

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ankle fractures are among the most common injuries that currently account for 10.2% of all bone injuries.1 Between 2015 and 2018, ankle fractures were reported in the Swedish Fracture Register as the third most frequent fractures after wrist and hip fractures and recognized as the fifth most common type of bone fracture by Court-Brown et al. in the UK.23 Moreover, these fractures often necessitate surgical intervention that may result in substantial morbidity, including post-traumatic arthritis, infection, failure of fixation, reoperation, and potential mortality.45
Ankle fractures can result from various injury mechanisms, including falls, sports, exercise, jumps, and others.67 The overall incidence of ankle fractures has been reported in many population-based studies or among studies with selected patient groups, and varies from 42.2 to 187/100,000 person-years.1234789101112131415 A burgeoning increase in the incidence of ankle fractures, particularly in older women, has been recently reported.81012131416
Although ankle fractures are quite common, most reported studies include a limited number of patients, mostly from single hospitals or limited areas or selected patients (surgically treated, hospitalized, or of a specific age group). These factors limit the generalizability of the results to the national population. A few nationwide population-based studies have investigated selected groups who visited the emergency department or only hospitalized patients.610 The nationwide population-based epidemiologic data of ankle fractures is scarce in the literature.
This study aimed to provide epidemiologic information on ankle fractures in the nationwide population for a period of a decade, including incidence by age groups, seasons, fracture subtypes, and trends over time in South Korea.
METHODS
Data source
South Korea has a universal health care system in which the Korea National Health Insurance (KNHI) operates a mandatory health insurance program and provides health insurance coverage to approximately 98% of the citizens.17 All patients’ data were extracted from the Health Insurance Review and Assessment Service (HIRA). The HIRA manages and stores medical information data submitted by medical institutions for compensation in the electronic record format. The database provides information about unselected populations representing the entire spectrum of disease extent and severity. This database contains general and sociodemographic information, specific health care services, outpatient prescriptions, and diagnostic information based on the Korean Classification of Disease, 7th revision (KCD-7).18
Patient identification
Injury diagnoses were registered according to the KCD-7, primarily constructed based on the International Classification of Diseases, 10th revision of the World Health Organization (ICD-10), and classified according to their anatomic region. Ankle fractures were identified in the monthly data of outpatients and inpatients with diagnostic codes S82.5, S82.6, and S82.8 according to the KCD-7, representing the ankle fractures. S82.5 represents fractures of the medial malleolus, S82.6 represents fractures of the lateral malleolus, and S82.8, including subgroups of S82.82 and S82.83, represents bimalleolar fractures and trimalleolar fractures. The diagnostic codes for specific ankle fracture locations are summarized in Supplementary Table 1.
We removed all records except for the date at the initial diagnosis of ankle fractures to avoid data duplication. Patients diagnosed with ankle fractures in 2008 were excluded because their data were collected prior to the study period. The observation period of our study was 10 years (2009–2018) after excluding a washout period of 1 year (2008). A total of 869,024 patients were selected, of whom 794,312 patients were included in the study (excluding those in 2008).
Statistical analysis
To calculate the overall incidence rate, the data of the entire study population including the year at diagnosis, age, and sex were obtained from the National Statistical Office’s website (http://kostat.go.kr/).
To determine the factors affecting the patients’ incidence rates, we considered the year at diagnosis, age, sex, type of ankle fracture, and season. The incidence rate was calculated as the number of patients with ankle fractures divided by the total population. The population data were analyzed according to year at which diagnosis was established, sex, and age. Data pre-processing and analysis were conducted using the SAS Enterprise 6.1 guide program.
Ethics statement
Personal data provided by HIRA was de-identified because the entire database was encrypted by altering the identifiable personal information. The study protocol was approved by the Institutional Review Board (IRB) of Hallym University Dongtan Sacred Heart Hospital (IRB No. 2020-03-020). No informed consent was required from patients due to the nature of public data from HIRA.
RESULTS
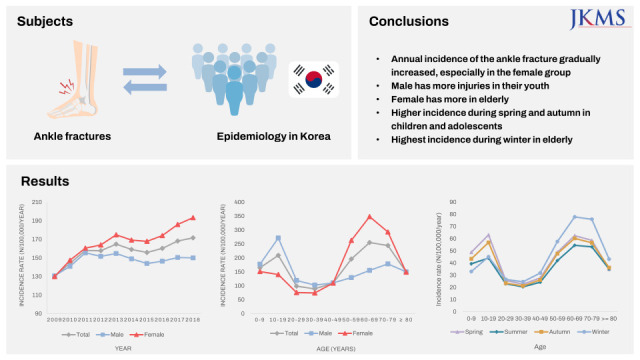
Trends in annual ankle fracture incidence rates: Annual incidence of ankle fracture gradually increased, especially in the female group
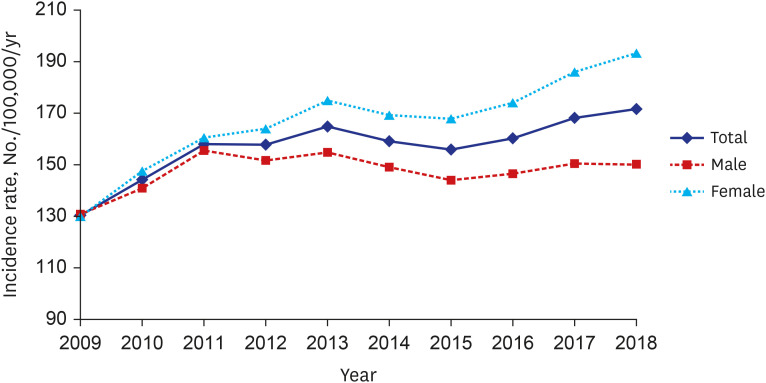
The annual and age-adjusted incidence rates of ankle fractures per 100,000 persons are summarized in Table 1. The mean incidence rate of ankle fractures between 2009 and 2018 was 159.2/100,000 person-years. The incidence rate was 149.9/100,000 person-years for males and 168.4/100,000 person-years for females. The overall incidence rate increased from 130.4/100,000 person-years in 2009 to 171.6/100,000 person-years in 2018. The incidence rate of ankle fractures in males fluctuated around 150, whereas in females, it tended to increase gradually. The incidence rate in females was higher than that in males, and this difference increased over time. An increasing trend in the incidence and differences between sexes is shown in Fig. 1.
Table 1
Annual incidence and age-adjusted incidence of the ankle fracture per 100,000 persons in South Korea
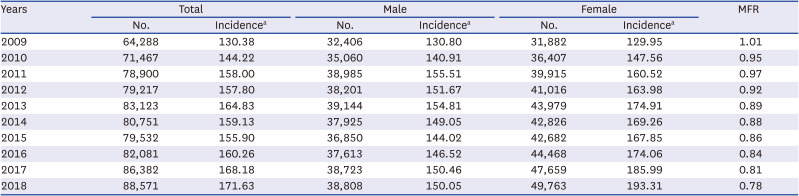
Fig. 1
The incidence rates per 100,000 person-years of ankle fracture in South Korea during 2009–2018, stratified by sex and year. The figure corresponds with Table 1.
Changes in ankle fracture incidence rates according to age and sex: Male has more injuries in their youth, and meanwhile, female has more injuries in older ages
Table 2 shows the mean incidence rates of ankle fractures between 2009 and 2018 according to age and sex. For 60-year-old females, the incidence rate was 348.19/100,000 person-years. This was the only incidence rate over 300, and was the highest among all age groups for both males and females. There were 420,597 (53.0%) females and 373,715 (47.0%) males. The overall incidence rate showed bimodal peaks in adolescents and patients in their 60s. The incidence rate according to age is depicted in Fig. 2 and shows a clear difference between both sexes. The incidence rate in the male group reached a peak in the adolescent period.
Table 2
The number of patients with ankle fractures and incidence rate according to age and gender
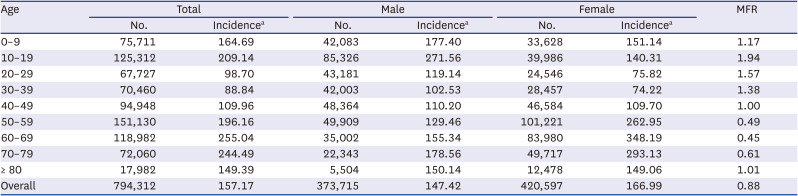
Fig. 2
The incidence rates per 100,000 person-years of ankle fracture in South Korea during 2009–2018, stratified by age and sex. The figure corresponds with Table 2.
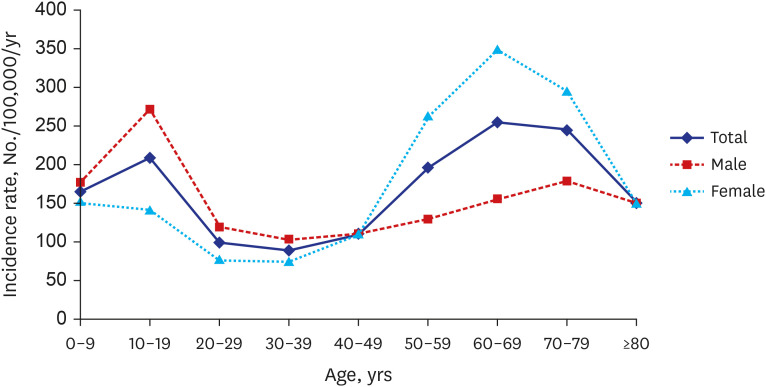
In contrast, the incidence rates in females peaked among the 60 years age group. With increase in age, the incidence rate in males increased relatively slowly, whereas that in females more than doubled. Males of 40 years of age had a higher ankle fracture incidence rate as compared to females. There was little difference between males and females in their 40s. On the other hand, the incidence rates in females rose drastically after their 50s.
Ankle fracture incidence rates by fracture subtype: Isolated lateral malleolar fracture was the most frequent injury pattern
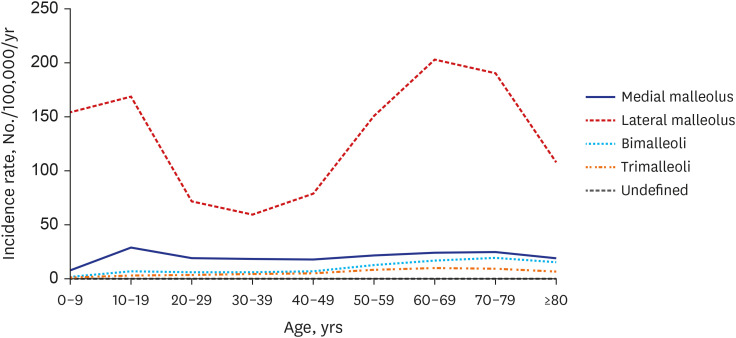
Table 3 shows the distribution of the ankle fracture types over the years. Lateral malleolar fractures are the most common type, accounting for 77.58% of all ankle fractures. The distribution of fracture types by age group is shown in Fig. 3. Lateral malleolar fractures were predominant among all age groups. The incidence rates of the medial malleolus, bimalleolar, and trimalleolar subtypes were similar among different age groups. In contrast, the lateral malleolar fracture incidence rate was noticeable in adolescents and older adults.

Ankle fracture incidence rates according to month and season: Children and adolescents showed the highest incidence during spring and autumn. Meanwhile elderly showed the highest incidence during winter.
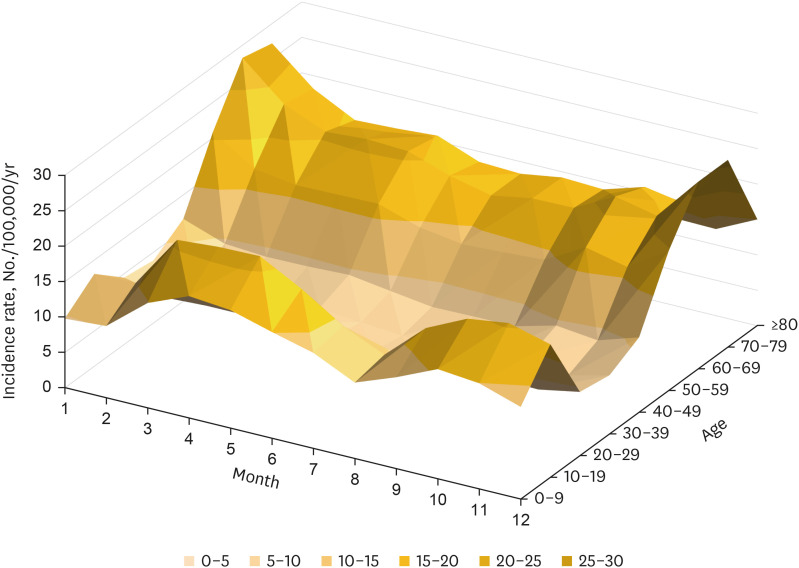
The incidence rates of ankle fractures according to age and month is shown in Fig. 4. In the age group below 20 years, the monthly incidence rates showed a bimodal distribution in spring and autumn. During winter however, the monthly incidence rates followed a unimodal peak among older adults. In adults in their 20s to 40s, the incidence rate was the highest in winter, but the seasonal difference was minimal. The incidence rate in the 20–40 years age group was significantly lower than that in children, adolescents, and older adults. The seasonal variation in ankle fracture incidence rates is shown in Supplementary Fig. 1.
DISCUSSION
Previous epidemiological studies on ankle fractures have been conducted in the United States, Switzerland, Sweden, Denmark, Finland, and Scotland.368910121619 Although these studies investigated the epidemiologic data of ankle fractures and included few population-based studies, the entire populations in the respective countries were not considered. The present study reported an incidence rate of 159.2/100,000 person-years among a non-selected patient group with ankle fractures. Moreover, this rate was considerably higher than that reported by Thur et al.10 (71/100,000 person-years in the Swedish National Patient Register between 1987 and 2004). Scheer et al.6 reported a notably low incidence rate of 42.2/100,000 person-years using the data between 2012 and 2016 provided by the National Electronic Injury Surveillance System (NEISS). These results might be underestimated owing to the characteristics of the study population that included either the hospitalized patients or those who visited the emergency department. However, we believe that our data accurately reflect the ankle fracture trends in South Korea as a whole, considering the characteristics and patient population of our study.
Other non-population-based epidemiologic studies included limited number of patients and were confined to either selected age groups, estimated population sizes, specific hospitals, or specific regions. Moreover, none of the studies explored nationwide population-based data from nonselected patients. Court-Brown et al.1 reported an overall ankle fracture incidence rate of 100.8/100,000 person-years in 2000 and 137.7 in 2014 in Edinburgh, among patients aged > 15 years. Daly et al.13 reported an overall incidence rate of 187/100,000 person-years from 1979 to 1981 in Rochester, Minnesota, the United States, using an estimated population size, with the sample size being limited to a hundred patients. Elsoe et al.8 reported an incidence rate of 168.7/100,000 person-years at the Aalborg University Hospital in Denmark in North Denmark from 2005 to 2014. Their findings were similar to those reported by Court-Brown et al. Juto et al.9 disclosed an incidence rate of 179/100,000 person-years in Norbotten County in Sweden from 2009 to 2013, excluding patients under 20.
Our results are similar to those of previous studies and show an increasing trend in the incidence rates of ankle fractures among the aging population.8101216 We believe that aging itself is a significant cause of a relatively high incidence of ankle fractures in our study population. Most studies were limited to a short period of time and the long-term trends were not addressed. However, the present study reported incidence rates spanning over the period of a decade and showed significant year-to-year changes, with an overall weak trend in incidence rates increasing from 2009 to 2018. South Korea’s population is rapidly aging. In fact, the population aged 65 years increased from 10.6% in 2009 to 14.8% in 2018. It is expected to surpass 20% in 2025 and 40% in 2050.20
The incidence rate according to age followed a bimodal distribution. When examining the incidence rates within each sex category separately, the difference in the incidence rates according to age showed a stark contrast. The incidence of ankle fractures in males showed a unimodal peak during the adolescence period and then slowly increased with age. On the other hand, in women, the incidence rate decreased during the period extending from adolescence to the 20s and 30s, then rose sharply after the 40s, reaching its peak in the 60s. The increase in the incidence of ankle fractures was most pronounced in women over the 60s. A study by Kannus et al.12 found a 164% increase in the number of women aged ≥ 60 years who have experienced ankle fractures between 1970 and 2000. These findings are significant because they indicate an increased risk for ankle-related osteoporotic fragility fractures in women.
The literature shows that ankle fractures predominate in adolescent males and older adult females. These findings are in accordance with the results of our study. Court-Brown et al.1 also reported a unimodal distribution for both sexes, with peak incidences in adolescent males and old females. Thur et al.10 and Elsoe et al.8 showed a similar incidence pattern, with incidence rates in the male group peaking in the adolescent period and peaking in the female group in the 60s age group. However, the results of this study showed a decreasing trend among men. According to Scheer et al.,6 males reported nearly twice as many ankle fracture incidents as compared to females during the adolescent period. Similarly, Juto et al.9 and Thur et al.10 reported a doubling of the incidence of ankle fractures in females in their 60s as compared to males. As compared with the results of our study, Juto et al.9 showed a similar trend in ankle fracture incidence rates according to sex and age, and high incidence rates were observed among men until their 30s. In addition, Juto et al.9 showed similar incidence rates for men in their 40s. As for women, the ankle fracture incidence rates started to outpace from their 50s, peaking in their 60s, and amounted to more than double the incidence rates of men in that same age group.
The most common fracture type in all age groups was a fracture of the lateral malleolus, accounting for 77.6% of all fractures. Elsoe et al.8 and Hasselman et al.21 also reported that lateral malleolar fractures are the most common fracture subtype accounting to 57.6%. However, the lateral malleolar fractures accounted for 55% of all ankle fractures in our study. The overestimation of isolated lateral malleolus fracture rates in our study could be explained by the type of data used in our study. In fact, the data used are not clinical but are rather data for insurance claims that did not distinguish metaphyseal fractures from avulsed or “chip” fractures. Although the distribution of specific fracture subtypes varies between our study and previous studies, most investigators agree that the lateral malleolar fractures are the most common fracture subtype.81316
Although few studies have reported seasonal differences in the incidence rates of ankle fractures, none of the studies reported seasonal differences in ankle fracture incidence rates stratified by age. Juto et al.9 reported a difference in the frequency of ankle fractures throughout the year, with a peak incidence rate occurring in December. Elsoe et al.8 also reported seasonal and monthly variations with a peak incidence in January. Their results showed a considerably high number of ankle fractures during the winter of 2010 and 2011, which was unusually cold and snowy.
Similarly, in January 2011, an extreme cold snap and 100 year record-breaking heavy snowfall occurred in South Korea. In December 2012, there was more than twice as much snowfall as in the same month of the previous year.22 The incidence rate of ankle fractures was exceptionally high during the study period. Cold winters and heavy snowfall might have increased the risk of ankle fractures.
The bimodal distribution in spring and autumn incidence rates in school-age adolescents and children is thought to be due to increased outdoor activities as the school and kindergarten semesters begin.
The present study had some limitations. First, the quality of the HIRA database was controlled by the register and not by physicians. The diagnostic codes representative of specific fracture subtypes did not take into account the mechanism of injury, as proposed by the widely used Lauge-Hansen classification system. Although diagnostic codes S82.5, S82.6, S82.82, and S82.83 indicate the location of the fracture in the ankle, they do not classify various fracture types according to the injury mechanism. Therefore, the data used in this study could not be used to determine whether a surgical procedure was necessary.
Second, it is difficult to differentiate between actual rotational ankle fractures and avulsion or "chip" fractures. In fact, both these types are included in our study as in other population-based studies using data from state institutions. This is especially true for the lateral malleolus fractures, which may be overestimated.
Despite the limitations, our study had certain strengths. The National Health Insurance provides health coverage to 98% of the total population in South Korea. Therefore, this study investigated the largest number of ankle fractures published to date, representing nearly the entire population of the country. Almost all ankle fractures occurring in South Korea were considered, targeting all populations rather than being limited to a specific region, hospital, or age group. To our knowledge, this is the first long-term epidemiological study of ankle fractures in South Korea.
In conclusion, this study showed a mean incidence rate of 159.2/100,000 person-years spanning a period of a decade in South Korea. The incidence of ankle fractures increased over the 10-year study period from 2009 to 2018, especially in older women. Our results showed significant differences in ankle fracture incidence rates between men and women. Among men, the highest incidence rate was during the adolescent period, with a relatively even distribution among other age groups. In contrast, the incidence rates in females gradually increased with age. Lateral malleolar fractures were found to be the most common fracture subtype in all age groups accounting for 77.6% of all fractures. In children and adolescents, fractures occur more frequently in spring and autumn, whereas those in older adults occur mostly in winter.
 XML Download
XML Download