

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The widespread coronavirus disease 2019 (COVID-19) has caused substantial worldwide health and social impacts for two years, since the first case of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection was identified in December 2019.1 However, the administration of effective COVID-19 vaccines and immunity acquired through natural infection have greatly reduced the extent and intensity of the epidemic. Moreover, as the omicron variant (B.1.1.529) is suggested to have a lower risk of hospitalization than other SARS-CoV-2 variants, some developed countries are attempting to transition from epidemic to endemicity.2
The pattern of the COVID-19 epidemic in the second quarter of 2022 shows a unique regional context.3 In Western countries including the United States, the United Kingdom, and European countries, the epidemic was brought under control after repeated epidemic waves of similar size over the last two years. East Asian countries such as the Republic of Korea (hereafter, “South Korea”), Japan, and Taiwan, which experienced relatively low incidences of COVID-19, also entered a stable state after a large-scale epidemic of the omicron variant that was several to tens of times larger than previous waves. In contrast, China and the Democratic People’s Republic of Korea (hereafter, “North Korea”) have adopted a “zero-COVID” strategy, maintaining the incidence of SARS-CoV-2 infections as low as possible via stringent lockdown policies and movement restrictions.4567 However, as local blockades have been implemented in China following a rapid spread of the omicron variant, the zero-COVID strategy’s sustainability has been questioned.8
With the economic sanctions and diplomatic isolation of North Korea, establishing a proper COVID-19 response strategy may be even more challenging. For the last two years, North Korea closed its borders and curtailed the influx of COVID-19, enabling the country to maintain a near-zero incidence of COVID-19. Nevertheless, when the resurgence of COVID-19 occurred in China, the only country with whom North Korea has external relations, North Korean authorities acknowledged that COVID-19 was spreading considerably on 12 May 2022.9 The daily reported number of probable COVID-19 cases in North Korea peaked at approximately 400,000; however, as of 26 May 2022, a declining trend in the incidence of infections has been reported as a consequence of the government’s response, which included declaring a maximum emergency and imposing stringent lockdowns.10 Despite the decreasing trend in COVID-19 incidence in North Korea, concerns regarding the disease burden continue to grow. With widespread malnutrition and the absence of a stable healthcare system, the current COVID-19 epidemic has the potential to exacerbate the overall disease burden in North Korea.11 Furthermore, the accessibility to COVID-19 vaccines has been very limited in North Korea, and the country is thought to have an insufficient vaccine-induced immunity level.12 Low population-level immunity may lead to an upsurge of COVID-19 hospitalizations, exceeding the available hospital bed capacity in North Korea when the current, stringent public health and social measures (PHSMs) are eased. In response, various international cooperation proposals have been made, though it remains unclear whether these proposals will proceed.13
To avoid such tragedy and minimize the disease burden in North Korea, a tailored COVID-19 response strategy should be designed under the guidance of quantitative assessment. Therefore, despite limited data, a model-informed approach to projecting COVID-19 transmission scenarios in North Korea is reported in this study. Using the model, this study aimed to assess the damage level of the current COVID-19 epidemic in North Korea and suggest the potential impact of nationwide vaccination on the disease dynamics in the country by comparing COVID-19 epidemiological outcomes of various scenarios.
METHODS
Epidemiological data
The Korean Central News Agency (KCNA) website was accessed to retrieve the epidemic curve of probable COVID-19 cases in North Korea from 12 May to 26 May 2022.10 Probable cases were defined as individuals having either an epidemiological link with other probable cases or COVID-like symptoms (such as fever).14 However, due to the limited testing capacity in North Korea (e.g., the reported cumulative confirmed COVID-19 cases were 186 as of 14 May 2022, while 296,180 probable cases were newly reported the same day), all probable cases were assumed to be symptomatic cases in this study. In addition to case counts, the daily numbers of COVID-19 deaths in North Korea were reported, though these data were not used in the current study due to a large number of famine-related deaths15 and a lack of capacity for post-mortem COVID-19 testing in North Korea.
Extrapolation of probable COVID-19 cases in North Korea
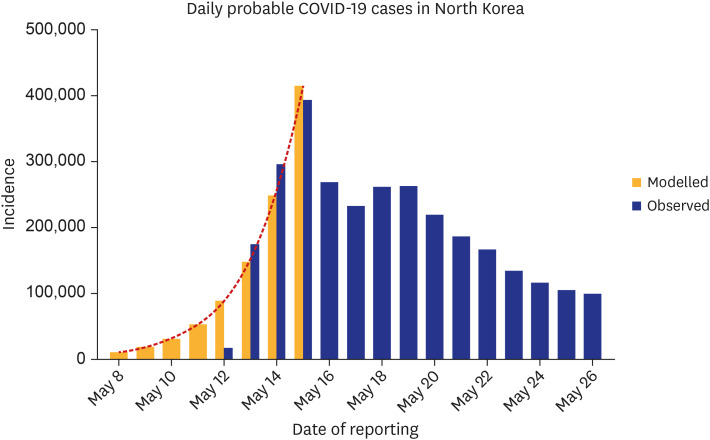
As the number of probable COVID-19 cases in North Korea was available beginning in the middle of the epidemic (when the number of newly reported cases had already approached 200,000), the observed incidence by the date of report t, i(t), was extrapolated using an exponential growth model with the rate r: i(t) = i0exp(rt), where i0 is the expected number of cases at time t = 0.16 Both r and i0 were estimated by fitting the exponential growth model to the reported case counts throughout the increasing trend from 12–15 May 2022 (Fig. 1). Then, the cumulative incidence by the date of report t, Icumul(t), was calculated as an integral of i(t) over time from 0 to t: Icumul(t) = i0(exp(rt) − 1)/r.
Fig. 1
Probable COVID-19 cases in North Korea by date of reporting. The epidemic curve of probable COVID-19 cases in North Korea by date of reporting is shown. The blue bars represent the empirically observed case counts, and the yellow bars represent the extrapolated case counts based on the exponential growth model. The red lines represent the 95% confidence intervals derived using the parametric bootstrap method.
COVID-19 = coronavirus disease 2019.
Model formulation and parameterization
A simple, discrete-time, deterministic, compartment model governing the SARS-CoV-2 transmission dynamics in North Korea was devised to calibrate a parameter and served as a baseline model (Fig. 2A). The baseline model was composed of six states: susceptible (S), exposed (E), infectious (I), hospitalized (H) (i.e., admitted to the intensive care unit, indicating severe COVID-19 cases), recovered (R), and deceased (D). First, susceptible individuals who had contact with an infectious individual transitioned to exposed status (E) following the force of infection, λ, for a susceptible individual was modelled as:
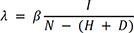
Fig. 2
Schematic diagrams for modelling framework. Diagrams showing a compartment model and transition rates for (A) the baseline model and (B) the extended model integrating nationwide vaccination are shown. S, E, I, R, H, and D denote susceptible, exposed, infectious, recovered, hospitalized (severe COVID-19 cases), and deceased states, respectively. Subscript v indicates individuals who are vaccinated with the first dose, and subscript f indicates those who are vaccinated with the second dose. Subscript n indicates the month since the second dose was administered representing the time-varying vaccine effectiveness.
COVID-19 = coronavirus disease 2019.
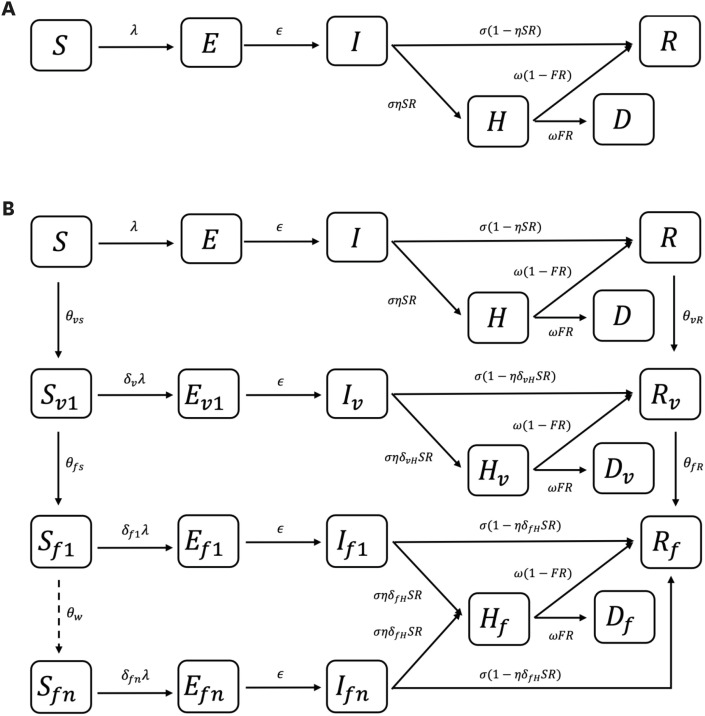
where β stands for the probability of a successful transmission given a single contact with an infectious individual which is assumed to be identical between symptomatic and asymptomatic cases. N is the total population corresponding with a sum of individuals in all six states. After contracting the disease, exposed individuals become infectious after a latent period (1/ε). Infectious individuals move to either recovered states (R) or hospitalized states (H) following the infectious period (1/σ) based on age-adjusted risk of severity (SR). The symptomatic proportion of total infected individuals (η) is based on the assumption that asymptomatic cases will not progress to severe cases. In addition, hospitalized individuals transition to either recovered (R) or deceased (D) states based on the age-adjusted fatality risk among hospitalized cases (FR) and duration of hospitalization (1/ω). In this study, the FR was calculated based on the age-adjusted infection fatality risk (IFR): FR = IFR/SR.
Then, β was estimated by fitting the baseline model to the reported incidence between 12–14 May 2022. The incidence data during this timeframe was analyzed as the effective reproduction number dropped below one on 14 May, based on the three-day incubation period and generation time of the omicron variant.17 Although the implementation of stringent PHSMs was first reported on 13 May,18 such a decline in the effective reproduction number may imply that the PHSMs began to have a significant impact on the disease dynamics from 14 May. The expected number of the newly reported probable cases on day t, E(reported(t)), was modelled as:

where ηβSI(t) indicates the number of symptomatic cases who move from S state to E state through contact with infectious individuals (both symptomatic and asymptomatic cases assuming the identical infectiousness between them) on day t. g(.) is the probability mass function of the incubation period distribution,17 assuming no time delay from symptom onset to reporting due to a lack of information. It was assumed that reported(t) follows a Poisson distribution, and all utilized parameters (i0, r, and β) were jointly estimated using maximum likelihood estimation. The 95% confidence intervals (CIs) of parameters were calculated using the parametric bootstrap method with 5,000 times resampling. The reproduction number of COVID-19 cases prior to the implementation of stringent PHSMs was derived as: β/σ. The full details of the model parameters are presented in the Supplementary Table 1.
Numerical simulations for evaluating the impact of stringent PHSMs
Based on the proposed model, numerical simulations were performed to evaluate the effect of stringent PHSMs by comparing the empirically observed and projected incidences of probable COVID-19 cases in North Korea. To model the impact of stringent PHSMs on SARS-CoV-2 transmission, a constant, k, was multiplied by the estimated β from 13 May 2022. In each simulation, the asymptomatic proportion of total COVID-19 cases was altered (1 − η: ranging from 30% to 50%), along with the reduction level of transmissibility (k; ranging from 0.2 to 1). The asymptomatic proportion of total infected cases differs depending on the rigor of epidemiological investigations (particularly in circumstances where the testing capacity is limited, as in North Korea), and such variations in asymptomatic cases (i.e., underreporting of cases following the assumption that all reported probable cases in North Korea are symptomatic) can change how PHSMs affect the transmission dynamics of COVID-19 (e.g., a large number of individuals with natural immunity may primarily lead to a decline in incidence rather than interventions). Therefore, the impact of stringent PHSMs was quantitatively evaluated by varying both factors (η and k) and comparing the epidemiolocal outcomes of the COVID-19 epidemic as the number of newly reported probable COVID-19 cases and the prevalence of severe cases. The moderate asymptomatic proportion was set at 30%,1920 while the highest value was set at 50% to reflect the possibility that an epidemiological investigation and testing capacity in North Korea may be insufficient to identify all symptomatic cases due to the massive daily incidence. The highest value (i.e., 50% of asymptomatic proportion) was introduced to demonstrate the effect of nationwide COVID-19 vaccination in a setting where considerably more individuals have natural immunity than the reported number of probable COVID-19 cases in North Korea.
Numerical simulations with the nationwide COVID-19 vaccination
To assess the potential impact of nationwide vaccination on the transmission dynamics of COVID-19 in North Korea, nationwide vaccination was incorporated into the baseline model (Fig. 2B). Due to the scarcity of vaccines and the enormity of the current COVID-19 epidemic in North Korea, it was assumed that people who have not been reported as probable cases would be given first priority in a vaccine roll-out. Accordingly, individuals in the S state, as well as the asymptomatic proportion of those who recovered ((1 − η) × individuals in the R state), were included in the target group for nationwide vaccination. The roll-out of vaccines was modelled to be distributed among the target group in a randomly uniform manner from 1 June 2022, and the second dose was expected to be administered 21 days later to everyone who received the first dose.21 In addition, the COVID-19 vaccine was assumed to provide prompt protection to a subset of the vaccinated individuals based on the time-varying vaccine effectiveness against the omicron infection,22 whereas natural immunity was assumed to be lifelong. Accordingly, those in R state were modelled to have lifelong immunity against SARS-CoV-2 infection even after receiving the vaccination.
Then, numerical simulations to quantitatively assess the potential impact of nationwide vaccination were conducted, comparing the number of newly reported probable COVID-19 cases and the prevalence of severe cases in different scenarios via scenario analyses. As the asymptomatic proportion of the population can also influence the effect of nationwide vaccination, the scenarios included different combinations of vaccination coverage with two doses (ranging from 0% to 80%) and asymptomatic proportions (ranging from 30% to 50%). In all scenarios, k was chosen as the best-fit value after comparing the observed and projected incidence via the baseline model (as noted above). When the set proportion of the population was vaccinated with a single dose, the stringent PHSMs were lifted, while the PHSMs placed prior to 14 May 2022 (including personal protective behaviors such as wearing masks) were expected to be maintained (k = 1). In the scenario without nationwide vaccination, the stringent PHSMs were lifted on the same day as the scenario with 50% vaccination coverage (20 July 2022). The averted numbers of probable COVID-19 cases, hospitalizations, and COVID-19 deaths reported from 1 June to 31 October 2022 were also assessed. Based on the median value of each estimated parameter, the cumulative numbers of each epidemiological outcome in scenarios with and without vaccination were compared by varying the vaccination coverage and asymptomatic proportion. R statistical software was used for all of the analyses. The data analyzed in the current study are publicly available.10
RESULTS
The epidemic curve of probable COVID-19 cases in North Korea and the extrapolated incidence with the exponential growth model is shown in Fig. 1. A substantial decrease in the reported case counts was observed from 16 May following the implementation of stringent PHSMs, and the trend is sustained as of 26 May. Based on the exponential growth model assuming constant transmission dynamics over time, the cumulative number of probable COVID-19 cases (Icumul) in North Korea was estimated as 134,491 (95% CIs, 134,489–134,493), as of 11 May 2022.
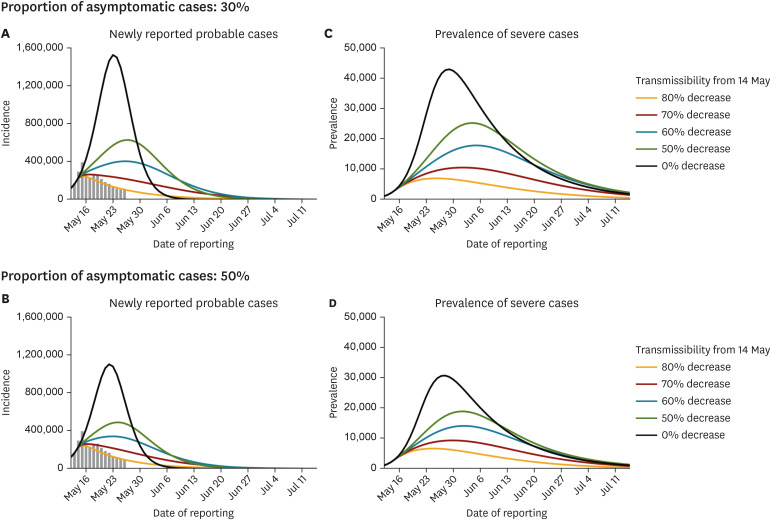
The schematic diagrams of the baseline model and the extended model incorporating nationwide COVID-19 vaccination are shown in Fig. 2. Using the baseline model and assuming a moderate asymptomatic proportion (30%), the reproduction number of COVID-19 under the existing PHSMs in North Korea (prior to the implementation of the stringent PHSMs) was estimated as 3.13 (95% CIs, 3.12–3.13). Despite the limited number of data points and unreliable case counts on 12 May 2022, the reconstructed incidences were mostly in line with the overall trend of observed incidences (Supplementary Fig. 1). Based on the reconstructed transmission dynamics, the impact of the stringent PHSMs (k) on the disease dynamics in North Korea was quantified (Fig. 3). The comparison between the empirically observed and projected incidences of probable COVID-19 cases suggests that the stringent PHSMs reduce the transmissibility of SARS-CoV-2 by more than 80% in North Korea (Fig. 3A and C). The estimated reproduction number and level of reduction were robust over the possible range of asymptomatic proportions (30–50%).
Fig. 3
Quantified impact of stringent PHSMs on SARS-CoV-2 transmission in North Korea. The quantified impact of stringent PHSMs enacted on 14 May 2022 on the SARS-CoV-2 transmissions in North Korea are shown with varied proportions of asymptomatic cases (range 30–50%). (A, B) The number of newly reported probable cases, and (C, D) the prevalence of severe cases are shown. The grey bars show the empirically observed number of newly reported cases (A, B). The colored lines and shaded areas show the projected transmission dynamics of COVID-19 based on different effects of the stringent PHSMs (i.e., the reduction levle in the transmissibility of SARS-CoV-2) and 95% confidence intervals derived using the parametric bootstrap method despite small uncertainties surrounding parameters.
PHSM = public health and social measure, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
The potential effects of nationwide COVID-19 vaccination in North Korea under different combinations of vaccination coverages and asymptomatic proportions, given the 80% reduction in the SARS-CoV-2 transmissibility from 14 May (k = 0.2), are shown in Fig. 4. The projections suggest that nationwide vaccination would be necessary to suppress a huge upsurge in both cases and hospitalizations of COVID-19 following the lifting of the stringent PHSMs. Such resurgences were also observed in scenarios with an asymptomatic proportion of 50%, though the extent of the epidemic shrunk as the asymptomatic proportion increased. This finding highlights the importance of nationwide vaccination to suppress the resurgence of cases and hospitalizations after lifting stringent PHSMs in North Korea over the entire range of potential asymptomatic proportions (30–50%). In addition, it is suggested that vaccinating more than 60% of the population with two doses will allow North Korea to sustain the prevalence of severe cases below the peak value of the current wave (estimated as near 7,000 cases) (Fig. 4B and D). The number of COVID-19-related hospitalizations was projected as less than 1,500 across the entire range of asymptomatic proportions when 80% of the population was vaccinated, highlighting the importance of achieving high vaccination coverage to minimize the infection burden in North Korea. However, small resurgences in incidence were observed even after vaccinating 80% of the population due to waning vaccine effectiveness against the omicron infection. The averted number of incidences, hospitalizations, and COVID-19 deaths in North Korea as a result of nationwide vaccination based on different combinations of vaccination coverages and asymptomatic proportions are shown in Fig. 5. As the asymptomatic proportion of the population decreased (i.e., the number of underreported individuals who developed natural immunity to SARS-CoV-2 decreased), nationwide vaccination greatly reduced all COVID-19 epidemiological outcomes in North Korea.
Fig. 4
Projected impact of nationwide vaccination on SARS-CoV-2 transmission in North Korea. The projected impact of nationwide vaccination on SARS-CoV-2 transmission in North Korea are shown, assuming the stringent PHSMs reduce the transmissibility of SARS-CoV-2 by 80% (k = 0.2), and that the stringent PHSMs will be lifted after a fraction of the population receive at least a single dose of the vaccine. Two epidemiological outcomes are shown by varying both the proportions of asymptomatic cases (range, 30–50%) and the vaccination coverage (range, 0–80%). (A, B) The number of newly reported probable cases and (C, D) the prevalence of severe cases are shown. In scenarios without nationwide vaccination, the stringent PHSMs are modelled to be lifted on the same date as scenarios with 50% of vaccination coverage, and the PHSMs placed prior to 14 May 2020 are expected to be maintained (k = 1). The grey bars show the empirically observed number of newly reported cases (A, B). The colored lines and shaded areas show the projected transmission dynamics of COVID-19 based on different vaccination coverage with two doses and 95% confidence intervals derived using the parametric bootstrap method despite small uncertainties surrounding parameters. The dashed lines show the date when the stringent PHSMs are lifted in each projection.
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, PHSM = public health and social measure, COVID-19 = coronavirus disease 2019.
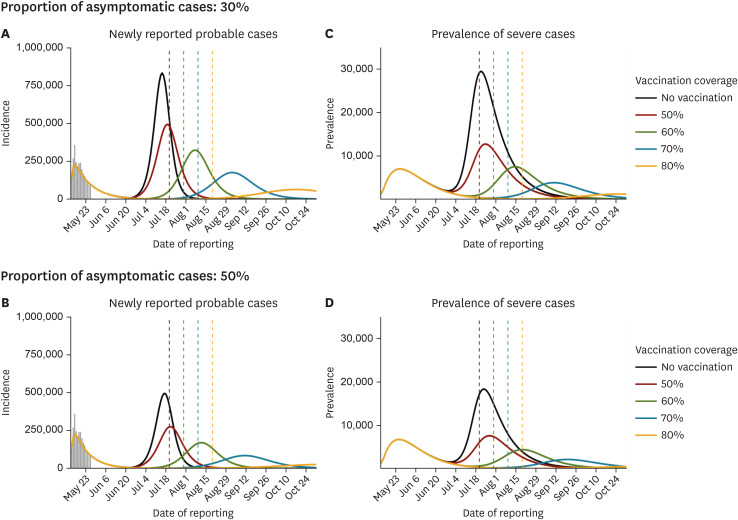
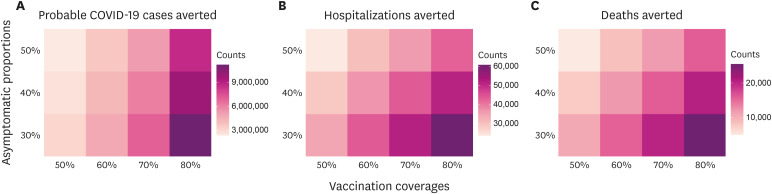
Fig. 5
Averted epidemiological outcomes of COVID-19 following nationwide vaccination in North Korea.
The averted epidemiological outcomes of COVID-19 as a result of the introduction of nationwide vaccination from 1 June to 31 October 2022 are shown. Three epidemiological outcomes achieved by varying both the proportions of asymptomatic cases (range, 30–50%) and the vaccination coverage (range, 0–80%) are shown. (A) The number of probable cases, (B) hospitalizations, and (C) COVID-19-related deaths are shown. The cumulative epidemiological outcomes of each projection are compared with those of the projected outcomes without nationwide vaccination based on the median value of each estimated parameter (i0, r, and β).
COVID-19 = coronavirus disease 2019.
DISCUSSION
In this study, a model-informed approach was used to evaluate the effect of the current, stringent PHSMs in North Korea by varying asymptomatic proportions of the total SARS-CoV-2 infections. Despite very limited data, an 80% reduction in SARS-CoV-2 transmissibility was projected, which is consistent with the observed time series of probable COVID-19 incidence, indicating a significant impact of the stringent PHSMS on the disease dynamics in North Korea. The observed and projected number of COVID-19 deaths was not compared to validate the model because only a total of 63 deaths had been reported from 13 May to 26 May 2022, while the cumulative case counts reached approximately 2.6 million.10 Such low death counts may be underreported due to the high mortality rate related to other conditions in North Korea,23 as well as the right truncation with regard to the time delay from infection to death (of which information is not available).
The findings of this study suggest that nationwide vaccination is essential to suppress a huge resurgence of COVID-19 incidence and hospitalizations in North Korea after the stringent PHSMs are lifted. This result was observed over the entire range of possible asymptomatic proportions (30–50%), and it was primarily caused by the insufficient number of individuals with either natural or vaccinal immunity to achieve herd immunity when the transmissibility of SARS-CoV-2 increased following the lifting of stringent PHSMs. In contrast, the current declining trend in incidence may be maintained even after the intervention period if the proportion of immune individuals via natural SARS-CoV-2 infection reaches the requisite level to develop herd immunity (i.e., 1 − 1/R = 68%, given the estimated reproduction number), as in scenarios with higher asymptomatic proportions than the suggested range in this study. However, despite the lack of COVID-19 testing capability, the actual asymptomatic proportion in North Korea is unlikely to be extraordinarily high (more than 50%) as a certain proportion of infected individuals will develop symptoms, allowing them to be identified as probable cases. In addition, if the stringent PHSMs are lifted once SARS-CoV-2 transmissions reach near-zero levels (the zero-COVID strategy), the size of the epidemic may remain small, unlike the projections based on the deterministic model. Nevertheless, relying solely on such a strategy without immunization is unsustainable given the risks of pre-symptomatic transmission24 and the importation of the SARS-CoV-2 virus from outside North Korea. Indeed, abrupt surges in COVID-19 cases were observed in other countries where the zero-COVID strategy has been implemented (including China and New Zealand) when new SARS-CoV-2 variants with higher transmissibility were imported.56 Moreover, immunizing at-risk individuals allowed those nations to maintain low numbers of hospitalizations and deaths.2526 However, the disease burden following such resurgences may be considerably amplified in North Korea, where the vaccination coverage is known to be zero.
Our projections also suggest that vaccinating more than 80% of the population with two doses may keep the peak prevalence of severe cases in North Korea below 1,500, averting more than 40,000 COVID-19 hospitalizations in all scenarios. The importance of such a reduction in hospitalizations via nationwide vaccination is highlighted in North Korea due to very limited medical equipment and facilities for treating severe cases (e.g., limited oxygen supplies, ventilators, and intensive care units). Due to limited medical resources, excess mortality might be observed when the demand exceeds the available capacity in North Korea,27 and the projections may underestimate the achievable contribution of nationwide vaccination to reduce the number of COVID-19 deaths. However, based on heterogeneities in the risk of death (e.g., a higher risk of death in elderly patients or those burdened by comorbidities), if North Korea allocates vaccines prioritizing those at risk of hospitalization, the reduction in the disease burden can be attained with lower vaccination coverage than the projections suggest.28 A more precise quantitative assessment of such vaccine allocation strategies can be provided when additional information (e.g., age-specific case counts) becomes available by incorporating the age-structured SARS-CoV-2 transmission dynamics into future models.
The resurgence potential of SARS-CoV-2 transmissions in North Korea is not an issue only confined to the country. With waning vaccinal immunity and the emergence of new SARS-CoV-2 variants capable of evading vaccinal immune response (e.g., omicron variants BA.4 and BA.529), some countries with abundant vaccine availability are stockpiling vaccines with plans to conduct additional booster vaccinations. However, large-scale transmissions in countries with low vaccination coverage (such as North Korea) may lead to the emergence of new SARS-CoV-2 variants with a high level of immune escape (even from natural immunity),30 resulting in a considerable global threat to containment efforts until the vaccines are reformulated to specifically target the new strains. Therefore, to avoid such a tragedy, an active interest in planning optimal vaccine allocation should be shared among all nations. Such discussions took place during the COVID-19 Vaccines Global Access (COVAX) initiative co-led by multiple global health organizations.31 Furthermore, the collapse of the healthcare system following overwhelming hospitalizations may increase the potential for new SARS-CoV-2 variants arising. Therefore, not only the vaccine allocation, international cooperation to secure adequate medical equipment and antiviral treatments32 for treating COVID-19 hospitalized cases in low- and middle-income countries will be also important to minimize the risk of global infection burden. Given that the reported vaccination coverage against other infectious diseases in North Korea is comparable to that of other developed countries,33 achieving high coverage with COVID-19 vaccines may not be challenging with international vaccine aid. However, considering a certain ambiguity surrounding the capacity for vaccine allocation, such measures to ensure the resilience of the healthcare system should also be accompanied in North Korea.
Although the extrapolated incidence prior to 12 July was considered to avoid overestimating the reproduction number, it should be noted that the lack of epidemiological data (including the reporting delay) might still lead to an overestimation of the effect of the stringent PHSMs. Nevertheless, it was believed that the suggested approach, which made the best use of available empirical data, was more accurate than relying solely on the reported reproduction number in other countries. The reproduction number significantly varies depending on the epidemiological situation of each country such as the extent to which PHSMs have been implemented and the degree of adherence to interventions. Moreover, such information on North Korea is particularly shrouded in huge uncertainty. In addition, despite this limitation, the proposed model was still able to evaluate the potential effect of nationwide COVID-19 vaccination which is the main objective of the present study.
This study also had some additional limitations. First, the projections fully rely on the reported number of probable COVID-19 cases in North Korea. Underreported SARS-CoV-2 infections in North Korea were accounted for via a plausible range of asymptomatic proportions; however, if the actual value is extreme (higher or lower than the assumed range), the suggested impact of nationwide vaccination on the averted numbers of COVID-19 incidence and hospitalizations may be over- or under-estimated. In addition, it was assumed that the asymptomatic proportion remains constant over time, although it may vary following the abrupt increase in the incidence. Nevertheless, with the available information, this model assesses the overall impact of nationwide vaccination on the disease dynamic in North Korea. Second, it was assumed that there were no large-scale SARS-CoV-2 infections in North Korea prior to the current wave due to the extreme border closures.12 However, if a substantial number of individuals already had immunity to SARS-CoV-2 infection before the current wave, the projected transmission dynamics of COVID-19 and its epidemiological outcomes, especially the numbers of COVID-19-related hospitalizations and deaths, may be affected. Third, the importation of new SARS-CoV-2 with higher transmissibility was not considered. Nevertheless, given the strict border closures and economic isolation, the likelihood of importation was considered to be not significantly high in North Korea. Furthermore, if the higher transmissibility of new variants is mainly driven by the immune escape of new variants, the scenarios with a lower vaccine coverage and that with new variants will produce a similar result as a consequence. Lastly, the suggested effects of COVID-19 vaccination may vary depending on the characteristics of the vaccines, such as their effectiveness against SARS-CoV-2 infections and hospitalizations for each variant. Moreover, there is no available information on the vaccine allocation capacity in North Korea. Thus, it was assumed to be the same as that of Japan,34 given the comparable vaccination coverage against other infectious diseases between the two countries.33 A more precise assessment should be conducted in future studies when additional information regarding each vaccine type, prioritized vaccination groups, and the daily dose of vaccine allocation in North Korea becomes available.
In conclusion, nationwide vaccination would be essential to maintain the suppression of SARS-CoV-2 transmission after lifting the stringent PHSMs in North Korea, especially when a small proportion of all SARS-CoV-2 cases is asymptomatic. Despite limited data regarding COVID-19 in North Korea and unknown asymptomatic proportions, this study highlights the importance of ensuring vaccine accessibility to minimize COVID-19-related hospitalizations and deaths, which would significantly increase the infection burden in countries like North Korea where both vaccinal and natural immunity levels are low.
 XML Download
XML Download