

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Congenital heart surgery (CHS) is technically demanding because of the vital nature of the diseased organ, the wide variability and relative rarity and complexity of the individual pathologies, and the limited surgical access route. CHS requires proficient technical skills and the ability to manage the complex clinical situations before, during and after the procedure, making training extremely complex and challenging. CHS training is fundamentally an apprenticeship in which the relationship between the mentor and the trainee is critically important.1 Technical skill development continues to rely primarily on the traditional “Halstedian preceptorship” format in which trainees are gradually exposed to patients in the operating room under the close tutelage of a senior staff surgeon.23 Although modern training models such as “Zwischenberger model” reinforce training with achievable graduated steps and documentation of the learning activities for certification,45 training of surgical skills for CHS continues to be delivered mostly in the operating room.
CHS training in the operating room has a few important limitations. The trainee’s exposure to surgical cases is primarily based on opportunistic encounters. Importantly, training in the operating room has to be able to produce an ideal surgical result even for a newly appointed surgeon. Therefore, the work that can be assigned to the trainee can vary according to the complexity of the procedure, the patient’s condition and the supervising staff’s willingness to allow the trainee to be the primary surgeon.4 In the modern era of excellent surgical outcomes of CHS, the high public expectation of perfect patient outcomes and the public awareness of the surgeon-specific performance including mortality data further limit the trainees’ opportunities to learn by doing.67 Furthermore, compulsory duty-hour restrictions for surgical trainees have decreased the number of cases performed by the trainees.478910 Consequently, the surgical experience during the CHS training period is widely varied among trainees with experience in complex neonatal surgery being universally limited.11
There is a lack of consensus of the training sequence required before entering the CHS training program including the duration of training and the minimum number of operative cases for certification.611121314 The duration of postgraduate training required to become a congenital heart surgeon varies among countries and ranges between 6–18 years with a median of 10 years.615 The median age of graduation of CHS fellow to certified surgeons was unacceptably high at 40 in the USA.1112 In addition, unexpected societal or worldwide incidents such as the long-lasting pandemic and wars may further compromise the already precarious training opportunities.161718 Due to all these limitations, it is expected that there will be a shortage of eligible cardiothoracic surgeons in the near future.10 Certainly, the advance in surgical techniques and outcomes in CHS has not been accompanied by the simultaneous improvement of the quality and efficiency of CHS training.
An essential component of successful CHS training is the acquisition of skills that are required to independently perform procedures competently with the lowest possible risk to patients. Without improvement of the inefficiency of training, it will remain extremely challenging for trainees to achieve this minimal requirement of training leading to prolonged training periods. In this regard, simulation is considered the best solution to provide trainees with a standardized and safe environment for their skill development.19202122 However, simulation in CHS skill training was very limited until recently when three-dimensionally (3D)-printed replicas or molded models of congenital heart diseases were used for hands-on training of surgeons.23242526272829 In this review article, we discuss the potential values of simulation, the types of simulation platform, the available simulation resources and the future direction of simulation in CHS skill training.
POTENTIAL VALUES OF SIMULATION IN CHS TRAINING
Deliberate practice of procedures outside the operating room will allow the surgeons to efficiently develop their surgical skills in a risk-free environment. Simulation provides trainees with the opportunity to receive interactive instruction and immediate feedback in order to identify their weaknesses and focus future training to resolve them.30 Repeated simulation with defined intervals has shown to maintain skill retention and further improvement of the skills with reduced procedural time.28 By simulating the planned or equivalent procedures in advance, the training surgeons will be able to perform their procedures on patients with a higher level of proficiency and confidence. As a result, the patients’ risk associated with inadequate procedures performed by inexperienced hands can be minimized, the operation room time can be shortened, and the surgical outcomes can be improved. By incorporating well-specified simulation modules into the regular training curriculum, the structured training can be delivered in a form of an efficient, thorough and uniform curriculum with the drawbacks of opportunistic encounters of cases minimized.2028 Simulation training may also be helpful in mitigating the adverse effect of unresolvable limited number of operative cases during training. Simulation training also allows an individualized approach by providing an opportunity to identify those who require additional training.31 Simulation can be used for demonstrating proficiency and objective certification based on the measurable quality indicators.1925 In addition, exposure to simulation of CHS before entering the training program could help candidate trainees to identify their aptitudes for CHS and to make a rational decision about their future career.19 This would improve surgeon retention and prevent CHS trainees from failing at an advanced age of training.61112
BARRIERS TO SIMULATION TRAINING
Kelly et al.32 underwent a survey on thoracic surgery residents’ attitudes regarding the utility of practice, i.e., simulation. The results of the survey demonstrated that the majority of the residents believed that practice outside the operating room was important and improved their operative skills. However, the lack of time, inadequate instruction and unavailability of simulation equipment were major barriers to simulation. In the authors’ program where simulation models for surgical training are available, dedicating training/simulation time into busy work schedules of their trainees is the major challenge to successfully implement these methods.28 Furthermore, objective assessment methods need to be incorporated to facilitate constructive feedback, reduce trainer dependence and promote self-directed learning.33 These barriers can be resolved by standardizing current training curricula and an increase in efforts and funds.
Until recently, CHS training simulators have been scarce and limited mostly to low-fidelity simulators focused on rehearsing basic techniques such as suturing, anastomosis and cannulation. The utilization of 3D printing technology and, more recently, silicone-molding technology has opened a wide door to various CHS simulators.232425262728293435 The authors’ group believe that almost all surgical procedures can be simulated on silicone-molded or 3D-printed models. Currently, a practical barrier might be lack of awareness of the existence and feasibility of available simulator models by both trainees and trainers.
TYPES OF SURGICAL SIMULATION PLATFORM
There are five broad formats of surgical simulators that include: 1) the low-fidelity simulators for basic skill development, 2) the virtual or extended reality simulators, 3) the beating heart simulators, 4) the isolated biological heart simulators, and 5) the 3D replicas of human congenital heart diseases.720
Perhaps most commonly used simulators are low-fidelity synthetic-based simulators used for mastering simple basic skills such as cutting, passing needles through tissue, suturing, knot tying, constructing anastomosis and cannulation.3032
The extended reality simulators using virtual reality, augmented reality and mixed reality technologies can be advantageous over physical simulators as they can be used by multiple users and repeated any number of times with real-time instruction and feedback.3637 However, the user’s perception of the depth on a computer screen or in a holographic space and the tactile sensation can be unrealistic and may result in unforeseen procedural mistakes.20 In general, usable extended reality-based simulators have not yet arrived in the field of CHS. On the other hand, extended reality simulators are useful for catheter-based intervention and assessment of the applicability of the intended or novel procedures or the proof of the concept.3839 Importantly, extended reality simulators are proven helpful in training of video-assisted surgical procedures such as minimally invasive thoracoscopic or laparoscopic surgery and robotic surgery in which the procedures are performed through the extended arms of the instruments that are controlled by the hands of the human user or robot.40 Although extended reality-based simulators have been of limited value and use in CHS, they will continue to evolve in CHS field as have been shown in automobile industry.
The pulsatile biological heart simulators are designed to provide the realistic operating room environment. Most realistic is simulation on live animals in a fully-kitted operating room. It is the highest fidelity training model allowing precision rehearsal of real life.7 The pulsatile heart model can also be set using a sacrificed animal heart. Ramphal et al.41 developed a comprehensive simulation setting in which a heart removed from an animal is placed in a well of simulated pericardial cavity within a mannequin and connected to a computer-controlled mechanical pump. Both settings enable simulation of surgical procedures such as coronary artery bypass surgery, aortic valve replacement and Ross operation on an arrested or beating heart with real-time monitoring of the simulated hemodynamics. Such high-fidelity settings allow realistic surgery in an operating room with superimposition of usual and adverse clinical scenarios. The pulsatile biological heart simulators are expensive, laborious and time-consuming settings, and carry limitations and ethical issues regarding the use of animals.42 Therefore, their availability is limited despite the well-proven strengths.7 Less-comprehensive pulsatile heart simulators can be set for the procedures that are performed on a beating heart such as Blalock-Taussig shunt, coronary artery bypass and mitral or tricuspid valvuloplasty.
The isolated biological heart simulators are the isolated animal or human heart. Although they lack realistic environment including the heart pulsation, blood flow and surrounding tissues, they are applicable for training of some CHS procedures that are performed on an arrested heart. The most commonly used are the animal hearts.43 They are extremely valuable for simulation of the procedures such as coronary artery bypass surgery, Ross operation and arterial switch operation that can be simulated in normal hearts.13 A single heart can be used for simulation of multiple procedures to reduce the required cost. The major limitation of simulation using ‘normal’ hearts is that most CHS procedures cannot be simulated on anatomically normal hearts. Less commonly, human cadavers are used for surgical simulation.44 Anecdotally, innovative surgeons tried their novel procedures on the human pathologic specimens showing the pathology similar to that they would like to treat.
The 3D replicas of human pathological hearts for surgical simulation were introduced in mid 2010s.2324252627282935 Modern medical imaging technologies provide 3D digital information of the human body that can be reconstructed into 3D digital object in various ways according to the purpose of study.45 The acquired image data can also be used for reproduction of the physical models using 3D printing technology. Using the 3D image data obtained from the patients with heart disease, wide variety of pathological hearts can be reproduced. Application of 3D printing technology for reproduction of simulation models has enabled simulation of CHS for various congenital heart diseases, which has long been overdue.13192345 It was regarded that simulation in CHS education had finally arrived with the introduction of 3D printed models.34 CHS specifically benefits from the use of these models due to the fact that the surgery itself is very complex with multiple steps to learn, the access inside the heart is difficult, making the procedures particularly difficult to teach, and that there are so many different conditions to master with considerable variation within each lesion set, all of which are different to many other surgical specialties, even to adult cardiac surgery.
3D MODELING, PRINTING AND MOLDING FOR SURGICAL SIMULATION
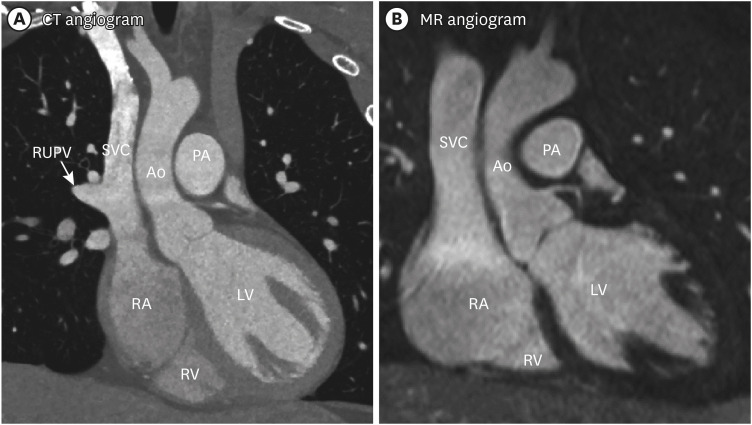
Any modern 3D image data can be applied for 3D modeling and printing. Most useful for 3D modeling are contrast-enhanced computed tomographic (CT) and magnetic resonance (MR) angiograms (Fig. 1). CT provides a high spatial resolution ranging from 0.5–0.625 mm while the practically achievable resolution at MR is 1 mm or larger. Homogeneous contrast enhancement of all parts of cardiovascular system can be achieved with MR, while it is a challenging task in CT. Rotational angiograms obtained during cardiac catheterization can also be used. 3D ultrasound images (echocardiograms) are of limited use due to the abundant artifact from air and bones.
Fig. 1
Contrast-enhanced (A) CT and (B) MR angiograms reconstructed in coronal planes. Both angiograms were obtained by electrocardiographic gating to late diastole. CT angiogram was obtained during breath-holding. MR angiogram was obtained during expiration phase by tracing the diaphragmatic motion using respiration navigation technique. The RUPV in left panel is connected anomalously to the SVC.
CT = computed tomographic, MR = magnetic resonance, RUPV = right upper pulmonary vein, SVC = superior vena cava, Ao = aorta, LV = left ventricle, PA = pulmonary artery, RA = right atrium, RV = right ventricle.
The modelling process can be divided into: 3D imaging, 3D modeling, and 3D printing and molding (Fig. 1).2345 As 3D imaging is the first step of the whole process, the quality of the images is crucially important. To avoid blurring of the images from the motion of the beating heart and respiration, the images are acquired during a short period of cardiac cycle and during sustained breathing or an expiratory or inspiratory phase of the respiration cycle. Imaging during a relatively quiet period of cardiac cycle can be achieved by using electrocardiographic signal. It is important to target late diastole for imaging to closely resemble the arrested heart surgeons are accustomed to at the operating table. The findings at surgery can be significantly different from the findings seen at imaging in systole especially when the ventricles are hypertrophied.
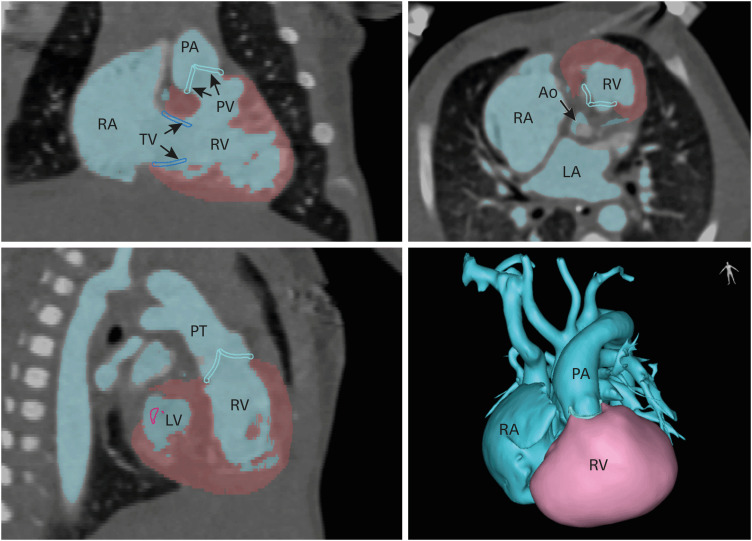
The acquired images are then post-processed for 3D modeling. Using multiplanar reconstruction platform, the regions of interest are extracted by using thresholding (changing each imaging unit [pixel] to black or white pixel by using a threshold signal intensity) (Fig. 2). The process of extraction of the required information is called “segmentation.” As none of the existing imaging technologies are perfect for all cardiovascular structures, the reconstructed images contain insufficient or inaccurate information. Therefore, manual editing by a knowledgeable and experienced observer is essential. For instance, the sites of attachment of cardiac valves are of great surgical importance but are often not clearly defined in reconstructed images. They require manual tracing by an experienced observer. As the cardiac valve leaflets are thin and constantly moving during cardiac cycle, they are hardly definable at CT or MR. Such poorly definable structures by imaging can be graphically designed based on the imaging findings and the operator’s knowledge.45 The designed fake valves are then added to the original heart model. Although such approach should be carefully applied when it is applied for patient management, it is an acceptable solution for surgical simulation. Imaging data fusion can also be used for more complete data set. For instance, the reconstructed images of the cardiac valves at 3D echocardiograms can be extracted and added to the reconstructed CT or MR image data.
Fig. 2
Postprocessing of a computed tomographic images from a neonate with hypoplastic left heart syndrome. The cardiovascular lumen (blue) and ventricular myocardium (brown-pink) were segmented using two different thresholding value ranges. The cardiac valve annuli are traced manually. The bottom right panel shows the three-dimensional volume rendered image of the segmented cardiac structures.
Ao = aorta, LA = left atrium, LV = left ventricle, PA = pulmonary artery, PV = pulmonary valve, RA = right atrium, RV = right ventricle.
The final reconstructed 3D image data are then converted to a file format for 3D printing such as Standard Tessellation Language and Virtual Reality Modeling Language. There are various 3D printing technologies. The choice of a 3D printing equipment for reproduction of surgical simulation models is limited by the physical properties of the available printing materials. Most importantly, the material should be flexible, stretchable and resistant to physical forces such as traction and suturing. The soft flexible print materials that are applicable for surgical simulation are limited. The most applicable among the commercially available print materials in the authors’ opinion and experience are photopolymer resins (Agilus, Tango Plus and Tissue Matrix; Stratasys Ltd, Rehovot, Israel). Although they are far from perfect, the 3D-printed models using various combination of these materials were well received by the users.232425262728 However, it is challenging to find the materials that are highly elastic and yet strong enough when they are exposed to physical forces. Silicones and polyurethane are the chemical materials that provide high elasticity and strength.23294546 Although 3D printing equipment using silicones or polyurethanes have been introduced, its utility for 3D printing of complex structures such as hearts is yet to be proved.
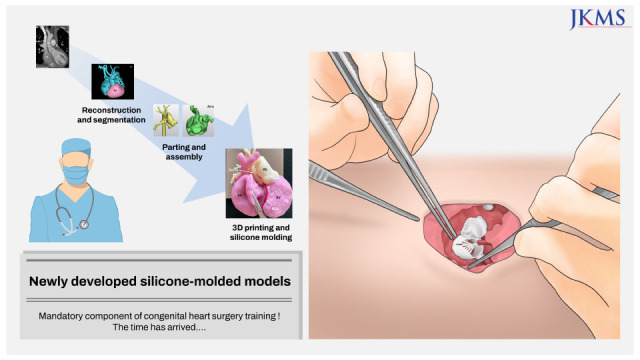
There has been evolution of ideas in using 3D printing technology for the reproduction of CHS simulation models. The latest is applying the molding technique to produce silicone-based models (Figs. 3, 4, 5). Molding is a commonly used technique for both prototyping and mass production. 3D printing allows easy reconstruction of the molds where liquid material (i.e., silicone or polyurethanes) can be infused, which will solidity to the desired shape. Despite these materials having superior mechanical qualities compared to directly printed materials, it has been challenging to use this technology for extremely complex structures such as hearts and its application has been limited to a few investigators.46 The authors’ group recently developed an innovative idea called “parting-and-assembly strategy” in which the heart is divided into multiple parts, each part is molded separately and the molded parts are assembled using adhesive agents.29 By using silicones of different physical properties and colors for the heart muscle, vessels and cardiac valves, the new strategy allowed realistic representation of the heart models and vessels. The models are extremely elastic and highly resistant to physical forces during traction and suturing. The users who used both 3D-printed and silicone-molded models unanimously found that the latter outperforms the former.29 Considering the current limitations of 3D printing technology and print materials, silicone molding will play its major role in fabrication of models for CHS simulation unless the silicone-based 3D printing technology is able to produce the models of comparable or higher quality than silicone-molded models.
Fig. 3
Segmentation of a hypoplastic left heart syndrome model for the Norwood-Sano operation. The segmented cardiovascular system is divided into multiple parts, each part is produced with silicone using molding technique and the molded parts are assembled together with adhesive glue.
PA = pulmonary artery.
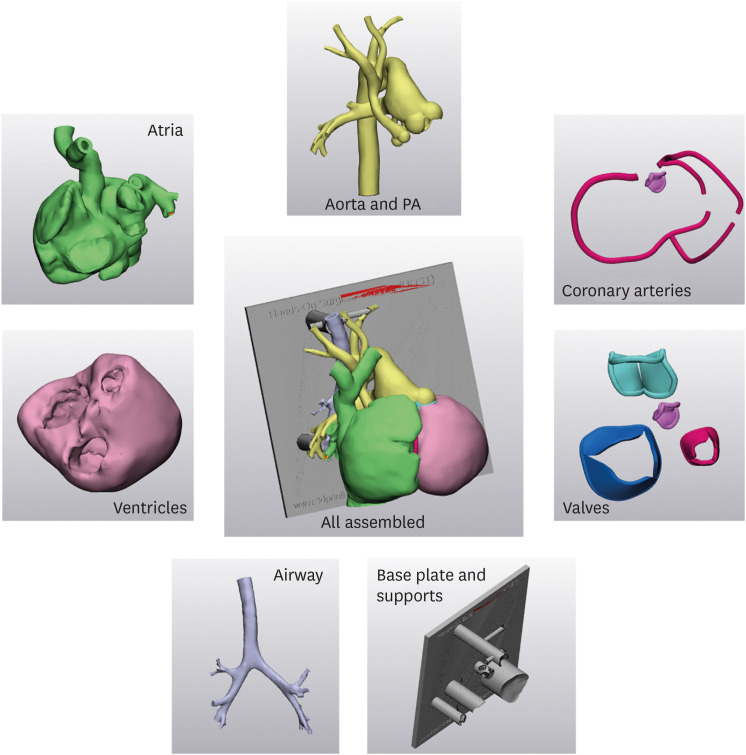
Fig. 4
Silicone-molded model of hypoplastic left heart syndrome (A). (B) The result of the Norwood operation. Severely hypoplastic aorta was reconstructed using the native aorta, main PA and a large surgical patch.
PA = pulmonary artery, RA = right atrium, RCA = right coronary artery, RV = right ventricle.
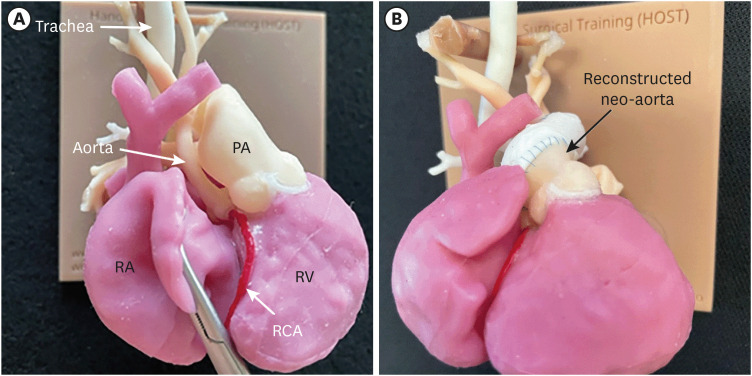
Fig. 5
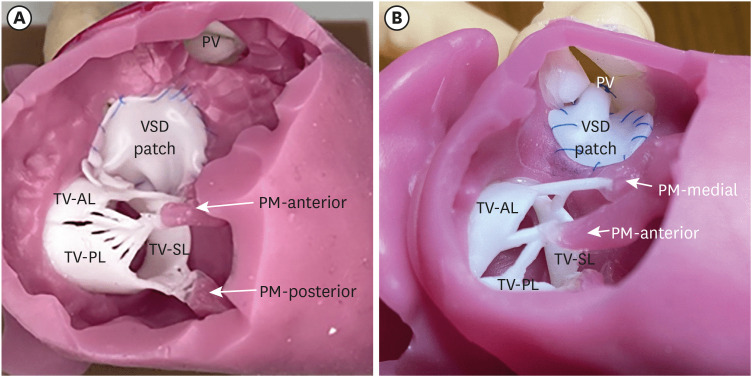
Silicone-molded models for VSD closure. The anterior wall of the right ventricle was removed after the surgical closure of the VSD to show the surgical outcome. (A) Model with a perimembranous type of VSD. The VSD was patch closed from a right atrial approach through the TV. Note that the graphically designed leaflets, chords and PMs are added to closely mimic the surgical scene. (B) Model with a doubly-committed juxtaarterial VSD. The VSD was patch closed through the PV via an incision in the main pulmonary artery.
VSD = ventricular septal defect, TV = tricuspid valve, PM = papillary muscle, PV = pulmonary valve, AL = anterior leaflet, PL = posterior leaflet, SL = septal leaflet.
To provide a realistic environment, a chest-wall operating table simulator can be used (Fig. 6).47 This allows adjustment of the height and pitch-and-roll motion with a suture retraction disc underneath. The simulator is designed to replicate the limited access to the surgical field experienced through a midline sternotomy.
Fig. 6
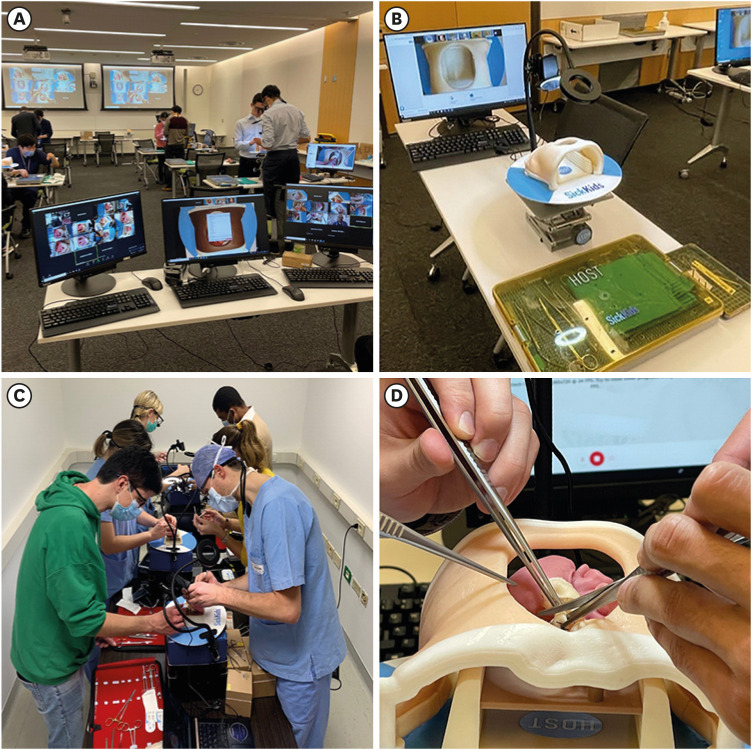
Setting for simulation training for a hybrid in-person and online course. (A) Room setting with multiple operation tables are set for in-person attendees. Each in-person and online attendee’s procedure is monitored by the proctors through a web-camera. (B) Operating table setting. A dynamic chest wall and operating table simulator is set with a surgical light and web-camera for online demonstration and recording. The round disc underneath the chest wall simulator is installed to secure sutures and assist with retraction. (C) A scene of the session in a remote site where the attendees’ performances were remotely proctored online. (D) Surgeons simulating a procedure on a model mounted in a chest wall and operation table simulator.
HANDS-ON SURGICAL TRAINING (HOST) USING 3D-PRINTED OR SILICONE-MOLDED HEART MODELS
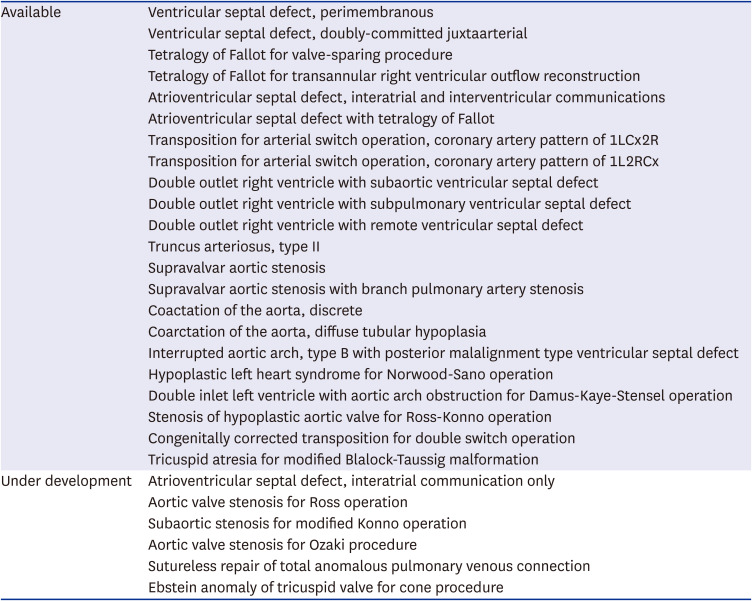
As discussed, there were two breakthroughs in the fabrication of surgical simulation models for CHS training. The first was the utilization of 3D printing technology using patients’ image data in 2015 and followed by the introduction of the parting-and-assembly strategy for silicone molding in 2020. Since 2015 when the 95th American Association of Thoracic Surgery organized the first HOST session using 3D-printed models for CHS training, international HOST courses have been organized annually at the authors’ institution and sporadically in other institutions in USA and Asia.23242526272829 In the first 5 years, 3D-printed models were used for all HOST courses and from 2020 silicone-molded models have been exclusively used. Both the attendees and proctors appreciated that the models are highly acceptable for surgical simulation and that the courses are immensely helpful for development of surgical procedures. The authors’ institution has incorporated monthly HOST sessions in the curriculum of CHS fellowship training program since 2019.28 The available models include those for simple procedures such as patch closure of ventricular septal defects and those for complex CHS such as arterial switch operation for transposition of the great arteries and Norwood-Sano procedure for hypoplastic left heart syndrome (Table 1).
Table 1
List of silicone-molded simulation models for congenital heart surgery
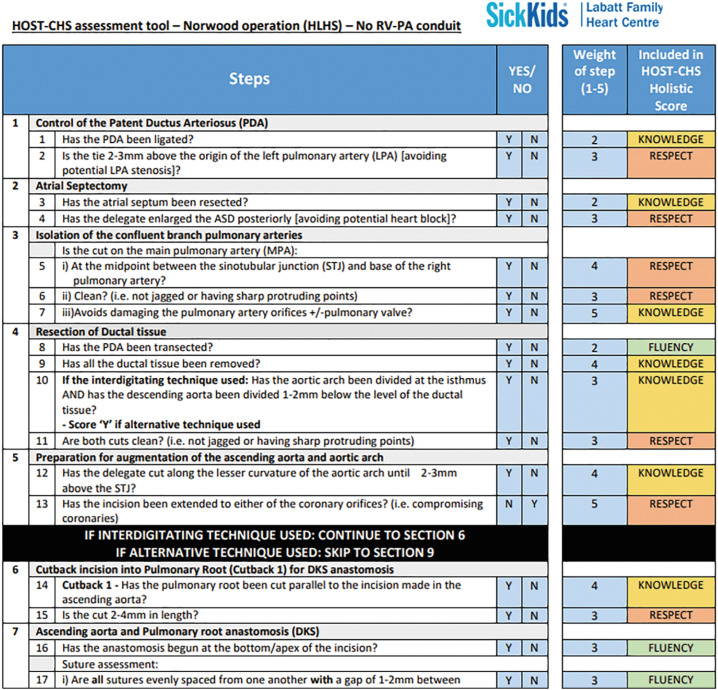
While simulation training of CHS is obviously helpful in surgeons’ skill development, its impact may vary among trainees. Therefore, the impact of HOST should be evaluated objectively and quantitatively for the individualized constructive feedback and also for the accreditation process for standardization and regulation of the training program. The trainees’ procedures are assessed for improvement of the technical performance and surgical procedure time. The HOST-CHS assessment tool is a newly developed procedure-specific checklist that is designed to objectively assess the technical performance of each step involved in the index procedure (Fig. 7).25 Each step is scored as either successful or unsuccessful (i.e., yes or no). To help discriminate between importance of each task, all steps have a pre-defined weighted score based its importance using a Likert 1–5 score (5 = high importance, 1 = low importance). The evaluation using HOST-CHS assessment tools has proven to be consistent among evaluators of different experience including non-medical doctors, surgeons in training and established proctor surgeons.25 For assessment by the proctors or other evaluators, the trainees’ procedures were recorded either through a camera mounted on the operating table or a head camera. A table-mounted camera is excellent for extracardiac procedures such as arterial switch operation or arch reconstruction surgeries, while a head camera is required for predominantly intracardiac procedures such as patch closure of a ventricular septal defect. The use of a head camera requires steady positioning of the operator’s head, which is challenging.
Fig. 7
HOST-CHS assessment tool for evaluation of Norwood operation simulation. The tool lists the surgical steps that can be reproduced on the three-dimensional-printed or molded model. Each step is assessed whether it was successful (yes) or unsuccessful (no). All steps have a predefined ‘weight’ based on its importance to the overall procedure using a Likert scale (1 to 5) with 5 implying the highest importance and 1 implying the least importance. Each step was categorized into one of three holistic categories that include: 1) fluency of the procedure, 2) knowledge of the technical aspects of the procedure, and 3) respect of tissue during the procedure.
HOST-CHS = Hands-On-Surgical Training-Congenital Heart Surgery.
The authors’ data demonstrated objective improvement in surgical time and technical performance at the second HOST attempt for the arterial switch operation and Norwood operations,2627 which may apply for any CHS procedures.28 What matters is how many attempts are required to master the individual procedures and how much the acquired skills will be retained after a certain period of interval. With further clarification of such unknowns, training curriculum will be able to be optimized for efficient and cost-effective training.
HOST can also be utilized for rehearsal of the procedure before a trainee takes the primary operator’s role on an elective surgery.48 If the patient’s 3D image data are available, a replica can be 3D-printed for trainee’s rehearsal. If the patient’s image data are not available, a replica of a heart with similar pathology can be reproduced for rehearsal. Practicing the procedure in a risk-free non-stressful environment provides an ample opportunity to master the procedure before doing the procedure on the patient and, therefore, improves the surgical outcome and minimizes patient risk.
Simulation is also an ideal way to develop and evaluate novel surgical approaches. By simulating the novel procedures on models, the surgeons may improve their surgical skills and identify potential shortcomings or complications before applying the procedures on the patients.19 Similarly, simulation can be used for the development and testing of new devices. Simulation of the new procedures could permit improved dissemination of the technology and cross-fertilization of the ideas between centers as well as individual surgeons.
FUTURE DIRECTIONS
Although a variety of surgical simulation models are available, there are a few unexplored areas that include repair of the pulmonary venous pathologies using a sutureless technique and cardiac valve repair such as cone surgery for Ebstein anomaly of the tricuspid valve, and aortic and mitral repair techniques. Despite that both pericardium and cardiac valves are the most difficult structures to reproduce using patients’ image data, they can be simulated using computer-aided design.
The 3D-printed or silicone-molded models are for simulation of the arrested, bloodless heart surgery on cardiopulmonary bypass. For off-pump beating heart surgery such as coronary artery bypass, modified Blalock-Taussig shunt and aortic arch reconstruction, the models should be connected to a mechanical pump by which a pulsatile flow is generated to flow through the target structure.49 Such flow-circuits could potentially be used to pressurise hearts to test adequacy of repairs.
The surgical procedures can be broken down into essential components and partial-task training models can be developed at a low cost for training of the fundamental skills such as vascular anastomosis, augmentation of the stenotic vessel and patch closure of a defect.43 Low-cost models for such limited component task training will help the early-career surgeons to master their dextrous hand and finger motions.21
Silicone molding using “parting-and-assembly” strategy is a time-consuming, labor-intensive and expensive process.29 The cost will gradually be reduced with disseminated use of models. On the other hand, silicone-based 3D printing may eventually be available for direct printing of the models with silicones of different physical properties and colors.
3D-printed or silicone-molded models is now mature enough to be used routinely during CHS training. With further evidences of the impact of HOST in CHS, the organizations governing the training and certification of congenital heart surgeons are expected to recognize the HOST as an essential component of training. Similar to the mandates of simulation training for every pilot in aviation industry, completion of simulation training will ideally and ultimately be required for every surgeon to perform surgical procedures on patients.
The individual surgeon’s HOST is only a component of required simulation training. Ultimately, team simulation is required for integration of the roles and skills of the surgical team including the surgeons, nurses, perfusionists, anesthesiologists and other supporting staffs and also for management of various forms of crisis.1922
CONCLUSION
The benefits of surgical simulation in training of CHS are well known and undisputable. One of the major barriers to surgical simulation training was the lack of adequate surgical simulation models and equipment. Recently, this major barrier has been broken. Silicone-molded models for simulation of various CHS procedures are now available and readily usable. The time has arrived when all congenital heart surgeons and training programs should consider completion of formalized surgical simulation training before progressing to real-life operating in a similar fashion to the aviation industry where all pilots are required to complete simulation training before flying a real aircraft. Simulation training is not an option anymore but should be a mandatory component of CHS training.
 XML Download
XML Download