test date were considered partially vaccinated.
Obesity was defined when the body mass index was above the 95th percentile in children ≥ 2 years of age.
Comparison of COVID-19 severity before and during SARS-CoV-2 delta variant predominance
To compare the clinical severity of the delta variant in the absence of genomic confirmation of the SARS-CoV-2 variant, we used two time periods: the predelta-predominant period in South Korea, namely, January 1 to July 17, 2021 (epidemiological weeks 1–29), and the delta-predominant period, namely, July 18 to December 31, 2021 (epidemiological weeks 30–53) (Fig. 1).12 Because the thresholds for admitting children with COVID-19 changed over time with national policy and hospital bed capacity, the proportions of children with moderate-to-critical COVID-19 in relation to children hospitalized with medical needs were used to compare the clinical severity between periods.
Fig. 1
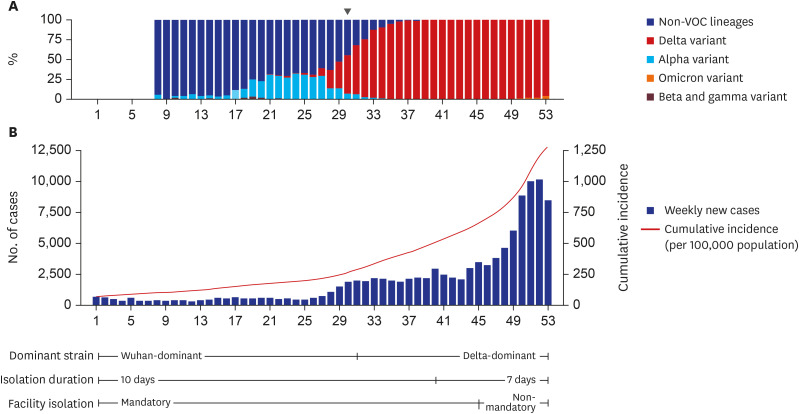
Epidemiologic curve and isolation policy of SARS-CoV-2 infection, South Korea, 2021. (A) Weekly distribution of SARS-CoV-2 variants in domestic cases. The delta variant became predominant at week 30 (arrow); (B) Weekly national new cases in children and adolescents aged 0–19 years and changes in national isolation policy.
VOC = variants of concern, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
Statistical analysis
Demographic characteristics are summarized using frequencies and percentages for categorical variables and medians with interquartile ranges for continuous variables. The nonparametric Wilcoxon rank test and χ2/Fisher’s exact test were used as appropriate. Factors associated with hospitalization and COVID-19 severity were assessed using multivariable logistic regression. Multivariable models on the association between underlying medical conditions and moderate-to-critical COVID-19 were specified separately for children aged < 2 years and 2 to 18 years because underlying conditions such as prematurity and obesity are clinically relevant for specific age groups.
A 2-sided P < 0.05 was used to define statistical significance. All statistical analyses were performed using STATA/SE 17.0 (Stata Corporation, College Station, TX, USA) and R, version 4.1.0 (R project for Statistical Computing, http://www.R-project.org).
RESULTS
Demographics, epidemiology, and comorbidities
The study population comprised 753 children aged 0 to 18 years who were hospitalized with SARS-CoV-2 infection between January and December 2021, including 229 (30.4%) in the predelta-predominant cohort and 524 (69.6%) in the delta-predominant cohort. In South Korea, 86.3% of pediatric COVID-19 cases in 2021 occurred during delta predominance (Fig. 1).
The clinical and demographic characteristics are shown in Table 1. The median age was 6.2 years, and 57.6% were male. There was no significant difference in the age distribution between the two periods (P = 0.873). The proportion of patients with household exposure decreased (from 69.0% to 56.3%, P < 0.001), and the proportion of patients with unknown exposure increased (from 12.7% to 26.7%, P < 0.001) during the delta-predominant period.
Table 1
Demographics and epidemiology of children and adolescents hospitalized with COVID-19 in South Korea from January to December 2021
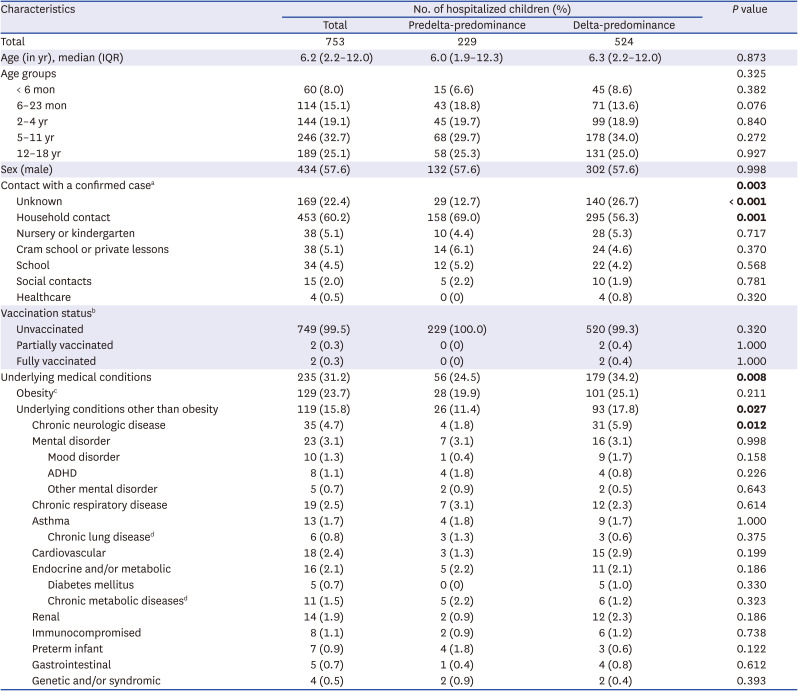
The values in bold represent statistically significant correlations.
COVID-19 = coronavirus disease 2019, IQR= interquartile range, ADHD = attention-deficit/hyperactivity disease, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
aInformation on contact with a person with confirmed COVID-19 disease was available in 751 cases.
bFully vaccinated children were defined as those who had received the final dose in their primary series ≥ 7 days before a positive SARS-CoV-2 test associated with their hospitalization. Children who received only 1 vaccine dose ≥ 7 days before the SARS-CoV-2 test date were considered partially vaccinated.
cObesity was defined as body mass index ≥ 95th percentile for children aged ≥ 2 years.
dChronic lung disease excludes asthma, and chronic metabolic disease excludes diabetes mellitus.
Most (99.3%) were assumed to be SARS-CoV-2 naïve at the time of their COVID-19 diagnosis. One patient had a prior history of SARS-CoV-2 infection, and 4 patients received at least one dose of a COVID-19 vaccine.
Thirty-one percent of all subjects had underlying conditions. Obesity was the most common (23.7%) condition, followed by neurologic diseases (4.7%) and mental disorders (3.1%). Children from the delta cohort were more affected by underlying conditions (24.5% vs. 34.2%, P = 0.008). The most common underlying disease in both periods was obesity. More children with chronic neurologic conditions were hospitalized during delta predominance (1.8% during predelta predominance and 5.9% during delta predominance, P = 0.012).
Clinical manifestation and severity of COVID-19 between the two study periods
Table 2 summarizes the clinical manifestations and severity of COVID-19 during the study periods. Admission for isolation, which consisted of patients who initially presented with mild symptoms, was most common (82.9%).
Table 2
Clinical manifestations of COVID-19 in hospitalized children and adolescents in South Korea from January to December 2021
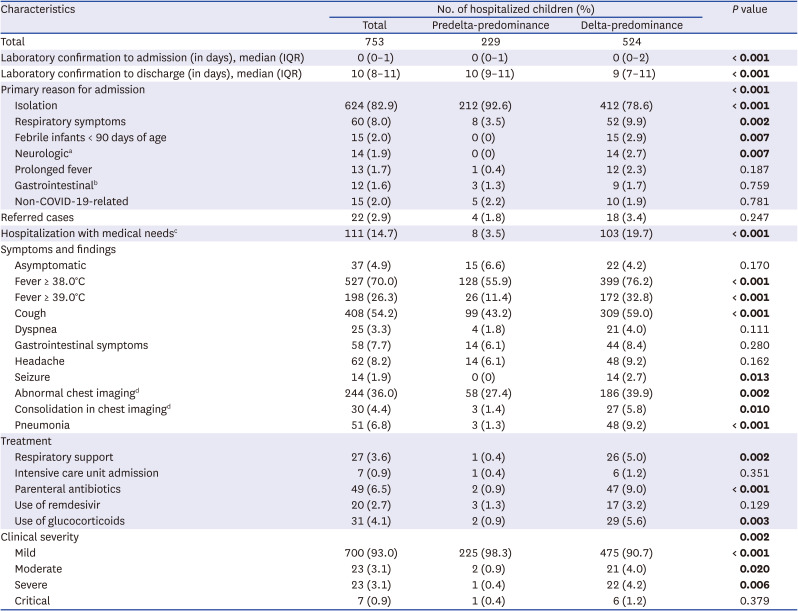
The values in bold represent statistically significant correlations.
COVID-19 = coronavirus disease 2019, IQR = interquartile range.
aNeurological symptoms included new-onset seizure or aggravation of preexisting seizure.
bGastrointestinal symptoms included abdominal pain or discomfort, nausea, vomiting, and diarrhea.
cPatients initially admitted with mild COVID-19 symptoms who developed new or worsening symptoms that would have ultimately driven hospital admission were included.
dChest radiographs were taken in 678 cases.
Fever (70.0%) and cough (54.2%) were noted as the two main symptoms. While abnormal chest radiographs were observed in 36.0%, clinical pneumonia was diagnosed in 6.8% of all cases. Overall, 30 (4.0%) children had severe-to-critical COVID-19. There were no deaths in the study population.
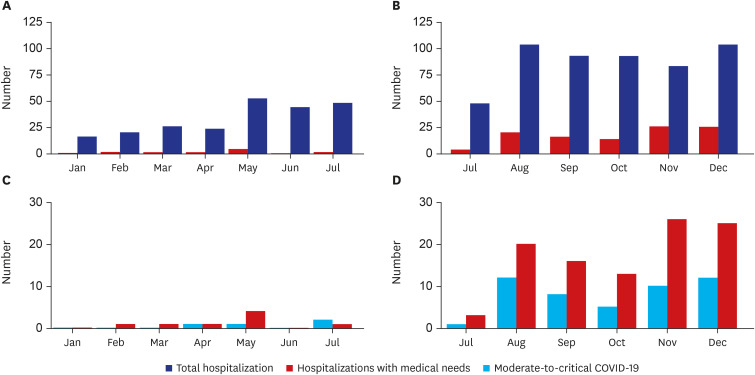
Compared with the predelta-predominant period, hospitalization for isolation decreased (92.6% vs. 78.6%, P < 0.001), and rates of fever (55.9% vs. 76.2%, P < 0.001), cough (43.2% vs. 59.0%, P < 0.001), and seizure (0% vs. 2.7%, P = 0.013) increased during the delta-predominant period. Accordingly, the proportions of hospitalization with medical needs (3.5% vs. 19.7%, P < 0.001), moderate illness (0.9% vs. 4.0%, P = 0.020) and severe-to-critical illness (0.8% vs. 5.3%, P = 0.004) also increased during the delta-predominant period (Fig. 2). The number of median days from COVID-19 diagnosis to discharge was shortened during the delta-predominant period, which was related to changes in national isolation policy. Most children were discharged on the 10th or 7th day of symptom onset when isolation was lifted.
Fig. 2
Monthly distribution of hospitalizations with COVID-19 among children and adolescents aged 0–18 years before and after SARS-CoV-2 delta predominance in 2021 by medical needs and disease severity. (A) Hospitalizations with medical needs in the predelta-predominant period; (B) Hospitalizations with medical needs in the delta-predominant period; (C) Moderate-to-critical disease in the predelta-predominant period; (D) Moderate-to-critical disease in the delta-predominant period.
COVID-19 = coronavirus disease 2019, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
Demographics and clinical manifestation of COVID-19 among children hospitalized with medical needs
Among 111 patients hospitalized with medical needs, the median age was 9.9 years, and 64.9% were male (Supplementary Table 1). They were older than patients hospitalized for isolation and more prone to underlying conditions (P = 0.003 and P < 0.001, respectively). Specifically, the proportions of obesity (44.4%), neurologic disease (9.9%), mental disorder (7.2%), and diabetes mellitus (2.7%) were significantly higher (P < 0.001, P = 0.011, P = 0.012, and P = 0.025, respectively). Most (93.6%) were infected during the delta-predominant period. No one had a prior history of SARS-CoV-2 infection or a history of vaccination against COVID-19.
Common reasons for admission were respiratory distress (43.2%), followed by new-onset or aggravated seizure (12.6%) and prolonged fever (11.7%). Clinical pneumonia was diagnosed in 41.4% of patients. Severe and critical COVID-19 accounted for 27.0%. Respiratory support was required in 24.3% of patients, and 6.3% of patients underwent critical care. The time from diagnosis to discharge was affected by the change in the isolation policy rather than the need for hospitalization.
Risk factors for moderate-to-critical COVID-19
There was no male predominance in moderate-to-critical COVID-19 (adjusted odds ratio [aOR], 1.6; 95% confidence interval [CI], 0.9–3.1; P = 0.130). Moderate-to-critical disease was significantly less likely in children aged < 12 years (aOR, 0.2; 95% CI, 0.1–0.4; P < 0.001). Underlying medical conditions, including obesity, were significantly associated with an increased risk of moderate-to-severe COVID-19 (aOR, 3.4; 95% CI, 1.8–6.3; P < 0.001) (Table 3). For individual underlying conditions in children aged 2 years or older, obesity (aOR, 5.2; 95% CI, 2.7–10.0; P < 0.001) and chronic lung disease (aOR, 24.4; 95% CI, 1.2–493.3; P = 0.037) were associated with an increased risk of moderate-to-critical COVID-19 (Table 3). The presence of underlying medical conditions was not associated with an increased risk of more severe COVID-19 in children aged younger than 2 years.
Table 3
Demographic characteristics and underlying conditions associated with moderate-to-critical COVID-19
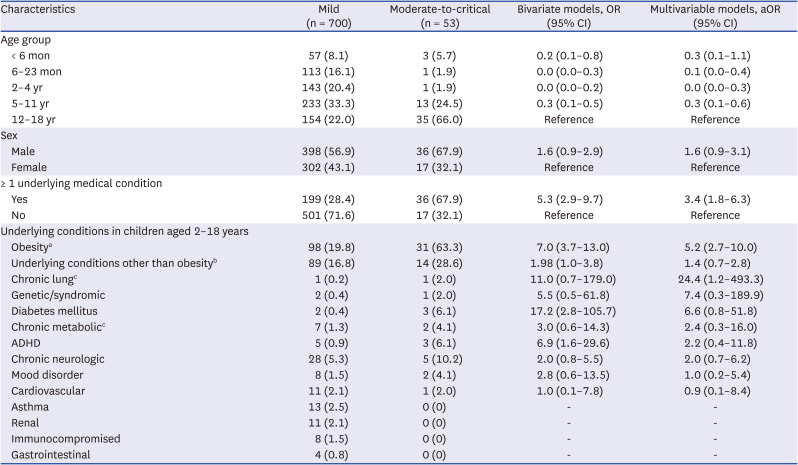
COVID-19 = coronavirus disease 2019, OR = odds ratio, CI = confidence interval, ADHD = attention-deficit/hyperactivity disorder.
aObesity was defined as body mass index ≥ 95th body mass index percentile for children aged ≥ 2 years. Multivariable models were adjusted for age group, sex and presence of underlying conditions other than obesity.
bMultivariable models are adjusted for age group, sex and presence of obesity.
cChronic lung disease excludes asthma, and chronic metabolic disease excludes diabetes mellitus.
Although the number of patients with moderate-to-critical COVID-19 was increased during the delta-predominant period, the between-period comparison showed that there was no statistically significant difference in the proportion of moderate-to-critical COVID-19 among cases hospitalized with medical needs (25.0% in the predelta period vs. 43.7% in the delta-predominant period, P = 0.432) (Supplementary Table 2). Among cases hospitalized with medical needs, the risk of moderate-to-critical COVID-19 was higher among patients aged 12–18 years (aOR, 4.1; 95% CI, 1.5–11.8; P = 0.008) and with obesity (aOR, 6.9; 95% CI, 2.4–19.6; P < 0.001) but not among patients with presumptive delta variant infection (aOR, 4.6; 95% CI, 0.7–30.7; P = 0.119) (Supplementary Table 3).
For children with obesity, the risk of moderate-to-critical COVID-19 was higher during the delta-predominant period after adjusting for age group, sex, and presence of other underlying conditions (aOR, 6.1; 95% CI, 1.2–29.6; P = 0.026). In contrast, COVID-19 severity in nonobese children was not affected by whether they were infected during delta predominance (aOR, 3.6; 95% CI, 0.8–16.4; P = 0.094).
Neonates and infants younger than 6 months of age
During the study periods, 60 infants younger than 6 months of age were hospitalized with COVID-19, including 40 infants younger than 3 months of age. Over 90% of infants had a history of household exposure to SARS-CoV-2. With the exception of one case in which a 19-day-old neonate presented with fever, lethargy, and desaturation, most infants presented with mild symptoms but were hospitalized due to their young age. In particular, approximately one-third (35%) of infants younger than 3 months of age were hospitalized due to the concern for concomitant serious bacterial infection. Of the 60 infants younger than 6 months of age, 4 infants (6.7%), who were all younger than 3 months of age, received empirical intravenous antibiotics that were discontinued when cultures returned negative for bacterial coinfection. Overall, 57 (95.0%) had mild disease, 2 (3.3%) had moderate disease, and one (1.7%) who presented with desaturation had severe disease.
DISCUSSION
The current study described the epidemiology, clinical manifestations, and outcomes of hospitalized children with COVID-19 before and after the dominance of the delta variant in 2021 through the largest multicenter cohort in South Korea. Although the number of moderate-to-critical COVID-19 cases increased after delta predominance, the delta variant showed similar severity to previous strains in most children and adolescents. Obesity was the most common comorbidity and affected COVID-19 severity.
Early reports and systematic reviews revealed the favorable outcomes of pediatric COVID-19.1314151617 After the emergence of SARS-CoV-2 variants of concern, reports indicated that clinical severity and treatment requirements among children infected with the new variants B.1.1.7 (alpha), B.1.351 (beta), and P.1 (gamma) were similar to those of children infected with wild-type SARS-CoV-2.1819
Pediatric COVID-19 cases and the rates of hospitalization increased following the emergence of the delta variant.67 Nevertheless, severity levels were similar, and the rate of hospitalization resulting in ICU admission or invasive mechanical ventilation did not dramatically change after delta-predominance in the United States.8 Furthermore, a nationwide study in Mexico found a reduced risk of pneumonia in unvaccinated children during delta-variant dominance.20
In our mostly SARS-CoV-2 naïve cohorts, an increased proportion of moderate-to-critical COVID-19 during delta predominance was observed. A similar trend was observed in a nationwide study in Japan, which had a low prevalence of COVID-19, hospitalized almost all infected children, and delayed vaccinating children until delta dominance.21 Although the proportion of Japanese children admitted to the ICU increased during the delta period (1.4% vs. 0.1%), the proportion of patients with underlying diseases also increased. Therefore, it was difficult to directly compare the two periods because the population of hospitalized children might differ between periods.
Until the predominance of the delta variant in each country, the cumulative infection rates of COVID-19 in Korea and Japan were less than 1%.22 More children with underlying diseases were inevitably infected during the delta period. The increased proportion of severe COVID-19 during delta predominance might be the result of an increase in community SARS-CoV-2 transmission and subsequent change in the thresholds for admitting patients. No significant difference was observed in the overall proportion of moderate-to-critical COVID-19 among cases hospitalized with medical needs in our study.
A Korean study including previously healthy and nonhospitalized children with COVID-19 suggested that delta variant infection did not cause worse clinical outcomes, such as pneumonia and hospital transfer, than previous variants did in unvaccinated children and adolescents.23 Interestingly, we observed increased severity of COVID-19 during delta predominance in children with comorbidities. It is notable that the proportion of severe COVID-19 increased nationally in Korea and Japan, where most children with comorbidities were SARS-CoV-2 naïve before delta predominance.
To date, various studies have reported risk factors for severe COVID-19.24252627 According to recent meta-analyses on risk factors for severe progression of COVID-19 in children, neonates, prematurity, obesity, diabetes mellitus, chronic lung disease, heart disease, neurologic disease, and immunocompromised status were suggested.2829 However, most studies included data collected during the early phase of the pandemic when treatment policies were not yet established and patients with various underlying diseases were more likely to receive aggressive management, such as preemptive ICU care. This early trend might produce some bias to the studies on the outcome of COVID-19 in patients with specific underlying medical conditions.30 Moreover, the outcomes of COVID-19 might be affected by each country’s epidemic situation, vaccination progression, and ethnicity distribution.3132 Therefore, risk factors for more severe COVID-19 in children may vary by time period and country.
Previously suggested risk factors other than obesity and chronic lung diseases did not appear significant in the current study, but the conclusion is limited, as the number of subjects with each medical condition was low. However, obesity was once again confirmed to be a significant risk factor for severe COVID-19, particularly at 12–18 years of age.
The delta variant may not be associated with more severe COVID-19 in most children and adolescents. However, our results suggest that children who have high-risk medical conditions and have no preexisting immunity to SARS-CoV-2 may experience more severe COVID-19 due to a variant with delta severity. Increased transmissibility itself could make at-risk children more vulnerable to SARS-CoV-2 infection and possibly result in more severe outcomes. Therefore, it is strongly recommended that children with high-risk medical conditions be vaccinated against COVID-19 to prevent severe outcomes.
The findings of this study have several limitations. First, this is not a nationwide hospitalization surveillance. However, since the participating institutions were among the hospitals that most actively responded to pediatric patients with moderate-to-critical COVID-19 in each region, our cohort is largely representative of COVID-19 disease spectrum of hospitalized children in Korea, including mild cases and moderate-to-critical cases. Second, as the number of children with COVID-19 increased, the subsequent increase in the absolute number of moderate-to-critically ill cases probably affected the overall severity of children admitted to the participating institutions. To compensate for this limitation, we used the proportions of children with moderate-to-critical COVID-19 in relation to children hospitalized with medical needs to compare the clinical severity between periods, but it is still possible that the severity of the delta-predominant period was overestimated. Third, risk factor analysis and comparison between periods were based on a small number of patients with moderate-to-critical disease. Finally, information on the SARS-CoV-2 lineages was not available. Therefore, the impact of the delta variant on COVID-19 outcomes could not be directly assessed.
In conclusion, we observed a similar severity of COVID-19 in Korean children during the delta-predominant period. Childhood obesity significantly affected the severity of COVID-19. Although the outcomes of SARS-CoV-2 infections in children are mostly favorable, a more transmissible or more virulent variant’s circulation may play a crucial role in more severe outcomes in certain groups, thus emphasizing the importance of immunization of eligible children.
 XML Download
XML Download