

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Breastmilk has been long esteemed the gold standard for infant nutrition, providing a wealth of essential nutrients and bioactive components to support proper growth and development during the first 1,000 days. The World Health Organization (WHO) currently advises exclusive breastfeeding up to 6 mon [1], but this is not always feasible due to problems such as difficulties with lactation, poor hospital practices, and various cultural barriers [234]. In such instances, formulas are given instead.
Among the available formulas, the preferred formula for infants with gastrointestinal issues or a family history of allergies is the hydrolyzed formula [5678]. Cow's milk allergy (CMA) is one of the most common food allergies in young children, affecting 2–3% of the pediatric population [9]. Hypoallergenic formula is recommended for infants with CMA who are not breastfeeding [10]. Extensively hydrolyzed formulas are tolerated in over 90% of infants with CMA [10]. However, extensively hydrolyzed formula cost more than standard cow's milk formulas (SFs) and are less palatable [10]. Partially hydrolyzed formula (PHF) is currently not recommended for patients with CMA [10]. However, some European studies evaluating the allergenicity of infant formulas reported that 40–60% of patients with CMA can tolerate PHF [111213].
Hydrolyzed formula possesses a nutritional profile comparable to that of SF, though it has been enzymatically treated with hydrolase to yield peptides that are more easily digested and less allergenic [141516]. Depending on the degree of hydrolysis and molecular weights of the resultant peptides, hydrolyzed formula can be classified into PHF which have peptides of 3–10 kDa or extensively hydrolyzed formula which is composed of > 90% of peptides with molecular weight of < 3 kDa [17]. The world's first PHF was made with a hydrolyzed whey protein with a molecular weight of 3–10 kDa in 1985 [14]. The PHF have been reported to be effective in supporting adequate growth, and reducing the risk of atopic dermatitis [181920].
Pediatricians generally recommend PHF for satisfying an infant's nutritional requirements throughout the early postnatal period for infants who have difficulty to digest [5721]. Additionally, for infants having a family history of allergy, PHF may reduce the risk of developing allergy [822]. The early stage of life has tremendous impact on infant's growth and development and therefore, supplementation of adequate nutrients is crucial. The purpose of this study was to investigate the effects of PHF on health indicators and growth in infants who were at high-risk of allergic disease and potential candidates for consuming PHF.
SUBJECTS AND METHODS
Subjects
Subjects were recruited from 6 tertiary hospitals. Eligibility criteria included infants below 2 mon of age, exclusively feeding on formula, having at least one first-degree family member with allergies, being born ≥ 34 weeks' gestation, and weighing ≥ 2,500 g at birth (including ≥ 2,000 g of multiple births). Exclusion criteria consisted of consuming formulas other than PHF or SF 3 weeks prior to the study having a chronic disease, congenital or acquired immunodeficiency syndrome, and/or experiencing an allergic reaction to the study's formulas within the first 2 weeks of the study.
Study design and protocol
This was a prospective, multicenter, controlled trial. Upon enrollment, infants’ birth weight, height, and family history of allergies, as well as the presence of a pet and individuals who smoked at home, were recorded. Anthropometrics were measured by trained personnel at baseline, 12 weeks, and 24 weeks of age. Weight-for-age, height-for-age, and weight-for-height were calculated using the WHO's infant growth chart [23]. Blood samples were tested to assess levels of white blood cells, hemoglobin, ferritin, protein, albumin, aspartate aminotransferase, alanine aminotransferase, eosinophil cationic protein, total immunoglobulin E (IgE), as well as cow's milk-, soy-, alpha-lactalbumin-, beta-lactoglobulin-, and casein-specific IgE (ImmunoCAP; Thermofisher scientific, Uppsala, Sweden) at 24 weeks of age.
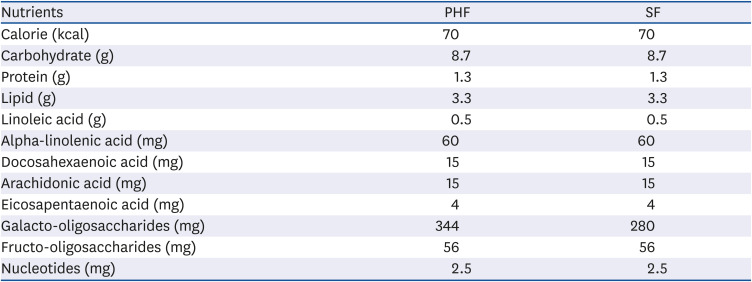
PHF (Absolute Sensitive®; Maeil Dairies Co., Ltd., Pyeongtaek, Korea) or SF (Absolute Myungjak®; Maeil Dairies Co., Ltd.), supplemented with docosahexaenoic and arachidonic acids, was given to infants by order of enrollment (Table 1). Both formulas provided adequate nutrients and were almost identical to each other, except the degree of hydrolysis of protein and the amount of galacto-oligosaccharides. PHF contains hydrolyzed whey protein for better digestibility. Compared to SF, an intact cow's milk protein formula, PHF reduced allergenicity. All caregivers were instructed to feed their infants as many times a day as needed until 24 weeks of age.
Table 1
Composition of the study formulas
Ethics
The study was performed in accordance with the Declaration of Helsinki statement. All procedures were approved by the Institutional Review Board at Ajou University School of Medicine (AJIRB-MED-OBS-14-444), Inha University Hospital (INH-IRB15-0921), Hallym University Sacred Heart Hospital, Hallym University College of Medicine (2015-I092), Yonsei University College of Medicine (Gangnam, 2015-0008-001; Sinchon, 4-2015-0827), and Soonchunhyang University Hospital (2014-12-028). Caregivers provided written informed consent to participate in the study.
Statistical analysis
Results are listed on a per-protocol basis. Continuous variables are presented as median (interquartile range), and categorical variables as counts and percentages. The continuous and categorical variables were compared by the Mann-Whitney U test and Fisher's exact test, respectively. Differences in anthropometric measures between the groups were determined using Mann-Whitney U test. For the multiple comparisons of subgroup regarding sex, the significance was verified at P = 0.05/2 = 0.025 by applying the Bonferroni correction. Statistical analyses were conducted with SPSS (version 25, IBM Statistics; IBM Corp., New York, NY, USA), and P < 0.05 was considered statistically significant.
RESULTS
Baseline characteristics
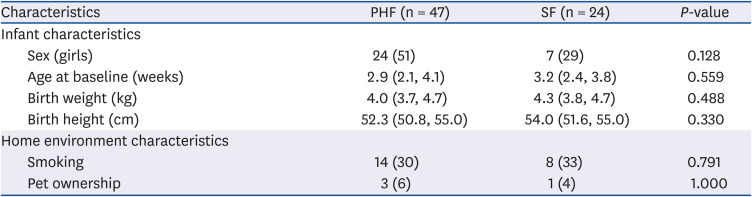
Eighty-three infants (56 in PHF group, 27 in SF group) participated in the study, 4 (2 in PHF group, 2 in SF group) withdrew, 2 (1 in PHF group, 1 in SF group) dropped out, and 2 (1 in PHF group, 1 in SF group) failed to complete the study because their caregivers refused the blood analysis. Subjects were randomly recruited in each group from the beginning of the study; however, due to difficulties in recruitment, the PHF group was recruited earlier than the SF group during the study period. Of the 79 infants who completed the study (54 in PHF group, 25 in SF group), 8 (7 in PHF group, 1 in SF group) were excluded from the final analysis because of missing data at 24 weeks of age, resulting in a final count of 71 (Fig. 1). No significant differences in age, sex, birth weight and height, or the home environment were observed between the groups (Table 2).
Fig. 1
Flow diagram of the study participants.
PHF, partially hydrolyzed formula; SF, standard cow's milk formula.
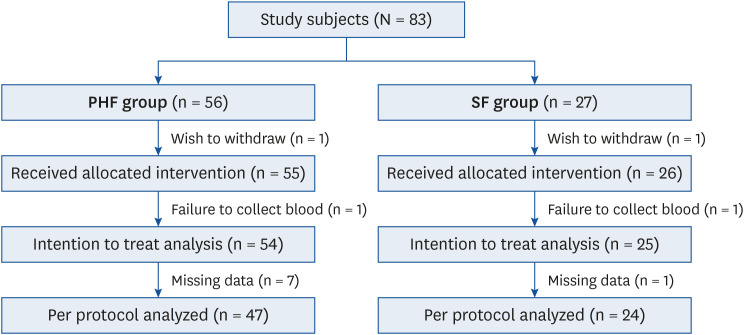
Table 2
Baseline characteristics according to formula groups
Formula intakes and tolerance
Throughout the study period, there were no symptoms of food intolerance such as diarrhea, constipation, or refusal of intake in each group. The PHF and SF were well accepted by the infants, and there was no difference in adverse food reaction between the 2 formulas.
Anthropometric measures
There were no significant group effects or group-by-time interactions at baseline, 12 weeks, and 24 weeks of age for weight, height between the groups (Table 3). There were no significant differences in weight, height, and weight-for-height at baseline, 12 weeks, and 24 weeks of age in each sex between the PHF and SF groups. At baseline, weight-for-age z-score was higher in the PHF group; however, at 24 weeks of age, it was higher in the SF group and boys' subgroup. At 24 weeks of age, the weight-for-age and height-for-age z-scores of the SF group were higher than those of the PHF group, but there was no significant difference in the weight-for-height z-score. As a result of difference from baseline to 24 weeks of age, weight-for-age and height-for-age z-scores were higher in SF than PHF group, but there was no significant difference in the weight-for-height z-score (Table 4).
Table 3
Anthropometric measures at baseline, 12 weeks, and 24 weeks of age
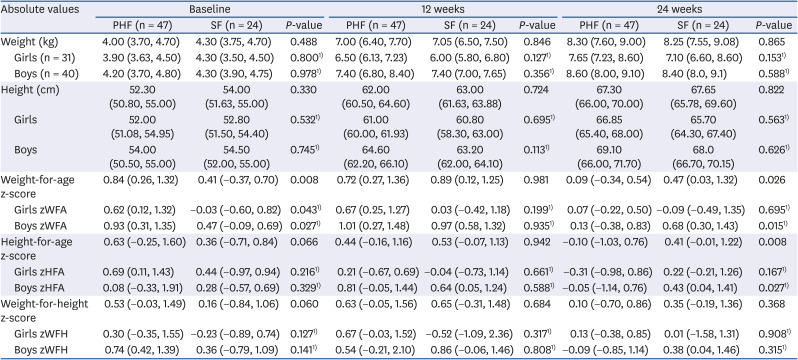
Data are presented as median (interquartile range).
P-values were derived from Mann-Whitney U test.
PHF, partially hydrolyzed formula; SF, standard cow's milk formula; zWFA, weight-for-age z-score; zHFA, height-for-age z-score; zWFH, weight-for-height z-score.
1)The significance was verified at P = 0.025 by applying the Bonferroni correction.
Table 4
Changes of anthropometric measures from baseline to 24 weeks of age
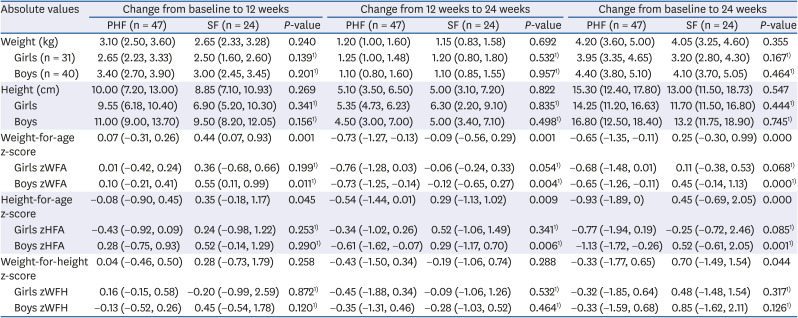
Data are presented as median (interquartile range).
P-values were derived from Mann-Whitney U test.
PHF, partially hydrolyzed formula; SF, standard cow's milk formula; zWFA, weight-for-age z-score; zHFA, height-for-age z-score; zWFH, weight-for-height z-score.
1)The significance was verified at P = 0.025 by applying the Bonferroni correction.
Laboratory parameters and atopic dermatitis
At 24 weeks of age, the total counts and proportions of white blood cells and levels of hemoglobin, ferritin, total protein, albumin, aspartate aminotransferase, alanine aminotransferase, eosinophil cationic protein, as well as total IgE, cow's milk-, soy-, alpha-lactalbumin-, beta-lactoglobulin-, and casein-specific IgE did not reveal statistically significant differences between the groups (Table 5).
Table 5
Laboratory parameters at 24 weeks of age
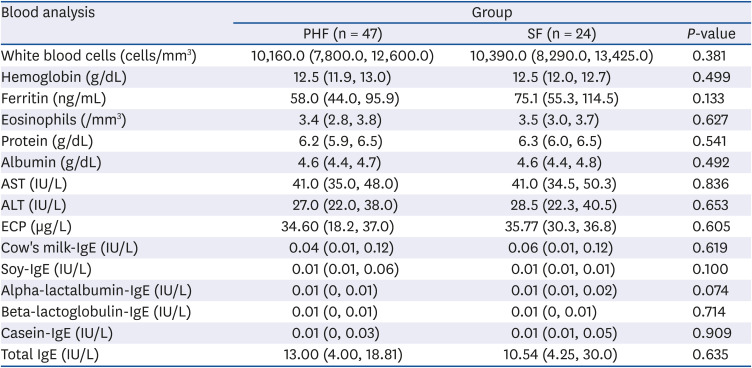
Data are presented as median (interquartile range).
Comparison of continuous variables was calculated using Mann-Whitney U test.
PHF, partially hydrolyzed formula; SF, standard cow's milk formula; AST, aspartate aminotransferase; ALT, alanine aminotransferase; ECP, eosinophil cationic protein; IgE, immunoglobulin E; IU, international units.
None of the infants had moderate-to-severe atopic dermatitis caused by CMA during the study period.
DISCUSSION
This study revealed that the growth and health indicators of PHF-fed infants were comparable to those of SF-fed infants during the first 6 mon of life. These results suggest that PHF may provide normal growth for infants who have difficulty with SF due to disorders such as CMA or malabsorption, which are consistent with previous results [181920]. In addition, we found that cow's milk-based formula, whether SF or PHF did not cause atopic dermatitis in early infancy.
At baseline, 12 weeks and 24 weeks of age, there were no significant differences in weight, height, and weight-for-height in each sex between the PHF and SF groups. This study found that infants in both groups grew up adequately. However, when looking at the mean change of growh parameter from baseline to 24 weeks of age, both weight-for-age and height-for-age z-scores were higher in the SF group than those in the PHF group, and higher the boys' group compared to the girls' group. At baseline, the weight-for-age z-score was higher in the PHF group, but at 24 weeks of age, it was higher in the SF group. The male infants were more in the SF group than the PHF group (71% vs. 49%) and the weight-for-age z-score was higher in the boys' group compared to the girls' group. Therefore, we presumed that the SF group gained more weight than the PHF group because more male infants were in the SF group.
In this study, none of the infants developed atopic dermatitis during 24 weeks of age. All subjects did not develop CMA. Cow's milk antigens usually cause the first allergic responsiveness in infancy. In addition, atopic dermatitis can be considered a possible skin symptom of CMA since atopic dermatitis and food allergy often occur together in early childhood. Therefore, we included specific IgE to cow's milk and incidence of atopic dermatitis in outcome measures and found that none of subjects developed a CMA or atopic dermatitis. These findings are consistent with the results that early introduction of allergenic foods such as egg or peanut are associated reduced risk of developing food allergy [2425]. The results from recent cohort study and a randomized trial of early exposure to milk protein in the diet of breastfed infant have shown that the incidence for IgE-mediated CMA could be as low as 0.5% [262728].
These infant formulas are produced in accordance with the regulations under strict hygienic conditions, and commercially available. Both formulas provided adequate levels of nutrients and were almost identical apart from hydrolysis of protein. The PHF was composed of whey protein hydrolysate hydrolyzed by enzymes to increase digestibility. It has been specifically developed to reduce common feeding problems and enhance tolerability in formula-fed infants.
Although the guidelines on infant feeding have changed over the decades, PHF has been available and used worldwide for a long time [2930]. For high-risk infants who cannot be exclusively breastfed for 4–6 mon of age, the hydrolyzed formulas have been reported to decrease atopic dermatitis [83132]. However, recent meta-analysis does not provide strong evidence for PHF's protective effect on prevention of allergy development in non-breastfed high-risk infants [1633]. Thus, the British Society for Allergy and Clinical Immunology encourages parents to feed SF rather than hypoallergenic formula in infants who can tolerate cow's milk [34]. Recently, the PHF has been repositioned from products that reduce allergic reactions in high-risk infants to the products that reduce the crying time or episodes of regurgitation in infants with discomfort to SF.
The first 1,000 days in infants critical, characterized by rapid brain growth and development. Human milk is the golden standard of nutrition for infants during the first 1,000 days of life. However, exclusive breastfeeding is not always possible for infants and parents. Therefore, there are a lot of infant formula products chosen by caregivers' needs. PHF is generally used for healthy infant, infant who felt discomfort, or high-risk infants according to the recommendations and guidelines.
This study was a controlled trial in Korea which evaluated the effects of formula feeding. However, there were some limitations. First, we could not enroll infants who were exclusively breastfed. However, in real world, it is very difficult to extensively breastfeed infants up to 24 weeks in order to exclude the effects of formula feeding. Secondly, this was not a blinded study; the formulas provided to infants were disclosed to caregivers. Thirdly, we were unable to recruit our target number of high-risk infants, therefore the number of subjects was not similar between groups. Our inclusion criteria were too strict to enroll. It was difficult to recruit infants younger than 2 mon of age who were not breastfed at any time during the study period, and recruiting infants having at least one first-degree family member with allergies was even harder. Because enrollment was difficult, and available data in SF were more, we recruited the PHF group first and then the SF group later. However, there were no differences in general characteristics of both groups. Moreover, despite these limitations, the obtained data were sufficient for comparative analyses. Finally, because we could not record the amount of formula consumed by each infant, we were unable to determine whether the infants who consumed more formula showed higher growth. However, we evaluated an overall growth pattern in infants who were fed formulas as much as they wanted. In addition, when we checked the amount of formula consumed by the infants in each formula group, infants in both groups consumed similar amounts.
In conclusion, this study demonstrated that not only PHF but also SF was well-accepted by infants who were at high-risk of allergic disease and potential candidates for consuming PHF, resulting in normal growth and hematological parameters up to 24 weeks of age. Therefore, infants who are unable to tolerate SF can be fed PHF without nutritional concerns about growth. If we evaluate the growth and development of infants who participated in this study later, we will be able to evaluate the differences of them between infants fed PHF and those SF in the early stage of life.
 XML Download
XML Download