

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Progressive supranuclear palsy (PSP) closely overlaps with corticobasal degeneration (CBD) in terms of atypical parkinsonism and tauopathy.1 The clinical features of CBD include asymmetric parkinsonism (rigidity, akinesia, myoclonus, and dystonia) and cortical symptoms (apraxia, alien hand, frontal lobe dementia, and aphasia).2 PSP clinically presents as an early onset of unexplained frequent falls, subsequent parkinsonism, vertical gaze palsy, dementia, pseudobulbar palsy, and cervical dystonia.3
Tau protein is a microtubule-associated phosphoprotein.14 Six isoforms of tau proteins are generated by alternative mRNA splicing of exons 2, 3, and 10 in the adult human brain.14 Tauopathies are classified into three repeat (exon 10 missing, 3R), four repeat (exon 10 present, 4R), or equal ratios of 3R and 4R tau due to the predominance of tau isoforms in cytoplasmic inclusions.45 PSP and CBD present as an accumulation of abnormal 4R tau isoforms in glial cells and neurons.1467
Regarding the misdiagnosis rate by the clinical–pathological overlapping between CBD and PSP, 42% of the pathologically diagnosed CBD cases clinically presented as a progressive supranuclear palsy and 29% of cases with corticobasal syndrome (CBS) had underlying PSP pathology.8 Other studies have also shown that about a third of autopsy-proven CBD cases were clinically diagnosed as PSP.28 Conversely, in autopsy-confirmed PSP cases, CBS presentation was rare.89
Herein, we report the neuropathological features of a patient with autopsy-confirmed CBD with PSP–CBD overlapping symptoms.
CASE DESCRIPTION
Clinical history
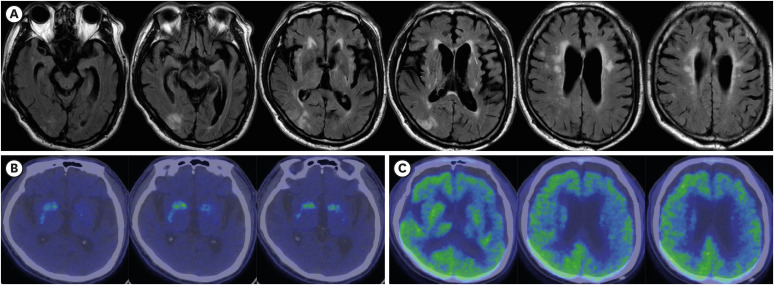
A 71-year-old man visited our movement disorder clinic because of aggravated and frequent freezing of gait and recurrent falls from age 68. Neurological examination at age 71 revealed marked limitation of the vertical saccade, bilateral slow horizontal saccade, dysarthria, symmetric bradykinesia, prominent axial rigidity, short steps and shuffling gait, postural instability, and progressive cognitive impairment. Cortical dysfunctions such as nonfluent language problems and limb apraxia were found. The mini mental state examination score was 25, and the clinical dementia rating scale score was 0.5. Magnetic resonance imaging (MRI) of the brain, which was taken when he had a cerebral ischemic stroke (at age 70), revealed prominent midbrain and left frontotemporal atrophies and right parietal–temporal infarction (Fig. 1A). Fluoro-propyl-carbomethoxy-iodophenyl-tropane (FP-CIT)-positron emission tomography (PET) revealed an asymmetrically decreased bilateral uptake in both the putamen and caudate nucleus (CN) (Fig. 1B). Fluorodeoxyglucose-PET noted a diffusely and asymmetrically decreased uptake in the left frontotemporoparietal lobes and thalamus (Fig. 1C). The response to levodopa treatment was poor. He died at age 72 because of acute pneumonia.
Fig. 1
Brain MRI and PET images of the patient. (A) T2 FLAIR-weighted axial brain MRI revealed acute right parietotemporal infarction, significant atrophy in the midbrain, and diffuse frontotemporal lobes, more severe on the left. (B) FP-CIT PET revealed decreased uptake in the tail portion of the bilateral putamens and caudate nuclei. (C) FDG-PET detected diffuse and asymmetrically decreased uptake in the left frontotemporal cortex, parietal lobe, and thalamus.
FDG = fluorodeoxyglucose, FP-CIT = fluoro-propyl-carbomethoxy-iodophenyl-tropane, MRI = magnetic resonance imaging, PET = positron emission tomography.
Pathology
All autopsy procedures were performed according to the protocol recommended by the Korean Brain Bank Network under the Korea Brain Research Institute and the proposal guidelines for standardized operating procedures.10
The whole brain weighed 1,350 g. Gross findings of the left brain fixed in formalin for 4 weeks revealed mild atrophy in the frontal cortex and midbrain in the sagittal plane, like a hummingbird sign (Fig. 2A, left). Coronal sections also exhibit mild atrophy in the frontal cortex, CN, thalamus, subthalamic nucleus (STN), and midbrain (Fig. 2A). The substantia nigra (SN) showed moderate pallor, and the locus ceruleus (LC) showed mild pallor (Fig. 2B). Lacunar infarction in the putamen (Fig. 2A) and a microhemorrhage in the pons (Fig. 2B) were also observed.
Fig. 2
Macroscopic (A and B) and microscopic (C-H) findings of the brain. (A) Sagittal section presenting the frontal lobe and midbrain atrophy (left). The midbrain is significantly atrophied than the pons. Coronal sections of the brain exhibiting mild cortical atrophy in the frontal cortex and thalamic region and moderately dilated ventricles with lacunar infarct in the putamen (circle) (right). (B) The midbrain exhibited moderate-to-severe hypopigmentation in the substantia nigra (arrowhead) and mild pallor in the locus ceruleus (arrow) with microhemorrhage in the pons (circle). (C) Mild superficial microvacuolation was observed in the frontal cortex (H&E, 40×). (D) Gallyas silver staining revealed dense astrocytic plaques (arrow heads) in the frontal lobe (200×). (E) Tau-positive threads and coiled bodies (arrows) were frequently observed in the subcortical white matter of the frontal lobe (AT8, 400×). (F) Several tau-positive neurons and threads were identified in the amygdala (AT8, 200×). (G) A ballooned neuron is observed in the amygdala (H&E, 400×). (H) A ballooned neuron is highlighted by tau staining in the amygdala (AT8, 400×).
H&E = hematoxylin and eosin staining.
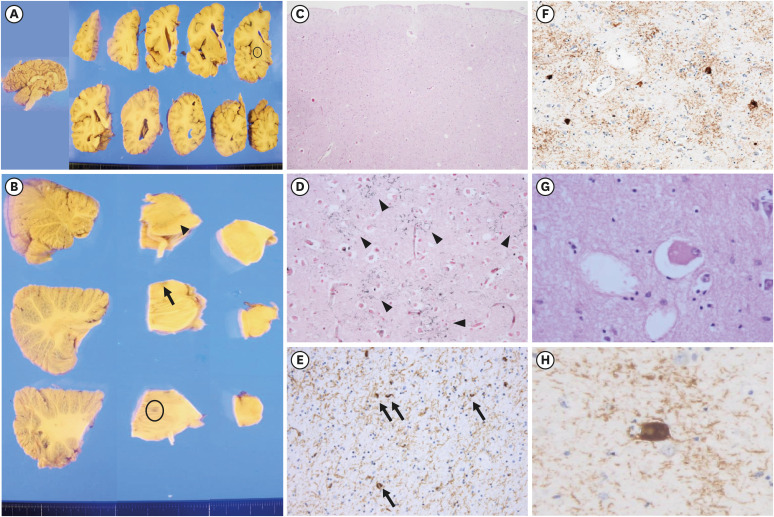
In microscopic examinations, hyaline arteriolosclerosis in the basal ganglia (BG) and multiple microinfarctions in the putamen were found. The subcortical white matter (WM) myelin pallor was moderate in the frontal cortex, motor cortex, internal capsule, and cerebral peduncle and mild in the temporal cortex. The hematoxylin and eosin staining of the neocortex revealed mild superficial spongiosis, neuronal loss, and gliosis (Fig. 2C). Neuronal loss and gliosis were severe in the SN, moderate in the CN, globus pallidus (GP), thalamus, STN, and mammillary bodies, and mild in the entorhinal cortex, nucleus basalis of Meynert (nbM), and LC.
Abnormally phosphorylated tau deposits were highlighted by Gallyas silver staining and AT8 (phosphorylated tau) immunohistochemistry (IHC). The distribution and frequency of tau deposits are summarized in Table 1,11 as adapted from the criteria for CBD.7 Astrocytic plaques and threads were predominantly observed in the frontal lobe (Fig. 2D) and amygdala. Tau-positive threads and oligodendroglial coiled bodies were distributed in the frontal subcortical WM (Fig. 2E). Moreover, tau-positive neurons were extensively distributed and frequently observed in the entorhinal cortex, hippocampus, and amygdala (Fig. 2F). Some ballooned neurons were found in the amygdala (Fig. 2G and H), and a few were observed in the anterior cingulate and nbM.
Table 1
Distribution and severity of the histopathologic lesion
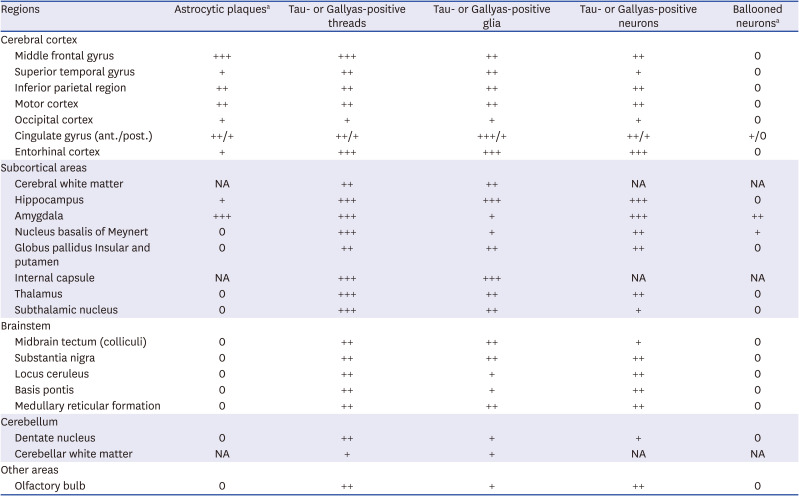
0 = none, + = sparse, ++ = moderate, +++ = very frequent (by standard reference illustrations of CERAD guidelines11), NA = not applicable, ant. = anterior, post. = posterior.
aCriteria of astrocytic plaques and ballooned neurons: + = mild/sparse.
Beta-amyloid, α-synuclein, and TDP-43 immunohistochemistry (IHC) were also performed to exclude other neurodegenerative diseases. Beta-amyloid IHC did not reveal any amyloid deposition in areas including the frontal cortex and medial temporal region. Amyloid angiopathy was not detected. Alpha-synuclein IHC highlighted the absence of Lewy bodies in the amygdala, cingulate, or midbrain. TDP-43 IHC did not reveal neuronal cytoplasmic or intranuclear inclusions or dystrophic neurites.
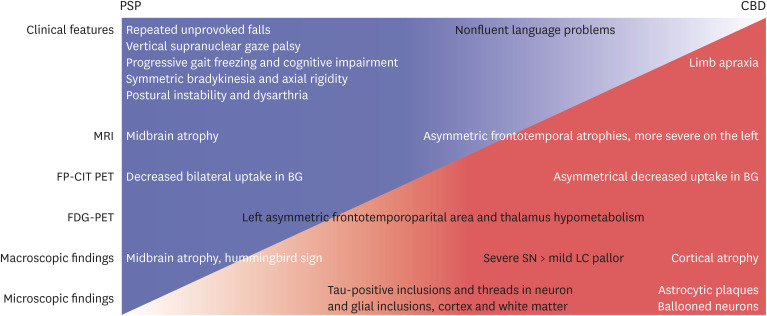
We made a schematic illustration about preferences of PSP or CBD in clinical and pathological findings of the patient (Fig. 3).
Fig. 3
Schematic illustration of PSP or CBD preferences in the clinical and pathological findings of the patient. The initial clinical symptoms, midbrain atrophy in the MRI, and bilateral decrease in the FP-CIT uptake in the BG suggested a clinical diagnosis of PSP. The midbrain on the sagittal section was astonishingly similar to the hummingbird sign, which was widely known as one of the characteristic radiological findings of PSP. However, later development of limb apraxia, asymmetric cortical atrophy in the MRI, and a more severe decreased FP-CIT uptake on the left putamen indicated CBD. In the macroscopic findings, less severe hypopigmentation of the LC than of the SN and more extensive cortical atrophy including the posterior cortex also implied CBD. Finally, astrocytic plaques and ballooned neurons were almost exclusively observed in CBD. Black-colored phrases were overlapping findings of both PSP and CBD.
PSP = progressive supranuclear palsy, CBD = corticobasal degeneration, MRI = magnetic resonance imaging, FP-CIT = fluoro-propyl-carbomethoxy-iodophenyl-tropane, BG = basal ganglia, LC = locus ceruleus, SN = substantia nigra, PET = positron emission tomography, FDG = fluorodeoxyglucose.
DISCUSSION
The Movement Disorder Society Clinical Diagnostic Criteria for PSP (MDS-PSP) suggested the combinations of core clinical features, supportive clinical clues, and imaging findings plus the mandatory inclusion criteria of basic features.3 The mandatory basic features were sporadic occurrence, age ≥ 40 years at onset, and gradual progression of PSP-related symptoms.3 The four core features were ocular motor dysfunction, postural instability, akinesia, and cognitive dysfunction.3 According to the level of certainty (highest, mild, and lowest) of the MDS-PSP criteria,3 the initial symptoms of our patient corresponded to probable PSP because of the core features (vertical supranuclear gaze palsy, repeated unprovoked falls within 3 years, progressive gait freezing within 3 years, akinetic rigidity, and ideomotor apraxia), supportive clinical cue (poor levodopa response), and supportive imaging finding (midbrain atrophy and bilateral striatal dopaminergic denervation despite asymmetricity).3 Given the combination of clinical features, the clinical predominance type of our patient was probably PSP with Richardson’s syndrome, with progressive gait freezing or predominant parkinsonism.3
In our patient, axial rigidity, postural instability/falls, and vertical gaze palsy can be classified as progressive supranuclear palsy syndrome (PSPS) among the five phenotypes of CBD.2 PSPS accounted for about one-fourth of pathologically confirmed CBD cases.2 Axial rigidity, gait abnormalities, postural instability, and falls were observed only in about one-third of CBD cases at presentation.2 Therefore, our patient was more likely to be diagnosed with PSP, not CBD, in the early stages. Cortical dysfunction around 3 years after diagnosis suggested clinical CBD.2
Regarding the macroscopic findings of CBD, the SN was usually hypopigmented, whereas LC pigment may be grossly preserved.7 Our patient also had less hypopigmentation on the LC; however, these findings were reported in typical PSP.6 Second, neuronal loss and gliosis of the SN are observed in both PSP and CBD. However, cortical involvement is prominent in CBD, whereas the involvement of BG is prominent in PSP.67 Third, tau-positive threads in CBD were diffusely distributed in the subcortical WM and gray matter (GM), GP, BG, STN, thalamus, brainstem, and cerebellum.67 The distribution of tau-immunopositive threads in PSP tends to overlap with that of CBD.6 The density of tau-positive threads in CBD were equally presented in both GM and WM, or more observed in the WM.6 Tau-positive threads in both the cortical and subcortical areas in our patient appear to be more relevant to CBD. Fourth, ballooned neurons of the cortical areas in CBD have a diagnostic significance, but they are very rare as the PSP pathology.6 Our patient had ballooned neurons in the anterior cingulate gyrus and amygdala, and the findings do not carry strong diagnostic significance.67 Ballooned neurons in the anterior cingulate gyrus and amygdala did not have a diagnostic significance in our patient. Fifth, PSP usually demonstrated symmetrical cortical atrophy, but CBD usually presented with cortical involvement and laterality.6 Finally, astrocytic plaques affecting the cortices and striatum are significantly pathognomonic findings of CBD.6 In our patient, astrocytic plaques were observed in the cerebral cortices, consistent with the pathologic diagnosis of CBD.
In summary, clinical findings such as supranuclear palsy, symmetric akinesia, rigidity, dysarthria and dysphagia, and midbrain atrophy in MRI and gross examination (hummingbird sign), decreased FP-CIT uptake in both BG more closely resembled PSP (Fig. 3). On the contrary, cortical dysfunction, asymmetric cortical atrophy in MRI, asymmetric decrease in FP-CIT uptake in the BG, and less severe LC pallor (not always) favor CBD. Microscopically, astrocytic plaques, tau-positive neurons, glia, and threads in the cortex and subcortical areas confirmed the final diagnosis as CBD. Moreover, right cortical infarction, multiple lacunes, and arteriosclerosis in the BG may contribute to the symptoms of our patient. They had probably made the initial diagnosis of CBD difficult.
Typical cases of CBD and PSP can be easy to clinically differentiate, but the definitive diagnosis of PSP and CBD have been only made pathologically. Thus, understanding the complex clinical course of CBD and PSP through a sufficient follow-up period will aid in making a more reliable diagnosis.
 XML Download
XML Download