

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) pandemic, declared by the World Health Organization in 2020, continues.1 Several effective vaccines have been developed against COVID-19, but the new omicron variant is more transmissible than the delta variant as well as increased immune escape.23 The number of confirmed COVID-19 cases increased markedly after the emergence of the omicron variant in Korea, even though the vaccination completion rate exceeded 80% in December 2021.4
In a previous study, we reported that the incidence rates of COVID-19 infection in the Korean military were lower than those in the general Korean population, due to mass vaccination of COVID-19 conducted from July 2021 to early August 2021.5 However, after the omicron variant became dominant in January 2022, the number of confirmed COVID-19 cases skyrocketed among military personnel, as it did among Korean civilians. During this period, to prevent the spread of the disease, the military maintained strict non-pharmacological interventions (NPI), such as performing proactive real-time reverse transcription polymerase chain reaction (PCR) testing and applying prolonged isolation guidelines. Further, mass vaccination with a third dose of COVID-19 vaccine was performed in December 2021.
In this study, we analyzed the trend in the daily number of confirmed COVID-19 cases before and after the outbreak of the omicron variant on December 5, 2021 among the Korean military in a setting of intensive NPI and mass booster vaccination.
METHODS
Study design
Epidemiological data of confirmed COVID-19 cases in the Korean military were collected from September 1, 2021 to April 10, 2022. The change in trend in the daily number of newly confirmed COVID-19 cases was analyzed using November 1 and December 5, 2021 as reference dates. November 1, 2021 was approximately 3 months after the end of administering the second dose of COVID-19 vaccine in military. Additionally, it was the time when the third dose of vaccine could be administered, according to the guidelines of the Korea Disease Control and Prevention Agency (KDCA) in relation to the waning of the protective effect of the vaccine against symptomatic COVID-19.6 December 5, 2021, was the first day of the week on which the first case of the omicron variant was detected in the Korean military.
The trends in daily number of newly confirmed COVID-19 cases in the Korean military and in the population of Korean civilians adjusted to same population with the military are compared. The vaccination status of each confirmed COVID-19 case in the military was reviewed, and the change in the proportions of the status among confirmed cases were also checked.
Definitions
As of September 2021, 567,062 military personnel were on active duty as officers and soldiers in the Korean military. According to previous research about immunity waning after vaccination,7 if less than 3 months had passed since the second dose of vaccine (one dose for the Ad.26.COV2.S vaccine) or after the booster vaccination, individuals with confirmed COVID-19 were classified as “fully vaccinated.” Conversely, if more than 3 months had passed since the primary vaccination, the cases were classified as “not adequately vaccinated.”
Diagnostic tests for COVID-19 and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants
Diagnosis of COVID-19 and variant testing was conducted in both the Korean military and civilian laboratory institutions, and detailed methods are described in Supplementary Data 1. Confirmed COVID-19 cases were diagnosed by PCR testing of respiratory specimens, approved by the Ministry of Food and Drug Safety of the Republic of Korea.8 From March 14, 2022, rapid antigen testing was also approved for confirmatory testing in the military and individuals with a positive rapid antigen test result were regarded as confirmed COVID-19 cases. The 2 variant tests in the military were conducted by the Armed Forces Medical Research Institute and were performed on mean 16 samples (standard deviation 13) per week randomly selected from samples of military personnel with confirmed COVID-19.
Vaccination strategy in the Korean military
The major events, including mass COVID-19 vaccination are summarized in Fig. 1. After the second dose of vaccine (June 26 to August 6, 2021), 85.730% of military personnel were fully vaccinated by September 15, 2021. The exact vaccine coverage was not monitored after the end of vaccination program, but the vaccination coverage continued to increase due to a strong vaccination incentive policy. Non-vaccinated personnel were required to have weekly PCR tests, and were disincentivized by various quarantine guidelines, including leave. New recruits were strongly recommended to undergo vaccination before joining the military camps. However, because this recommendation was not well followed, and cluster infections occurred among unvaccinated soldiers, vaccination of trainees was started in the camps on September 27, 2021.
Fig. 1
Timeline of COVID-19-related events in the Korean military, including the mass vaccination program.
COVID-19 = coronavirus disease 2019.
aMilitary personnel who received the first dose of ChAdOx1 nCoV-19 vaccine were given a second dose of ChAdOx1 nCoV-19 or BNT162b2 vaccine, depending on the individual’s choice. Excluding the untracked units under the direct control of the Ministry of National Defense, which make up 4.4% of the military, mass vaccination was performed as follows: ChAdOx1 nCoV-19, 0.67%; BNT162b2, 78.12%; Ad.26.COV2.S, 0.57%; and heterologous vaccination (ChAdOx1 nCoV-19 followed by BNT162b2), 20.64%.
bAll military personnel received the BNT162b2 vaccine as the third dose of vaccine. Individuals who were vaccinated in civilian institutions were considered as having missing data.
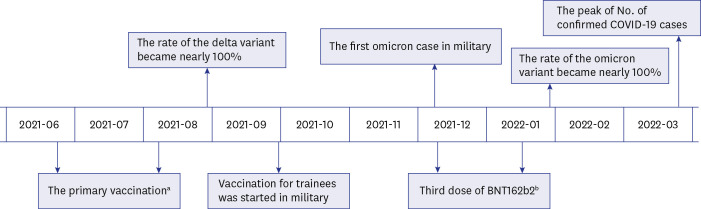
After the booster vaccination (December 6, 2021, to January 14, 2022), 62.216% of military personnel received a booster dose of the BNT162b2 vaccine by January 14, 2022. The military strongly recommended a booster vaccination if more than 3 months had passed since the primary vaccination, and after 6 months without a booster vaccination, personnel were treated the same as those who had not been vaccinated.
NPI in the Korean military
The strict NPI strategy in the military is detailed in Supplementary Data 2. Periodic PCR tests were not performed on asymptomatic personnel, but non-vaccinated personnel were required to have weekly PCR tests as part of the vaccination incentive policy. Personnel had to undergo 2 PCR tests if they had had close contact or shared an area of activity with individuals with confirmed COVID-19. Thus, if 1 case was confirmed, it often caused more than 1 battalion to be tested. For individuals with confirmed COVID-19, the isolation period was 14 days, which was longer than the 7 days of the KDCA guidelines.
Statistical analysis
The trend in the daily number of newly confirmed COVID-19 cases in the Korean military was analyzed using segmented regression analysis of interrupted time-series.9 Statistical significance was set at P < 0.050. Level change is a difference in the absolute value of confirmed cases, and the difference in trends was shown as the trend change. If the trend change was positive, there was a statistically significant increase based on the reference date. The detailed methods of analysis and modeling are described in Supplementary Data 3. All statistical analyses were performed using R version 4.2.0 (R Core Team, Vienna, Austria).
RESULTS
Daily number of confirmed COVID-19 cases in the Korean military before and after the emergence of the omicron variant
The daily number of newly confirmed COVID-19 cases in the Korean military is shown in Fig. 2. A statistically significant increase trend for COVID-19 occurrence after emergence of the omicron variant was observed (regression coefficient, 23.071; 95% confidence interval [CI], 16.122–30.020; P < 0.001). Soldiers accounted for 51.800% of the confirmed cases during the study period. However, since there are 1.684 times more soldiers than officers among military personnel, the incidence rate of COVID-19 was 1.567 times higher in officers than in soldiers. Even after the emergence of the omicron variant, the incidence rate of officers was 1.566 times higher than that of soldiers.
Fig. 2
Daily number of newly confirmed COVID-19 cases in Korean military and in the population of Korean civilians adjusted to the military populationa. The second graph shows the change in the proportion of each variantc among confirmed cases among the Korean military and civilian populations over time.
COVID-19 = coronavirus disease 2019, CI = confidence interval.
aThe trends in daily confirmed COVID-19 cases in Korean civilians adjusted to same population with the military are shown.
bThe change in trend in the daily number of confirmed COVID-19 cases in military was analyzed before and after December 5, 2021, when the first case with the omicron variant was detected in the Korean military. The trend was analyzed using segmented regression analysis of interrupted time-series.
cThe Armed Forces Medical Research Institute conducted variant tests on a mean of 16 samples (standard deviation: 13) of personnel with confirmed COVID-19 per week. The data on Korean civilians was obtained from the data published weekly by the Korea Disease Control and Prevention Agency (uniform resource locator: https://www.kdca.go.kr/contents.es?mid=a20107040000).
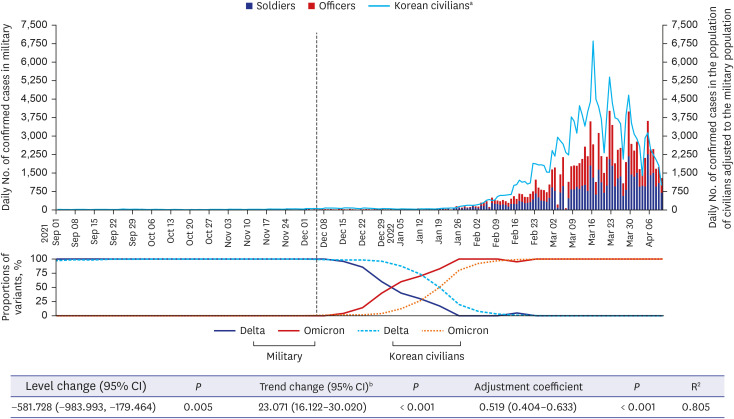
The trends in daily number of newly confirmed COVID-19 cases in the population of Korean civilians adjusted to same population with the military are also described. The vaccination completion rate among Korean civilians was 41.36% by the end of the primary vaccination phase of the military, 75.97% by November 1, 2021, and 80.84% by December 5, 2021.4 The booster vaccination coverage among Korean civilians was 44.96% after completion of the third vaccination phase of the military, and 64.18% at April 10, 2022, at the end of the study period. When the study period was divided into 3 periods based on the November 1 and December 5, 2021 reference dates, the number of daily confirmed cases among Korean civilians adjusted to same population with the military was a mean of 5.553 (standard deviation [SD] ± 4.918), 4.190 (SD ± 3.459), and 2.273 (SD ± 2.988) times higher than that of military personnel. The proportion of the delta and omicron variants among confirmed COVID-19 cases over time is shown in Fig. 2. Among military personnel, the proportion of cases due to the omicron variant exceeded 50% on January 2, 2022, and the omicron variant emerged more rapidly among military personnel than among Korean civilians.
Daily number of confirmed COVID-19 cases in the Korean military during the wave of the delta variant
The number of newly confirmed COVID-19 cases per day in the period when almost 100% of the confirmed cases were due to the delta variant is shown in Supplementary Fig. 1. With the reference date of November 1, 2021, approximately 3 months after the primary vaccination in the military, the number of confirmed COVID-19 cases increased significantly (regression coefficient, 0.832; 95% CI, 0.418–1.245; P < 0.001).
Trend in vaccination coverage of Korean military personnel with confirmed COVID-19 by week
The vaccination coverage of Korean military personnel with confirmed COVID-19 is shown by week in Supplementary Fig. 2. Except for a cluster of cases of COVID-19 at the beginning of October 2021 among personnel on a naval warship who had departed without vaccination, the proportion of confirmed cases of COVID-19 in unvaccinated personnel, who accounted for less than 10% of all military personnel, was similar to that among vaccinated personnel. Due to the mass vaccination with a second dose of vaccine in July 2021, the proportion of individuals classified as “not adequately vaccinated” increased from October 2021, and when the third vaccination was carried out from December 6, 2021, to January 14, 2022, the proportion of fully vaccinated confirmed personnel increased.
DISCUSSION
The results of the present study showed that the number of confirmed COVID-19 cases in the Korean military increased during 2 periods: there was a small increase after waning of the disease-protective immunity provided by the second dose of vaccine, and an exponential increase after the omicron variant became dominant. During the study period, although there was no significant change in the NPI strategies in the military and although a high vaccination coverage was maintained, after the emergence of the omicron variant, the increasing trend of the number of confirmed cases in the military followed that of the Korean civilian population.
During the wave of the delta variant, the number of confirmed COVID-19 cases in the military significantly increased 3 months after the primary vaccination. As in a previous study,10 it appears that the effectiveness of COVID-19 vaccination on the delta variant decreased with time. Considering that booster vaccination also increased the effect on the omicron variant,11 these trends support the vaccination guidelines of KDCA, which recommends booster mRNA vaccination 3 months after the second dose of vaccine to reduce transmission.
Before the emergence of the omicron variant, it was thought that, when over 70% of the population had completed the primary COVID-19 vaccination, the number of newly confirmed patients would be reduced due to herd immunity.12 In fact, after rapidly achieving a vaccination coverage of over 85% in the Korean military, the number of daily confirmed cases remained stable at less than 50 until November 2021, except for clusters of infection in units with a large proportion of unvaccinated personnel. However, after the emergence of the omicron variant, COVID-19 continued to spread, even after the third mass vaccination. These results are consistent with previous studies that have shown that the protective effect of the existing vaccine against symptomatic disease caused by the omicron variant was 62.4–73.9%, even shortly after the booster vaccination,13 and that it was not possible to achieve herd immunity with a vaccine that provided less than 70% protection against disease.14
The incidence rate of COVID-19 in the military was less than that among Korean civilians, which may have been due to not only the high vaccination coverage, but also to the NPI, including proactive PCR testing and isolation. However, considering that military personnel are relatively young and healthy, with few comorbidities, and given that the protective effect of the vaccine for severe COVID-19 is maintained even for the omicron variant,15 the probability of military personnel with COVID-19 progressing to severe disease is very low. If new SARS-CoV-2 variants with high transmissibility and low virulence emerge, according to the trend to date,16 an intensive NPI strategy within the military would increase the socioeconomic cost for excessive PCR testing and work disruption, which would outweigh the gains. Therefore, the target for disease control strategy should be revised from elimination of COVID-1917 to a “new normal” of life with COVID-19.18 For example, promoting the relatively inexpensive rapid antigen tests, and shortening the isolation period, would be effective for reducing the social cost and psychological stress that accompanies excessive regulation.
According to several previous studies,192021 soldiers living in groups often have close contact with each other without masks in their daily life, and are at risk of developing clusters of infection. However, in this study, the COVID-19 incidence rate during the study period was higher among officers than among soldiers. As most transmission among soldiers occurred in the form of clusters of infection, it can be inferred that relatively higher occurrence of COVID-19 among officers was because they had more contact with civilians and infected family members. During the COVID-19 pandemic, soldiers were health checked twice a day, and early detection and isolation strategy was conducted for symptomatic soldiers. Also, the space between beds in barrack is more than 1 m, and the wearing of masks is emphasized during official activities. To keep the COVID-19 incidence of soldiers low, even if other NPIs are alleviated, interventions to reduce the density of living spaces of soldiers would still be needed.
Our study had some limitations. First, because the data of the study were reviewed retrospectively, it was difficult to track vaccination status of approximately 30% of personnel with COVID-19. Second, except during the period directly after the primary vaccination and booster vaccination, data were not collected on vaccination coverage among military personnel. As some personnel received a third vaccination in civilian institutions, the coverage of third vaccination was underestimated. Third, as the disease severity among confirmed cases was unknown, effectiveness of COVID-19 vaccines for preventing severe disease caused by the delta and omicron variants could not be analyzed. Last, variant tests were conducted on only an average of 16 specimens per week in the military. Due to small number of specimens, there may be differences from the actual proportion of variants among confirmed military personnel, but to have representativeness, random samples from different units were selected every day.
In conclusion, the spread of the omicron variant occurred in the Korean military, despite more than 60% of Korean military personnel having received a third COVID-19 vaccination and the military maintaining intensive NPI.
 XML Download
XML Download