

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
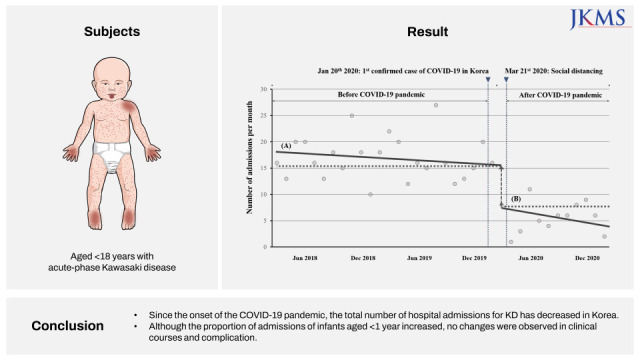
Kawasaki disease (KD), an idiopathic systemic febrile vasculitis, predominantly affects children aged < 5 years. It is the most common cause of pediatric acquired heart disease in developed countries.1 A high KD incidence has been reported in Northeast Asian countries, and Korea has the second highest incidence after Japan.2 According to 2015–2017 nationwide surveys on KD in Korea, the KD incidence has been steadily increasing since 2000.3 The etiology of KD remains unknown, but the leading theory is that preceding infection triggers immune system activation in a susceptible child. The seasonality of KD incidence supports this hypothesis.4
The coronavirus disease 2019 (COVID-19) was declared a pandemic on March 11, 2020.5 In Korea, the first case was announced on January 20, 2020, and as of August 15, 2021, there were 223,920 confirmed cases and 2,156 COVID-19-related deaths.6 After the first case, people voluntarily wore masks and refrained from going out.7 As the number of confirmed cases increased, the Korean government gradually raised the infectious disease risk alert level and officially implemented enhanced social distancing on March 20, 2020. Accordingly, interventions such as the mandatory wearing of masks in public places, restrictions on private gatherings and on the use of public and multipurpose facilities, and school closures were implemented.8
Social distancing has led to an overall reduction in pediatric cases and a dramatic decrease in the incidence of pediatric respiratory tract infections worldwide. In Finland, after a national lockdown in early 2020, pediatric emergency room visits for respiratory infections decreased by a third; further, the nationwide number of pediatric influenza and respiratory syncytial viral infection cases decreased.9 Similarly, not only in Korea but also in Canada and Taiwan, hospital visits for pediatric respiratory symptoms decreased by > 50%.101112
Against this background, it is meaningful to investigate changes in the incidence of KD in Northeast Asia since the COVID-19 outbreak. We aimed to confirm the change in the number of patients with KD during the COVID-19 pandemic by examining the seasonality of KD through a sufficiently long observation period and identifying changes in clinical characteristics and prognosis of KD using electronic medical record data.
METHODS
Study design and population
All data were extracted from the Clinical Data Warehouse (CDW), which provides access to a large database of patients from five hospitals in Korea: Seoul St. Mary’s Hospital, Yeouido St. Mary’s Hospital, Bucheon St. Mary’s Hospital, Uijeongbu St. Mary’s Hospital, and St. Vincent Hospital.
We extracted the data of patients with KD who were aged < 18 years from the CDW using the International Classification of Diseases, 10th Revision (ICD-10), code for KD (M30.3) between March 2018 and February 2021.13 We included patients who were in the acute phase of KD and excluded those with a secondary diagnosis and those who did not receive acute-phase treatment. Data analysis was performed after excluding readmission and duplicate data.
The acute phase of KD was defined as a primary diagnosis of KD treated with intravenous immunoglobulin (IVIG) therapy or a moderate (30–50 mg/kg/day) to high (80–100 mg/kg/day) dose of aspirin as anti-inflammatory therapy. A primary diagnosis of KD was defined as the first diagnosis of KD with the ICD-10 code M30.3. Each hospitalization for acute-phase KD was considered as an independent case. However, readmission within 60 days of the initial episode was considered as a continuation of the acute phase and was excluded.14 In addition, we identified duplicate data by reviewing the medical records of patients of the same sex and with the same birthdate.
Outcome definitions and measurements
We assessed the number of hospitalizations per month for 3 consecutive years during the study period. We divided hospitalizations into two groups based on whether they occurred before or after March 2020, that is, before and after the onset of the COVID-19 pandemic, to determine its effect on KD.
We also compared changes in the proportion of patients with refractory KD before and after the onset of the COVID-19 pandemic as well as differences in the disease’s clinical characteristics. Refractory KD was defined as resistance to the first IVIG infusion requiring the following additional treatments after at least 2 calendar days: additional IVIG, corticosteroids, and infliximab.1
The following cardiac complications were investigated using echocardiographic data captured within 2 months of the diagnosis of KD: coronary artery abnormalities, valvular regurgitation, pericardial effusion, and ventricular form and function. If echocardiography was performed multiple times within the 2 months, for each observed complication, the dataset depicting the highest severity of findings was selected for analysis. Coronary artery abnormalities were defined as Z-scores for one or more branches meeting the criteria, based on the Z-score classification system recommended in the American Heart Association guidelines updated in 2017.1 Valvular regurgitation was defined as mild to more severe degrees of regurgitation in the tricuspid and aortic valves. Ventricular form and function were evaluated using left ventricle end-diastolic and end-systolic diameters and ejection fraction as indicators.1
Statistical analysis
We performed a segmented regression analysis, a statistical method for estimating the impact of events in time series data, to identify changes in the monthly number of acute-phase KD.15 This method examines the changes in the level and trend of the measure following an event. The event in this study was the COVID-19 pandemic in Korea, the independent variable was the week of the year, and the dependent variable was the number of admissions for KD. As seasonal variations existed in the trend of the changes in the number of KD, the data were adjusted for seasonality.
To compare the characteristics of the two groups divided into the pre- and post-pandemic periods, we used Pearson’s χ2 test with Yates’ continuity correction or Fisher’s exact test for qualitative variables. In particular, only Pearson’s χ2 test was used for the comparison of the age distribution of the three groups. Moreover, Student’s t-test or the Mann–Whitney U test was used for quantitative variables.
All analyses were performed using R version 4.0.0 (R Foundation for Statistical Computing, Vienna, Austria), with the probability level for significance set at a P value of <0.05.
RESULTS
Demographic data and clinical characteristics of patients with KD after COVID-19
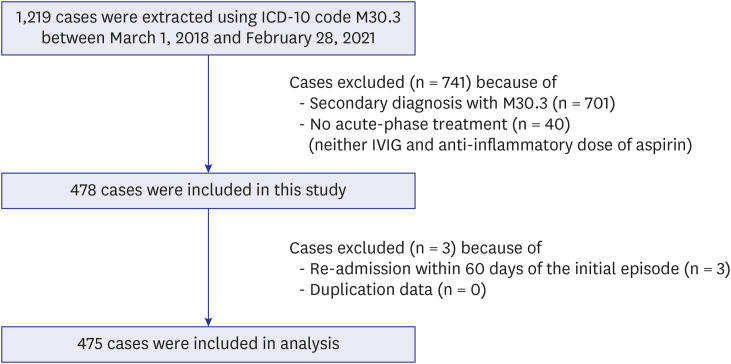
Data from 1,219 hospital admissions with the ICD-10 code M30.3 were extracted between March 1, 2018 and February 28, 2021. Among these, 478 patients with acute-phase KD were identified, and 701 patients with a secondary diagnosis of KD and 40 patients who did not receive treatment with either IVIG or aspirin (anti-inflammatory dose) were excluded. In addition, three patients who were readmitted within 60 days of the initial episode were excluded. Finally, 475 patients were included in the analysis (Fig. 1). There were no duplicate admissions resulting from transfers between the five hospitals among patients with the same birthdate and of the same sex.
Fig. 1
Flowchart of the study population.
ICD-10 = International Classification of Diseases, 10th Revision, IVIG = intravenous immunoglobulin.
The demographic data and clinical characteristics are summarized in Table 1.1617 Children diagnosed with acute-phase KD after the COVID-19 outbreak were younger than those diagnosed with KD before the outbreak, and there was no difference based on sex. Further, there were no differences in the Sano score, a predictive system for IVIG resistance, between the two groups.16 Laboratory tests revealed no significant differences in variables apart from the C-reactive protein (CRP) level and neutrophil fractions. The CRP level and neutrophil fractions were lower after the pandemic onset than during the pre-pandemic period. Most of the children in both groups received IVIG as the first treatment, but five patients received only an anti-inflammatory dose of aspirin. After the COVID-19 outbreak, the average duration of hospitalization was shorter. No patients in our sample tested positive for COVID-19 since the onset of the pandemic.
Table 1
Characteristics of patients with KD before and after the COVID-19 pandemic
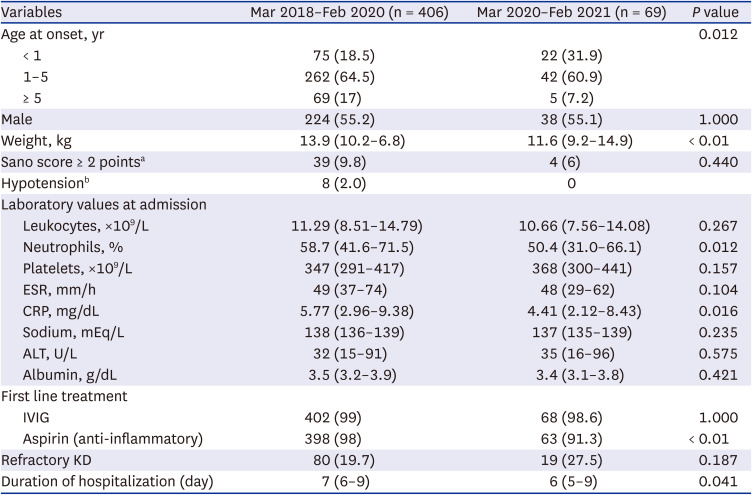
Variables are expressed as number (%) or median (interquartile range).
KD = Kawasaki disease, COVID-19 = coronavirus disease 2019, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, ALT = alanine transaminase, IVIG = intravenous immunoglobulin.
aSano score: scores calculated through the Sano predictive system as follows: 1) AST level ≥ 200 IU/L, 1 point; 2) CRP level ≥ 7 mg/dL, 1 point; and 3) total bilirubin level ≥ 0.9 mg/dL, 1 point.16
bHypotension is defined as a systolic blood pressure that is less than the fifth percentile of the normal blood pressure for the patient’s age.17
Decrease in the number of patients with KD after COVID-19
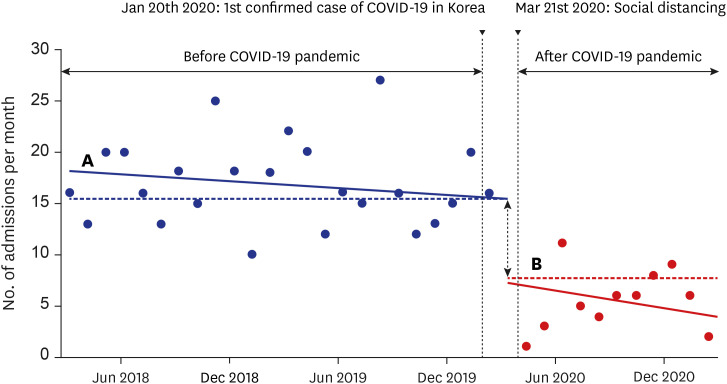
We identified 406 cases between March 2018 and February 2020 and 69 cases between March 2020 and February 2021. Since March 2020, the number of KD cases has decreased by 33.9% compared with the average number in the previous 2 years. Segmented regression analysis was used to determine the effect of COVID-19 on the number of KD cases per month; a significant decrease was found in the number of KD cases in March 2020, between the time when COVID-19 was first reported in Korea and the time when the government implemented an enhanced social distancing policy. In March 2020, there was a significant decrease of 7.9 persons/month (95% confidence interval [CI], −13.8 to −2.0; P = 0.009). Prior to this timepoint, the number of admissions was decreasing at a rate of 0.1 persons/month (95% CI, −0.3 to 0.1; P = 0.366); after this timepoint, the number of KD cases started decreasing at a rate of 0.2 persons/month (95% CI, −0.9 to 0.5; P = 0.572). However, these differences were not statistically significant (Fig. 2).
Fig. 2
Segmented regression analysis of the number of patients with KD. Compared with that in Mar 2018–Feb 2020 (A), the number of patients with KD per month in Mar 2020–Feb 2021 (B) has significantly decreased by 7.9 persons/month (95% CI, −13.8 to −2.0; P < 0.05). During the periods of 2018–2020 (A) and 2020–2021 (B), there was a decreasing trend in the number of admissions, but this trend was not statistically significant.
KD = Kawasaki disease, CI = confidence interval, COVID-19 = coronavirus disease 2019.
Proportion of patients with refractory KD after COVID-19
The demographic data and clinical characteristics of patients with refractory KD are summarized in Table 2. We identified 80 cases of refractory KD between March 2018 and February 2020 and 19 cases between March 2020 and February 2021. The proportion of patients with refractory KD did not change significantly since the COVID-19 outbreak (19.7% vs. 27.5%, P = 0.187). In both groups, the predominantly administered second treatment was a second dose of IVIG (63.8% vs. 68.4%, P = 0.908), followed by intravenous steroid treatment (55% vs. 57.9%, P = 1.000). No patient in either group received a third dose of IVIG.
Table 2
Characteristics of patients with refractory KD before and after the COVID-19 pandemic
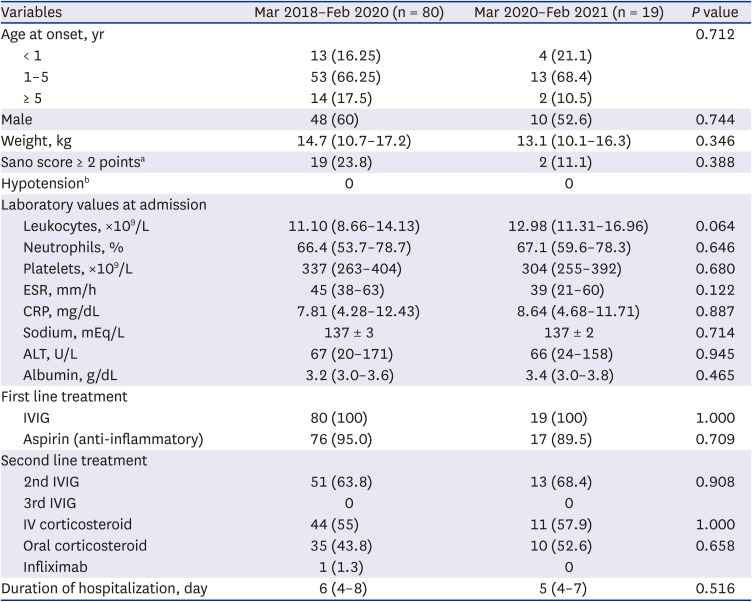
Variables are expressed as number (%), mean ± standard deviation, or median (interquartile range).
KD = Kawasaki disease, COVID-19 = coronavirus disease 2019, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, ALT = alanine transaminase, IVIG = intravenous immunoglobulin, IV = intravenous.
aScores calculated through the Sano predictive system as follows: 1) AST level ≥ 200 IU/L, 1 point; 2) CRP level ≥ 7 mg/dL, 1 point; and 3) total bilirubin level ≥ 0.9 mg/dL, 1 point.16
bHypotension is defined as a systolic blood pressure that is less than the fifth percentile of the normal blood pressure for the patient’s age.17
KD-related cardiac complications after COVID-19
Among the patients with KD diagnosed after the COVID-19 outbreak, 57 underwent echocardiography within 2 months of admission. Of these patients, seven (12.8%) exhibited coronary complications, and five (8.8%) exhibited pericardial effusion. Valvular regurgitation and ventricular dysfunction or dilatation were not observed. There were no statistically significant differences before and after the COVID-19 outbreak (Table 3).
Table 3
Cardiac complications of KD before and after the COVID-19 pandemic

DISCUSSION
Our data demonstrate that the monthly number of KD cases has significantly decreased since the outbreak of the COVID-19 pandemic. By contrast, the proportion of patients aged < 1 year with KD has increased compared with that before the outbreak. However, the proportion of patients with refractory KD did not change. Moreover, no significant changes were observed in the rates of coronary complications and pericardial effusion.
To the best of our knowledge, this is the first study to examine the changes in the clinical features and complications of KD in Korea after the COVID-19 outbreak. In addition, as this was a multicenter study conducted over a period of > 1 year after the onset of the COVID-19 pandemic, we were able to fully consider the seasonal variability in the occurrence of KD.
There have been a few reports regarding a decrease in the number of KD after the COVID-19 outbreak. A nationwide observational study in Korea reported that the number of patients with KD decreased by 40% from February to September 2020 compared to the same period in the year before COVID-19.18 On the other hand, no changes were observed in the proportion of patients with refractory KD compared to that reported in 2019.18 These results are consistent with our study. However, the observation period in the earlier nationwide study was insufficient for confirming the incidence of KD, which peaks in winter. Additionally, since it represents a big data study based on records derived from the National Health Insurance Service database, there may have been errors in the estimation of the incidence of KD as a result of duplicate or heterogeneous data.1920 Moreover, this earlier study did not exclude Kawasaki-like diseases, such as adenovirus infection and measles.18 Our study, on the other hand, included all seasons as we examined data over a 1-year period since the onset of the COVID-19 pandemic. In addition, we used a detailed operational definition of KD and an electronic medical record review to exclude Kawasaki-like diseases and duplicate cases to the greatest possible extent.
In Japan, three studies reported a decrease in the number of patients with KD after the COVID-19 outbreak. Of these, two multicenter studies reported reductions of 47.1% and 53%, respectively, and one nationwide study reported a reduction of 35%.212223 These studies compared data from 2020 to records from the last 3–5 years. However, they were all focused on the correlation between KD and infectious diseases, and lack a discussion of changes in the clinical features of KD. One multicenter study reported that the prominent clinical features of patients with KD in 2020 were a significantly lower white blood cell count, neutrophil count, and refractory KD ratio and that there was no significant difference in cardiac complications.21 However, this study was based on the data of only 36 patients collected from April to May, which represents a short study period as well as a small number of participants. Here, we investigated changes in the clinical features of both KD and refractory KD before and after the onset of the COVID-19 pandemic, and we reviewed the results of serial echocardiography examinations conducted over 2-month periods in these patients during the entire study period to determine whether cardiac complications occurred.
The exact cause of the decrease in the number of KD remains unclear. However, considering the dominant hypothesis that a preceding infection acts as a trigger for inflammation leading to KD, the main reason could be the decrease in pediatric infective diseases due to social distancing.4 Similar hypotheses have been proposed in previous studies.2223 After the first case of COVID-19 in Korea, a high number of people started wearing masks and refrained from going out even before the government officially declared that social distancing was necessary,7 which led to a nationwide decrease in respiratory infections.24 In addition, at our institution, there was an immediate decrease in emergency room visits for pediatric infectious diseases after the first case of COVID-19.25 With regard to KD, a significant decrease was observed from March, later than the one observed for infective diseases. These findings support the notion that social distancing is associated with the decrease in pediatric infectious diseases and corroborate the antecedent infection theory of KD.
Another explanation for the decrease in the number of admitted patients with KD may be the reluctance of caregivers to visit a hospital for fear of exposure to COVID-19. A multinational study found that 20% of caregivers said that they were reluctant to visit the emergency room for fear of being infected with COVID-19 at the hospital.26 In Italy, there have been several reports of aggravation of disease caused by delays in visits to pediatric emergency facilities due to caregivers’ reluctance.2728 However, some previous studies have suggested that the reluctance of caregivers and patients to visit a hospital for fear of exposure to the virus was not associated with the reduced incidence of KD.2329 One of these studies inferred that caregivers would not delay visits to the hospital due to the serious clinical presentation of KD; another study suggested that there was no difference in the duration of fever (in days) at the time of admission. In our sample, the length of hospital stay of patients with KD was significantly shortened after COVID-19, but this was not true for refractory KD. This may be due to fewer patients visiting the hospital very early in the clinical course of KD or due to patients being discharged earlier, which is not the case in refractory KD. Therefore, our findings may indeed be evidence of the fear of caregivers of contracting COVID-19 at a hospital. However, we are somewhat limited in the interpretation of our data, because we did not collect data on clinical day of KD on admission or on incomplete KD.
The proportion of children aged < 1 year with KD was larger after than before COVID-19 in our sample. Age < 1 year is one of the known risk factors for refractory KD.3031 A previous study has suggested that children aged < 1 year have a higher risk of contracting respiratory infections through parents or others because wearing a mask is not recommended in this age group. For this reason, the decrease in the number of patients with KD during the COVID-19 pandemic may be less pronounced in these children than in other age groups.23 However, our study was not designed to investigate this question, since it is only one of several factors we assessed, and further research is therefore needed.
Our results demonstrate no difference in the proportion of patients with refractory KD, pericardial effusion, and coronary artery complications between the two assessed time periods. It is well known that refractory KD is associated with prolonged fever and more severe coronary outcomes.30 In addition, pericardial effusion is observed in 6–24% of patients with acute-phase KD, which is suggestive of severe cardiac inflammation and is has been reported to be strongly associated with coronary artery complications.31 Therefore, our results indicate that there was no change in the severity of KD before and after COVID-19.
After the onset of the COVID-19 pandemic, there has been an increase in the incidence of multisystem inflammatory syndrome in children (MIS-C), a condition with clinical features similar to those of KD, in North America and Europe, which has been causing concern worldwide.3233 However, patients with MIS-C are generally older and have gastrointestinal symptoms, hemodynamic instability, and lower platelet counts, which are different from the features of classic KD.34 Additionally, very few MIS-C cases have been reported in Korea and Japan, where the prevalence of KD is high.35363738 In our study, all patients with KD who presented during the COVID-19 pandemic underwent screening for COVID-19 using polymerase chain reaction (PCR) tests prior to hospitalization. All PCR tests were negative, however, and there were thus no confirmed cases of COVID-19 in our sample. We assume that this is due to the overall smaller number of confirmed cases of COVID-19 in Korea compared to North America and Europe as well as to differences in susceptibility based on race.
This study has several limitations. First, this was a retrospective study on data that were extracted from the CDW, which provides access to a large database of patients from five hospitals. Second, since the ICD-10 coding system was used, there may be inaccuracies in the diagnostic data. These are, however, inherent limitations of studies using data from administrative databases. Moreover, we attempted to increase the accuracy of our results by using more detailed operational definitions and verification procedures to avoid including duplicate cases. Third, the diagnosis and treatment of KD did not follow the same protocol but was at the discretion of individual physicians at the five included hospitals, which resulted in differences in aspirin treatment and the non-implementation of echocardiography in all cases.
The strength of our study is that we identified changes in clinical features and complications in addition to changes in the number of patients with KD admitted to hospitals. For this purpose, we used data from a large database of five hospitals that provides a variety of clinical data from de-identified patients, such as medical records, drug prescription histories, laboratory test results, and imaging findings. In addition, since the five hospitals are all located in the Seoul Metropolitan Area where half of the Korean population resides, potential regional deviations could be reduced in our study. The trend of the number of patients with KD admitted to the hospital during the 2 years before the COVID-19 pandemic at these five hospitals was not significantly different from that shown by the National Health Insurance Service data during this same period. Therefore, we consider our findings reliable.
In conclusion, this study reveals a decrease in the number of patients with KD after the onset of the COVID-19 pandemic. We also found that the proportion of children aged < 1 year with KD was larger after the onset of the pandemic than during the pre-pandemic period. Although no change in disease severity was observed in our sample, our findings need to be interpreted with caution because age < 1 year is a risk factor for refractory KD. Further long-term studies are needed to identify whether the decreased incidence of KD persists.
 XML Download
XML Download