

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vitamin D was first discovered in the early 20th century and was considered to be a fat-soluble vitamin. Recent studies have demonstrated that vitamin D plays numerous roles as a prohormone in the human body [1], and is mainly involved in bone and calcium metabolism [23]. Vitamin D is produced in the skin through exposure to adequate sunlight, or is ingested in the form of vitamin D2 (ergocalciferol) and vitamin D3 through food. Vitamin D is not active by itself and must be converted into a physiologically active metabolite through 2 hydroxylation processes in the liver and kidney. The final metabolite of vitamin D as an active hormone is calcitriol (1,25(OH)2D), whereas the prohormone calcifediol (25(OH)D) is a precursor of vitamin D [4].
The primary function of vitamin D involves promoting the absorption of calcium and phosphorus in the intestinal tract or liver through vitamin D-dependent proteins. Vitamin D contributes to maintaining the blood levels of calcium and phosphorus necessary for the mineralization of bones [5]. In addition, the presence of vitamin D receptors on immune cells and various tissues such as the skin, brain, prostate, pancreas, breast, and colon has revealed its role to extend beyond extra-skeletal functions. Indeed, vitamin D is reported to affect cell proliferation and differentiation in the body, regulation of immune functions, and anti-cancer activity [678]. Furthermore, recent studies indicate that vitamin D influences muscle development, and chronic diseases (such as cardiovascular diseases, diabetes, metabolic syndrome, emphysema in smokers, and autoimmune diseases) are highly correlated with vitamin D concentration in the body [91011121314151617].
Growing evidence suggests that the risk of osteomalacia during the aging process is much greater than previously reported [1819]. Approximately 30–40% of hip fractures are caused by osteomalacia rather than osteoporosis. The remaining 60–70% cases are a result of insufficient mineralization due to lack of calcium and vitamin D and the combined effects of osteoporosis and early stages of osteomalacia [18]. Consequently, vitamin D supplementation is shown to effectively prevent hip fractures in the elderly [19]. In addition, vitamin D deficiency is also associated with the onset and progression of type 2 diabetes and sarcopenia [1213], and low levels of vitamin D are reportedly correlated with osteoporosis, depression, and various chronic diseases, including cancer, autoimmune diseases, and cardiovascular diseases [20212223].
Since the daily intake of vitamin D varies greatly depending on race, age, region of residence, disease state, and culture, the daily intake and lifestyle behaviors act as important variables [11]. South Korea is geographically located at 33–43°N latitude, with an abundant amount of sunlight. Thus, there is no prevalence of vitamin D deficiency, and hence vitamin D supplements have been neglected [4]. However, the modern lifestyle has seen a shift to working indoors with limited opportunities for exposure to ultraviolet (UV) rays which are essential for vitamin D synthesis. Thus, vitamin D must be supplied through food intake [11]. Studies reveal that blood concentration of 25(OH)D and the prevalence of 25(OH)D deficiency differs according to the sex, age, blood sampling time (season), and region [1124]. In the United States (U.S.) National Health and Nutrition Examination Survey, the rate of vitamin D deficiency (< 30 ng/mL) increased from 69% in 1988–1994 to 76% in 2001–2006 [11]. In the study of Korea Association of Health Promotion, only 17.1% men and 12.0% women had sufficient levels of vitamin D (> 30 ng/mL), suggesting that most people are afflicted with deficiency or insufficiency [24]. Accordingly, dietary reference intakes of vitamin D, which were determined in 2015, were included for revision in the 2020 dietary reference intakes for Koreans. This study aims to prepare the basis for determining vitamin D intake standards and suggestions to prevent chronic diseases in Koreans.
MATERIALS AND METHODS
Literature search
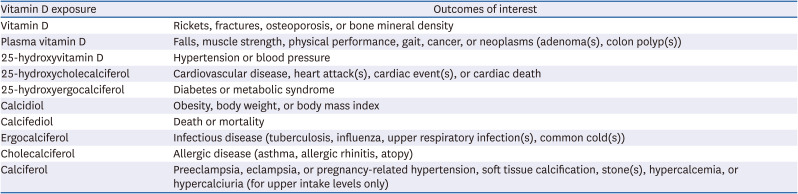
The literature search was conducted from April to September 2019. Papers published from January 2014 to December 2018 were searched. International databases such as PubMed, EMBASE, and Web of Science were used for articles published outside Korea. Korean databases included the National Digital Science Library, Korean Studies Direct Service System, and DBpia, and were used to search papers published in Korea. The selected keywords were 25(OH)D, parathyroid hormone, calcium, bone density, bone mass, fracture, rickets, osteomalacia, falls, physical activity, cancer, colon cancer, breast cancer, hypertension, myocardial infarction, cardiovascular disease, diabetes, obesity, metabolic syndrome, hypercalcemia, and hypercalciuria. The main inclusion criteria for selecting studies to establish the new dietary reference intake of vitamin D were as follows: ① effect of vitamin D intake on the blood levels of vitamin D (25(OH)D and 1,25(OH)2D); ② effect of 25(OH)D concentration in the blood on bone health, muscle and body functions, cardiovascular diseases, cancer, diabetes, metabolic syndrome, immune and infectious diseases, pregnancy, and total death; ③ effect of 25(OH)D concentration in the blood on mediating factors such as bone density and bone mass, blood pressure, blood sugar, and blood parathyroid hormone level; ④ effect of vitamin D on health outcomes through a mediating factor (Fig. 1). Articles included in the systematic literature review were selected by searching randomized controlled trials/intervention studies, cohort studies, nested case-control studies, case-control studies, cross-sectional studies, systematic reviews, and meta-analysis. Prioritization of studies was based on patient, intervention (or exposure), comparison, outcome, inclusion of a large number (60 or more) of healthy participants, an equal number of patient/control groups, and no missing results [25]. In addition, papers that assessed the effects of a single vitamin D nutrient and reported the effects of vitamin D on the outcome (Table 1) were prioritized for the final selection.
Fig. 1
Analysis tool for Vitamin D intake standards. Numbers in parentheses indicate the number of the main questions for selecting studies for new dietary reference intake of vitamin D: ① How does vitamin D intake affect blood levels of vitamin D (25(OH)D and 1,25(OH)2D)?; ② How does the concentration of 25(OH)D in the blood affect bone health, muscle and body function, cardiovascular disease, cancer, diabetes, metabolic syndrome, immune and infectious diseases, pregnancy, and total death?; ③ How does the concentration of 25(OH)D in the blood affect a mediating factor such as bone density and bone mass, blood pressure, blood sugar, and blood parathyroid hormone level?; ④ How does vitamin D affect the final health outcome through a mediating factor?
UVB, ultraviolet B; BMD, bone mineral density; BMC, bone mineral content; PTH, parathyroid hormone; CVD, cardiovascular disease.
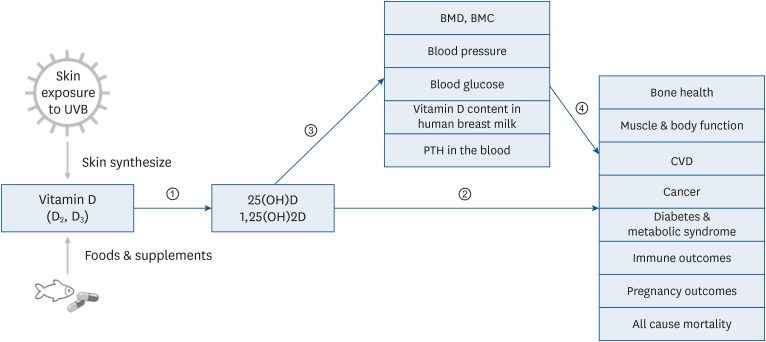
Table 1
Vitamin D and related diseases
Literature evaluation
For determining the quality of the selected studies, the scientific methods applied were evaluated through a systematic literature review [2627]. In order to maintain a transparent and consistent evaluation, we used the standard guidelines and forms developed by the 2020 Dietary Reference Intakes for Koreans (KDRIs) [26]. Works of literature were first selected by screening the abstract using the Rayyan program (https://rayyan-prod.qcri.org), followed by a second literature selection conducted by screening the entire text. To evaluate the quality of the study, the RoB 2.0 assessment form was used to extract data on purpose, study design, participants, results, basic information of the participants, appropriateness of the method for calculating the number of participants, explanation of participant selection and exclusion criteria, study period, follow-up period, follow-up appropriateness, dropout rate, statistical analysis, interpretation of the results, and correction for confusion factors [28]. Strength of evidence assessment was evaluated using the U.S. Department of Agriculture Nutrition Evidence Library Conclusion Statement Evaluation Criteria. Based on this assessment, studies were assigned as grades 1 to 4, signifying strong, moderate, limited, or grade not assignable, respectively (e.g., “strong evidence demonstrates” or “limited evidence suggests”) [29].
RESULTS
Literature characteristics for establishing dietary reference intakes of vitamin D
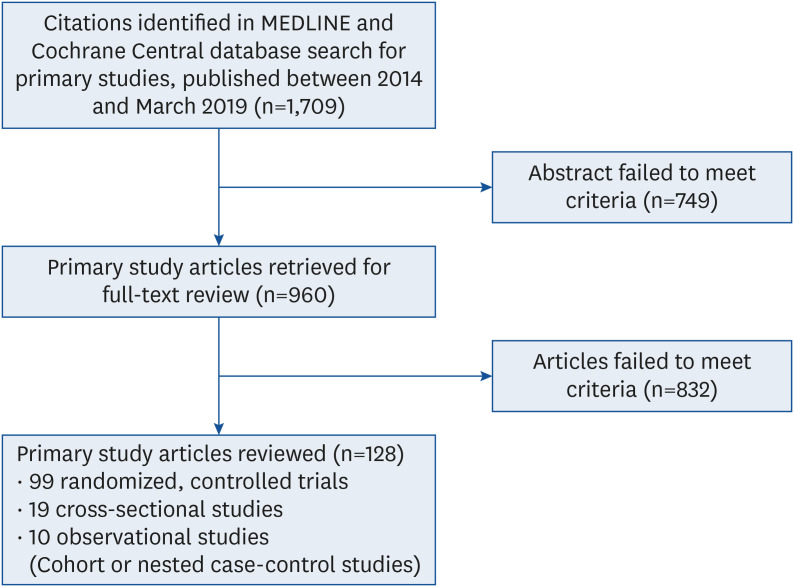
Totally, 1,709 studies were examined to revise the 2020 dietary reference intakes of vitamin D. Of these, 749 studies were excluded after the abstract screening, and 832 of the remaining 960 studies were excluded after reviewing for full-text screening. Ultimately, 128 studies were included in the final systematic review (Fig. 2).
A relatively large number of intervention studies and meta-analysis evaluated bone health (bone density, osteoporosis, and fracture) as outcome variables [183031]. However, most studies focused on postmenopausal women and the elderly, and there was a lack of studies for the younger age groups [323334]. A small number of intervention studies and meta-analysis used health indicators other than bone health (cancer, cardiovascular disease, diabetes, immune disease, and death) as outcome variables. Most studies were cohort and nested case-control studies. In such cases, most intervention studies analyzed health indicators other than bone health as secondary outcome variables rather than primary outcome variables. In particular, most Korean and Asian studies were case-control and cross-sectional types.
Data on the recently revised recommendation of vitamin D intake in Japan, which lies on the same latitude as Korea, was also included in the analysis. Based on the evidence to date, blood 25(OH)D concentrations and indicators of bone health (bone density/bone mass, calcium absorption, rickets, osteomalacia, and fracture risk) were included in the analysis to determine the dietary reference intake of vitamin D. Cancer, cardiovascular disease, hypertension, diabetes, metabolic syndrome, immune function, infectious disease, neurocognitive function, and pregnancy outcome were not used due to lack of evidence.
Blood vitamin D levels for establishing dietary reference intake of vitamin D
Vitamin D is not only absorbed through food intake, but is also produced in the skin following exposure to UV rays. However, since the serum level of 25(OH)D is an excellent indicator of bio-vitamin D obtained from both food intake and UV-induced production, blood 25(OH)D levels were also examined. The adequate level of vitamin D for bone health was determined to be within the range for the minimum parathyroid hormone and maximum calcium absorption. Since blood 25(OH)D and parathyroid hormone have an inverse relationship, a concentration of 20–30 ng/mL (50–75 nmol/L) was suggested, at which levels of the parathyroid hormone remain constant even if blood 25(OH)D levels increase [35].
The World Health Organization defines 25(OH)D levels lower than 20 ng/mL as insufficient [36]. Also, the U.S. Institute of Medicine reported that a blood level 20 ng/mL or more of 25(OH)D satisfies the required amount in 97.5% of the population, and any level lower than 12 ng/mL results in vitamin D deficiency [37]. Although there is no consensus on the optimal level of vitamin D in the body, 25–80 ng/mL is considered as adequate [38]. In the recently published “Guidelines for the Determination of Vitamin D Deficiency and Deficiency (Draft)” by the Japanese Society of Endocrinology and Japanese Society for Bone Metabolism, the levels 30 ng/mL or more, more than 20 ng/mL but less than 30 ng/mL, and less than 20 ng/mL, were defined as vitamin D adequacy, vitamin D insufficiency, and vitamin D deficiency, respectively [39] (Table 2).
Table 2
Comparison of vitamin D levels in the blood

| 25-hydroxy vitamin D (ng/mL) | World Health Organization, 2003 [32] | International Organization for Migration, 2011 [33] | Endocrine Society, 2017 (Okazake et al. [39]) |
|---|---|---|---|
| Deficiency | ≤ 10 | < 12 | < 20 |
| Insufficiency | 11–19 | 12–19 | 20–29 |
| Sufficiency | ≥ 20 | ≥ 20 | ≥ 30 |
A serum 25(OH)D concentration less than 12 ng/mL increases the risk of rickets (in children) and osteomalacia (in adults), reduces the calcium absorption rate and bone mass (in children and adults), and increases the risk of fracture (in the elderly) [211]. Therefore, as maximum effects of fracture prevention are observed at 20 ng/mL, the blood 25(OH)D level was set at 16 ng/mL and 20 ng/mL to satisfy the 50% (estimated average need) and 97.5% (recommended) of the required amount, respectively.
In 2,400 participants over the age of 10 yrs, the vitamin D level was measured from the 4th (2008) to 6th (2014) Korean National Health and Nutrition Examination Survey. The mean level of 25(OH)D showed less than 4% change from 2009 to 2013, which was relatively consistent. However, the mean level of 25(OH)D decreased from 19.2 ng/mL in 2008 to 17.8 ng/mL in 2009. Additionally, a significant decrease was obtained from 2013 (17.2 ng/mL) to 2014 (16.1 ng/mL). During the entire survey period, the blood concentration of 25(OH)D showed a decreasing trend in the entire population. Comparison of differences between genders revealed that the mean blood concentration of 25(OH)D determined annually was significantly higher in men than in women. However, the change in the average concentration of 25(OH)D decreased more rapidly in men than in women [40].
UV exposure time for vitamin D synthesis in the skin
Previous studies on the UV exposure time for vitamin D production were conducted in other countries on Caucasian skin types. Only a limited number of studies have investigated the UV exposure time for vitamin D production in Asian skin types. Studies in Korea have analyzed the time of UV ray exposure required for vitamin D synthesis, according to regions and seasons. In clean areas, 15, 12, 18, and 37 min exposure to UV rays are required during spring, summer, autumn, and winter, respectively, whereas in polluted areas, the time increases to 16, 16, 24, and 37 min exposure, respectively [41]. This is by considering the time required for the generation of erythema, as specified by the Korea Meteorological Administration. A total of 20 to 40 min of sunlight exposure per day is suggested for vitamin synthesis, without an outbreak of skin erythema. However, sunscreen products may affect vitamin D synthesis, and there is a high possibility of inadequate vitamin D synthesis subsequent to sunlight exposure.
Dietary reference intake of vitamin D by life cycle
The recommended dietary reference intake of calcium and vitamin D in the U.S. and Canada merely presents the amount of sufficient intake in 1997. The estimated average recommended amount and recommended intake were established only in 2011 [42]. However, since the same methodology used in the U.S. and Canada could be applied to establish the average required amount and recommended amount, only the sufficient intake amount was determined.
In Japan, the reference value for 25(OH)D concentration was set as 20 ng/mL. However, as a high proportion of the Japanese population was determined to have less than 20 ng/mL of 25(OH)D, the median value of 20 ng/mL could not be established as the value for a sufficient intake of 25(OH)D. Instead, sufficient intake amount was established using the minimum amount of vitamin D required that does not increase the risk of fracture [4344]. Therefore, the 2020 recommended level of vitamin D remained the same as the 2015 recommended level (presented in Table 3), based on the recommended amount in dietary reference intake of the U.S. and Canada, and on data obtained from Japan and studies published in Korea and other countries, vitamin D content in foods analyzed for intake level of Koreans, and the amount of sunlight and outdoor activity required per region.
Table 3
Adequate intake and tolerable upper intake level of Vitamin D by life cycle
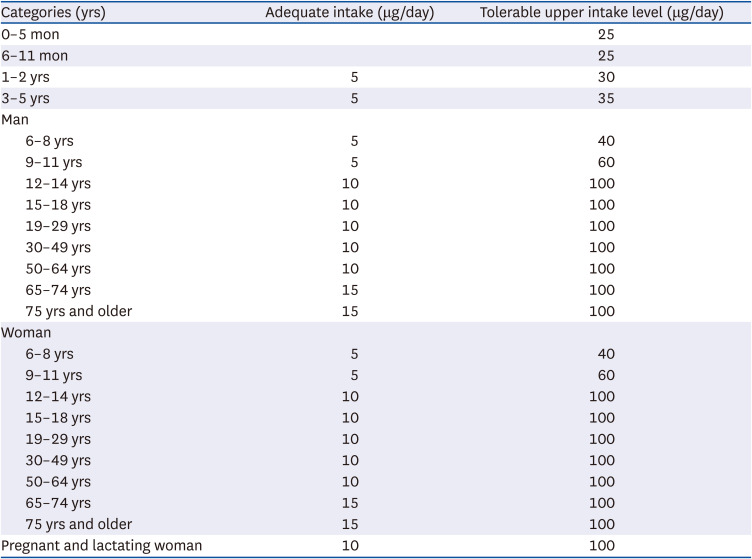
Vitamin D levels in infants under the age of 1 yr are affected by the mother's vitamin D level during pregnancy, and the amount of sunlight exposure and breast milk intake after birth. As breast milk contains a small amount of vitamin D, infants who do not obtain sufficient levels of vitamin D from sunlight must consume vitamin D from diet to prevent rickets. Therefore, the adequate intake level was set as 5 μg/day. In the growth period from the age of 1 to 18 yrs, children and adolescents do not acquire sufficient amount of UV rays and thereby have significantly insufficient levels of vitamin D [45]. Therefore, the adequate intake level of vitamin D during the growth period was set at 5 μg/day for children between the ages of 1 to 11 yrs, and 10 μg/day for children between the ages of 12 and 18 yrs.
Adults in the age group 19 and 64 yrs lack outdoor activities and have insufficient exposure to UV rays. Such lack of UV exposure is due to their lifestyle pattern. In particular, vitamin D deficiency is greater than 50% in the elderly over the age of 50 yrs, and especially in postmenopausal women. Thus, the adequate intake level was set at 10 μg/day vitamin D for musculoskeletal health and fracture prevention. For the elderly above 65 yrs, the adequate intake level was set to 15 μg/day for musculoskeletal health and prevention of various diseases.
Due to the increased calcium demand, pregnant women have an increased ability to produce calcitriol. However, they also show a decreased concentration of blood 25(OH)D due to the reduced amount of sunlight exposure during pregnancy. The transport of vitamin D from the mother to the fetus affects the growth rate of the fetus and newborns after birth [46]. According to the 2010 dietary reference intake for Koreans, the adequate intake level was established as 5 μg/day for adult women and 10 μg/day for pregnant women [47]. In the 2015 dietary reference intake for Koreans, the adequate intake level of 25(OH)D was set as 10 μg/day for both adult as well as pregnant women [48]. Lactating women experience hypocalcemia due to vitamin D deficiency from breastfeeding. Thus, the reference amount for breastfeeding infants must be established in consideration of preventing rickets. However, since studies have not indicated any additional evidence suggesting that the adequate intake levels of 25(OH)D differ for lactating and healthy women, the adequate intake level of 25(OH)D was set as 10 μg/day for lactating and healthy adult women [48].
The evidence for determining the tolerable upper intake level must consider not only acute toxic reactions due to excessive consumption, but also chronic side effects due to long-term high-dose intake. However, there is a lack of sufficient evidence for chronic excessive consumption [18]. Recently, there has been an increase in the population consuming a lower amount of vitamin D (that does not cause acute toxic reactions) but on high-dose vitamin D supplements for several years, indicating the necessity to evaluate the long-term health effects of high-dose ingestion of supplements. Additionally, since different sources of vitamin D may give rise to diverse side effects, there is a need to study the effects of supplement intake on the alterations in physiological responses through exposure to sunlight and response of 25(OH)D in the blood. Vitamin D poisoning, hypercalcemia, and hypercalciuria were used as indicators of adverse reactions caused by excessive vitamin D intake. A small number of studies evaluated the relationship between delayed growth, mortality rate, cancer, cardiovascular disease, falls, and fractures in infants; however, there is no indication of a clear causal relationship. Thus, these studies were not included in determining the tolerable upper intake level of vitamin D, which was set at 25–100 μg/day, according to the age group.
Main food sources for vitamin D
Unlike in the U.S. and Europe, food products containing vitamin D are not widely consumed by the public in Korea. Therefore, for adequate intake, food sources containing vitamin D must be actively included in meals. The total intake of vitamin D is the sum of the intake from diet and supplements. Natural sources of vitamin D include blue-backed fish, fish liver oil, and egg white. Among foods consumed by the Korean population, the number of food sources with high vitamin D content is limited. Fish, mushrooms, and eggs are food sources with high vitamin D content (Table 4). Additionally, milk, cheese, and yogurt fortified with vitamin D are also good sources. The adequate intake of vitamin D for Koreans is suggested at 10 µg. For elder individuals with decreased bone density, the recommended intake level is 15 µg. A total of 60 g of animal products (such as 1 egg, or 1 helping of salmon and herring) can help to reach the daily required intake level. Vitamin D-fortified food products were first produced in some countries after the importance of vitamin D for the prevention of rickets was reported in the 1920s [49]. Currently, in the U.S., vitamin D food fortification is voluntarily conducted. Most milk contains 385 IU of vitamin D per liter [50]. As per the Food and Drug Act in Canada, vitamin D must be fortified in milk and all plant-based beverages (35–45 IU of vitamin D per 100 mL) and margarine (530 IU per 100 g) [18]. In Korea, some dairy products fortified with vitamin D are currently produced autonomously. The level of fortification varies depending on the products; however, supplementation is approximately 36% of the standard intake level, which corresponds to 1.5–41.8 μg (35–836% of daily nutritional intake) [51].
Table 4
Main food source of vitamin D and its content1)
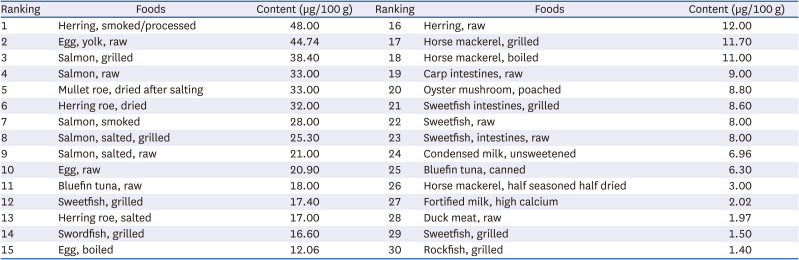
1)The Korean food composition database 9.1 [51].
DISCUSSION
The distribution of daily intake of vitamin D varies greatly, depending on individual factors or regional factors. Moreover, the daily vitamin D intake status and lifestyle behaviors are important variables since sources of vitamin D other than foods are also critical variables. Since the sources of vitamin D include food products and synthesis from sunlight exposure, it is challenging to calculate the appropriate required amount of vitamin D intake. For these reasons, the level of vitamin D in the Korean population is likely to be deficient or insufficient. Analysis of numerous studies to establish dietary reference intakes of vitamin D revealed that cross-sectional studies on the relationship between fracture risk and blood 25(OH)D concentration had been conducted in Korea. Very few studies assessed vitamin D intake concurrently, and a limited number of intervention studies examined for the prevention of fractures. However, in other counties, several large-scale clinical studies have been conducted, and their findings indicate that vitamin D intake levels of 10 μg/day is ineffective, but approximately 20 μg/day helps to prevent proximal femur fractures [52]. Furthermore, vitamin D deficiency in osteoporotic patients results in a negative calcium balance, which leads to secondary hyperparathyroidism and thereby an increased risk of fracture. Recent findings suggest that vitamin D affects the risk of fractures as well as osteoporosis. In particular, such effects of vitamin D are greater in the elderly. However, there is insufficient scientific evidence that determines an adequate amount of vitamin D required to prevent aggravation of the risk, and hence, the relevant contents cannot be used. Further studies indicate that vitamin D helps in maintaining muscle strength, and vitamin D deficiency has been suggested as a risk of falls. In a cohort study of 1,393 Japanese women over the age of 75, logistic regression analysis using conduction as an evaluation index showed that subjects with a blood concentration of 25(OH)D greater than 25 ng/mL had significantly higher muscular strength, as compared to individuals with levels below 20 ng/mL [53]. As most osteoporotic fractures (other than vertebral fractures) are caused by falls, vitamin D may act on bones and skeletal muscles to prevent fractures. However, since the scientific evidence to establish the amount of vitamin D required to prevent such skeletal and muscle weakness is insufficient, the relevant contents cannot be used. To prevent aging-associated loss of bone and muscle strength, it is essential to acquire an adequate amount of sunlight for vitamin D synthesis.
Considering all the above data, the dietary reference intakes of vitamin D remained the same as the values established in 2020 based on the recommended amount present in the dietary reference intake from the U.S. and Canada, data from studies in Japan, and the searched literatures published in Korea and other countries. Moreover, the vitamin D intake level and outdoor activity level of Koreans have remained unchanged compared to the evidence presented in 2015 and were not modified in the new standards. Based on the analysis of vitamin D content in food and the amount of sunlight and outdoor activity levels by region, the 2015 dietary reference intakes were not changed [48].
Currently, in Korea, there is insufficient data on blood vitamin D levels, synthesis of vitamin D from sunlight, and vitamin D intakes from natural food products, fortified foods, and nutritional health functional foods. Therefore, sufficient intake level rather than the recommended intake level was established. As this level was set based on the critical concentration of vitamin D, the dietary reference intakes must be considered in the management of diet and clinical practice. Additionally, the tolerable upper intake level also needs to be carefully considered.
CONCLUSION
In summary, the same dietary reference intakes of vitamin D established in the 2015 KDRI were suggested in the 2020 KDRI. A critical concentration of vitamin D was suggested as the sufficient level for Koreans (20–30 ng/mL). This is the same as the 2015 vitamin D dietary reference intake set at 10 μg/day for Korean adults. The level was determined based on the evidence from reliable and valid studies conducted in Korea and other countries. In addition, vitamin D synthesis is deficient in adolescents and adults due to their lack of outdoor activities. Therefore, in 2025, more accurate data on the vitamin D content of foods and the synthesis of vitamin D from UV rays through outdoor activities are required. Furthermore, meals must be adequately planned to meet the 2015 and 2020 vitamin D intake levels of 10 μg/day. Vitamin D deficiency is associated with chronic diseases, and the current level of vitamin D intake is a huge concern. Meals must be carefully designed for realistic solutions to overcome such challenges. It is therefore imperative to obtain reliable data on the correlation between exposure time to sunlight (including outdoor activities), vitamin D intake, and serum 25(OH)D concentration in Koreans.
 XML Download
XML Download