

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer (CRC) is the third most commonly diagnosed cancer and the second leading cause of cancer-related deaths worldwide.1 The incidence of CRC is known to be high in developed countries, and its incidence is increasing in Asia as socioeconomic development progresses. South Korea has the second highest incidence of CRC worldwide with 44.5 cases per 100,000 persons per year.2 With well-recognized risk factors such as aging, alcohol consumption, smoking, obesity, and family history, lifestyle changes in diets or in work patterns are emerging as risk factors for CRC.34
Recent evidence suggests that sedentary behavior (SB) can increase the risk of chronic diseases including CRC.5 SB is a concept separate from physical inactivity and refers to all activities with an energy expenditure of ≤ 1.5 metabolic equivalents of task, such as sitting, reclining, or lying postures.6 Modern individuals spend their time sitting while watching TV, reading, driving, and using computers in an office or at home. A review article estimated that adults in Korea spend 8.3 hours per day in SB, which was much higher than the standard recommended sedentary time in Korea and other countries.7 Previous studies have reported that the risk of chronic disease increases with increased SB.8 In addition to SB, physical activity (PA) is well-known for health-related lifestyle benefits, and may also influence the development of CRC.910 PA refers to any kind of body movement that requires energy expenditure, and can be classified into four domains: leisure-time PA (LTPA), occupational PA (OPA), domestic PA, and transportation PA (TPA).11 Both SB and PA are modifiable lifestyle-related factors, so interventions to correct them have significant potential in reducing the burden of cancer worldwide.
The relationship between PA, SB, and CRC requires a deeper understanding. First, the types of PA can have different effects on health. For example, LTPA has been consistently shown to have a favorable health effect, whereas OPA was often reported to have adverse effects on health.1213 It is necessary to study whether this phenomenon, termed the “PA health paradox,” also applies to CRC. Second, it is essential to include both SB and PA when estimating their association with CRC. This is because some office workers who spend much time in SB at work can meet PA standards after work. Conversely, manual workers who have less SB but enough OPA at work due to strenuous physical labor may spend much time in SB after work. To our knowledge, no study has analyzed how the association of SB with CRC varies with different types of PA. Therefore, this study aimed to investigate the association of SB and different types of PA with the risk of CRC.
METHODS
Data and participants
This cross-sectional study was conducted in November 2021, based on the Korea National Health and Nutrition Examination Survey (KNHANES) data VI–VIII collected by the Korea Centers for Disease Control Prevention (KCDC) from 2014 to 2019. KNHANES is conducted annually to assess the health and nutritional status of the Korean population.
A total of 47,309 participants were identified from the data from 2014 to 2019. A final sample of 33,403 participants was selected which included all adults aged ≥ 20 years old with complete information on PA, SB, and CRC. Participants with missing values for PA (n = 2,028) and CRC (n = 2,060) were excluded.
Measurements
For CRC, participants were asked if they had ever been diagnosed with CRC by a physician. Those who had not been diagnosed with CRC were included in the non-CRC group. SB and PA were evaluated using the Global Physical Activity Questionnaire (GPAQ) as a part of the KNHANES. The GPAQ was devised by the WHO and consisted of a self-reported questionnaire on OPA, LTPA, TPA, and SB.14 The validity and reliability of the Korean version has been verified.15 SB was evaluated by asking the question, “Except for sleeping time, how many hours a day do you usually spend sitting or reclining?” In this study, SB was dichotomized into < 10 hours and ≥ 10 hours modifying the criteria of a previous study in Korea.16
PA was defined based on the questions on OPA, LTPA, and TPA of the GPAQ. In these questions, “vigorous-intensity activity” referred to PA that required strenuous physical efforts and significantly increased breathing or heart rate, whereas “moderate-intensity activity” referred to PA that required moderate physical effort and slightly increased breathing or heart rate. The WHO recommended standard for PA in adults is ≥ 150 minutes of moderate-intensity activity per week or ≥ 75 minutes of vigorous-intensity activity per week.17 Therefore, those who engaged in ≥150 minutes of moderate-intensity activity per week or ≥ 75 minutes of vigorous-intensity activity per week were defined as participants of PA in both OPA and LTPA.18 TPA was defined as physical activity such as walking or cycling for ≥ 150 minutes per week when moving from place to place, except for work-related movement. If any one of the above three types of PA was performed, it was defined as any PA (+), and if no PA was performed, it was classified as any PA (−). Also, four groups were created using any PA and SB as combined variables: 1) SB (−) and PA (+) as the reference group, 2) SB (−) and PA (−), 3) SB (+) and PA (+), and 4) SB (+) and PA (−).
This study included the following demographic and health-related factors: age group (20–29, 30–39, 40–49, 50–59, ≥ 60 years), sex (male or female), marital status (married or other [divorced, single, widowed]), obesity (body mass index ≥ 25 or < 25 kg/m2), income level (high, mid-high, mid-low, and low), educational level (middle school or lower, high school, college or higher), smoking status (current smoker, ex/non-smoker), binge drinking, presence of cancer (any cancer except for CRC), and chronic disease (hypertension, diabetes, dyslipidemia, and cardiovascular disease). Binge drinking was defined as intake of ≥ 7 drinks for men or ≥ 5 drinks for women at least twice a week during the past year.
Statistical analysis
The χ2 tests were performed to analyze the relationship between CRC and the demographic and health-related variables. Multiple logistic regression analysis was used to determine the odds ratios (ORs) and 95% confidence intervals (CIs) of SB and different types of PA for CRC risk, after adjusting covariates included age, sex, marital status, obesity, smoking status, educational level, chronic diseases, and cancer diagnosis. Finally, to investigate the combined effect of SB and PA on the risk of CRC, ORs and 95% CIs for CRC risk were calculated according to the four groups of combined SB and PA. All analyses were performed using IBM SPSS Statistics for Windows ver. 25.0 (IBM Corp., Armonk, NY, USA), and statistical significance was set at P < 0.05.
RESULTS
Table 1 shows the association of CRC prevalence and participant demographics and health-related factors. The prevalence of CRC was significantly associated with male sex, older age, being married, obesity, being a non- or ex-smoker, lower educational level, the presence of chronic disease or cancer, and sitting time of ≥ 10 hr/day. However, binge drinking, income level, and all types of PA were not significantly associated with CRC.
Table 1
Association between general characteristics and CRC prevalence
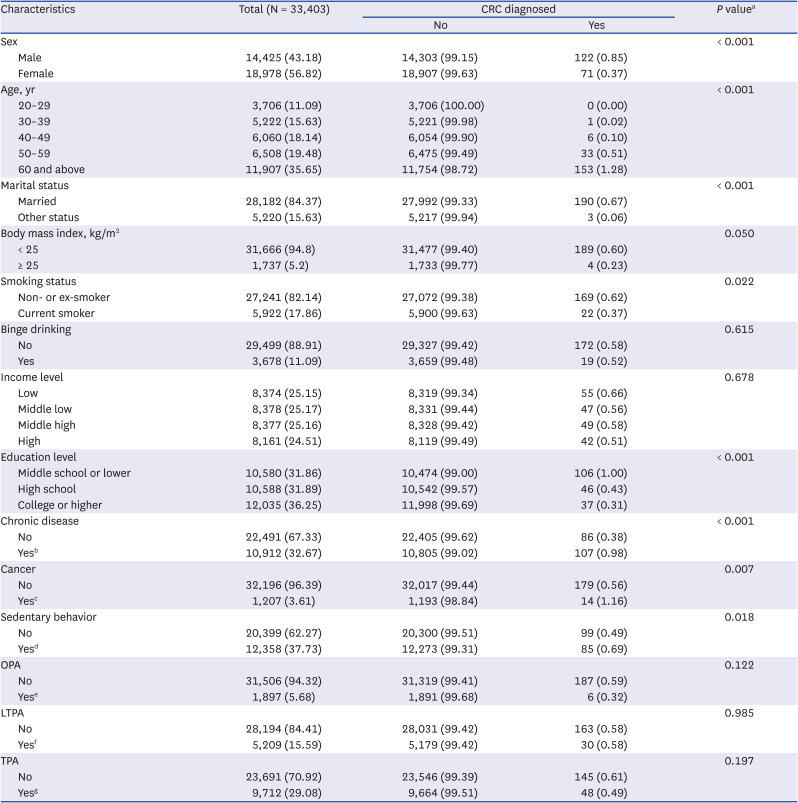
CRC = colorectal cancer, OPA = occupational physical activity, LTPA = leisure-time physical activity, TPA = transportation physical activity, PA = physical activity.
a
P value from χ2 test.
bHaving any chronic diseases including hypertension, diabetes, dyslipidemia, and cardiovascular disease diagnosed by a physician.
cHaving any cancers including stomach, liver, uterine cervical, breast, lung, and thyroid cancer diagnosed by physician.
dSitting time ≥ 10 hr/day.
eDoing ≥ 150 minutes of moderate PA or ≥ 75 minutes of vigorous PA in a week at work.
fDoing ≥ 150 minutes of moderate PA or ≥ 75 minutes of vigorous PA in a week during leisure time.
gDoing ≥ 150 minutes of PA in a week during transportation.
Table 2 shows the Ors for the association between SB, different types of PA, and CRC. In a fully adjusted model, SB was significantly associated with an increased risk of CRC (OR, 1.62; 95% CI, 1.20–2.17). However, different types of PA such as OPA, LTPA, and TPA were not significantly associated with CRC risk. Any PA of at least one of the above three activity types was also not associated with CRC risk.
Table 2
Association of colorectal cancer risk with sedentary behavior and PA
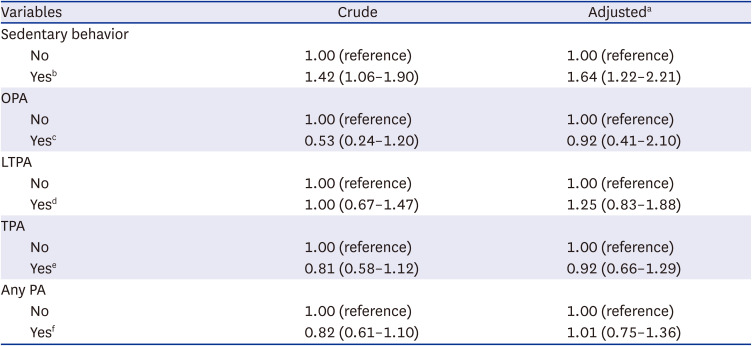
PA = physical activity, OPA = occupational physical activity, LTPA = leisure-time physical activity, TPA = transportation physical activity.
aAdjusted covariates included sex, age, marital status, obesity, smoking status, educational level, having chronic diseases and cancer.
bSitting time ≥ 10 hr/day.
cDoing ≥ 150 minutes of moderate PA or ≥ 75 minutes of vigorous PA in a week at work.
dDoing ≥ 150 minutes of moderate PA or ≥ 75 minutes of vigorous PA in a week during leisure time.
eDoing ≥ 150 minutes of PA in a week during transportation.
fPerforming at least one of three types of PA, including OPA, LTPA, or TPA.
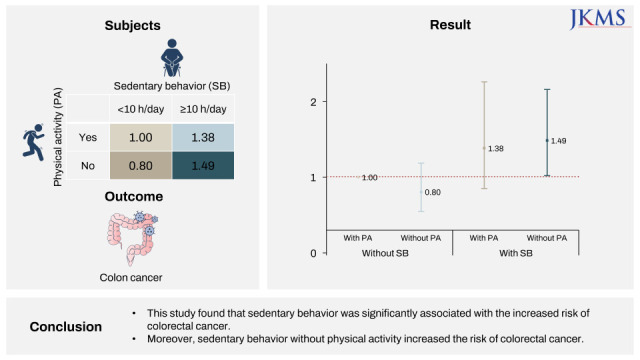
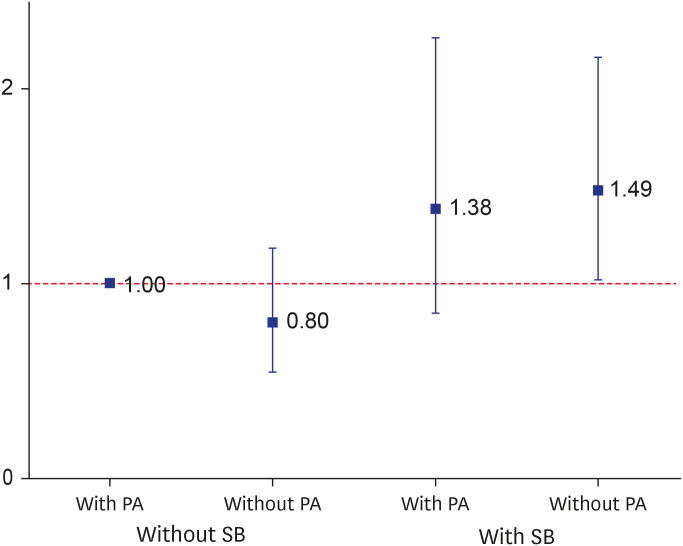
Table 3 describes the risk of CRC according to four categories using SB and PA as combined variables. Compared to the reference group without SB and with PA, those with SB and without PA were significantly associated with an increased risk of CRC (OR, 1.49; 95% CI, 1.02–2.16). The other two groups did not show a significant association with CRC risk (Fig. 1).
Table 3
Combined effect of SB and PA on colorectal cancer risk

| SBa | PAb | Crude | Adjustedc |
|---|---|---|---|
| No | Yes | 1.00 (reference) | 1.00 (reference) |
| No | No | 1.31 (0.90–1.91) | 0.80 (0.55–1.18) |
| Yes | Yes | 1.30 (0.80–2.10) | 1.38 (0.85–2.26) |
| Yes | No | 1.91 (1.33–2.75) | 1.49 (1.02–2.16) |
SB = sedentary behavior, PA = physical activity.
aSitting time ≥ 10 hr/day.
bPerforming at least one of three types of PA, including occupational PA, leisure-time PA, or transportation PA.
cAdjusted covariates included sex, age, marital status, obesity, smoking status, educational level, having chronic diseases and cancer.
DISCUSSION
This study has several important findings. First, SB was associated with an increased risk of CRC, while each type of PA was not associated with an increased risk of CRC. Second, those with SB and without any PA showed an increased risk of CRC as compared to those without SB and with PA. This relationship was seen in those with sitting time ≥ 10 hr/day and engagement in at least one kind of PA, regardless of whether it was LTPA, OPA, or TPA. The findings of this study suggest that with reduced sitting time, higher PA levels can reduce the risk of CRC regardless of the type of PA.
Although few previous studies on the association between SB and CRC varied by PA could be found, high PA levels was reported to alter the relationship between SB and overall cancer risk.19 More importantly, a Japanese study investigated the effect of modification of LTPA levels on the relationship between SB and CRC mortality.20 The authors found that time spent watching television was significantly associated with the risk of CRC only among those with high levels of LTPA, and thus assumed that low levels of LTPA had a greater effect on CRC mortality than SB.
SB has mainly been reported to be associated with an increased risk of CRC,21 but several studies have also reported no association.2223 However, this study found a strong association between SB and the increased risk of CRC that had a dose-response relationship wherein each 1-hour increment in sitting time per day was related to a 6% increased risk of CRC (OR, 1.06; 95% CI, 1.02–1.10) (data not shown).
Although each type of PA did not show a significant association with CRC risk in this study, there is strong evidence that PA has a protective effect against the development of CRC.24 Furthermore, diverse subdomains, such as LTPA, OPA, and TPA, have been established to lower the risk of CRC.25 Therefore, it can be inferred that a wide range of PAs can reduce the risk of CRC.
Several possible mechanisms have been suggested to explain the association between SB, PA, and CRC. First, prolonged SB and reduced PA can induce metabolic dysfunction, such as insulin resistance, which may lead to hyperinsulinemia and hyperglycemia.26 Hyperinsulinemia plays a role in tumorigenesis by activating insulin-like growth factor 1, and the hyperglycemic environment contributes to tumor cell proliferation by upregulation of the glucose transporter, epidermal growth factor, and epidermal growth factor receptor.2728 Second, excessive SB is known to induce chronic systemic inflammation with an increase in circulating inflammatory markers.29 It is well known that chronic inflammation promotes genetic mutations and tumor development through continuous tissue damage and regeneration. Moreover, numerous chemokines and cytokines from activated inflammatory cells may lead to tumor growth, migration, and differentiation by releasing growth factors, stimulating DNA damage.30 In this context, PA may lower systemic inflammation and cancer risk by releasing anti-inflammatory cytokines, such as interleukin (IL)-6 and IL-10, by reducing the circulating number of pro-inflammatory monocytes.31 In addition, energy expenditure from PA affects the metabolism of tumor cells, thereby hindering their growth and progression.32
Unlike the recently proposed hypothesis “PA health paradox,” this study suggests that a higher level of any type of PA, including even OPA, can be helpful in reducing the risk of CRC with reduced SB. OPA has shown inconsistent effects on health. It has been linked to an increased mortality,33 and poor subjective health34 but high OPA levels have also been associated with general health benefits.35 Meanwhile, LTPA has been shown to have a consistent protective effect on health and is inversely related to all-cause mortality.36 Although there are few studies on CRC risk and types of PA, a recent study found that both OPA and LTPA were associated with a lower risk of CRC.37
This study has several limitations. First, the cross-sectional design could not be used to determine the causal relationships. Therefore, the findings remain purely hypothesis generating. Further studies are required to verify the hypothesis on the joint effects of SB and different types of PA on CRC risk. Second, the main variables in this study were investigated using self-reported questionnaires in the KNHANES, which may have resulted in reporting bias. Third, although some research has indicated that the relationship between CRC and SB can differ depending on the anatomical sites of CRC,38 the KNHANES did not provide such information and therefore this factor could not be analyzed. Similarly, information on dietary habits, such as vegetable or fruit intake and frequency of eating out, was not consistently collected, and could not be included in the analysis. Future research should include these potential risk factors for CRC.
Despite these limitations, this study found a significant association between SB and CRC risk and the combined effect of SB and different types of PA on CRC risk. The strengths of this study are that it is based on validated and widely employed questionnaires on PA and SB, and the large sample size and its random homogenous characteristics permit reliable generalization.
In conclusion, this study shows that SB is significantly associated with an increased risk of CRC. The results also suggest that those who engaged in SB without PA were at higher risk of CRC. Reducing sitting time as well as increasing PA in any environment can be recommended to help reduce the risk of CRC.
 XML Download
XML Download