

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) is one of the deadliest and most widespread viral infections in human history. Currently, there are approximately 200 million confirmed cases and five million deaths worldwide.1 COVID-19 is caused by an enveloped positive-stranded RNA virus that includes beta-coronavirus with the same subgenus but a different strain as severe acute respiratory syndrome coronavirus, which caused a pandemic in 2003.2
As a result of increased globalisation, infectious diseases can be transmitted much more efficiently.3 Owing to the highly contagious nature of COVID-19, vaccination is important to achieve herd immunity and prevent disease outbreaks. BNT162b2 and mRNA-1273 are representative mRNA vaccines, and their safety has been proven through several clinical trials worldwide. Research on the efficacy and safety of vaccines is still in progress.4567 The short-term adverse effects of the vaccine are not significantly different from those of other vaccines, and long-term adverse effects are not yet known. Moreover, in patients with rare adverse effects, it is difficult to evaluate the causal relationship with the vaccine.
There had been several case reports of anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) occurring after vaccination.89101112 Recently, several cases of AAV were reported worldwide after receiving the COVID-19 mRNA vaccine.1314151617 Here, we report the first case of MPA following the second dose of BNT162b2 vaccine in Korea.
CASE DESCRIPTION
A 42-year-old man visited the emergency department because of general weakness, shortness of breath, edema, gross hematuria, and significant weight loss (5 kg) that had developed approximately 2–3 weeks earlier. The symptoms occurred after receiving a second dose of BNT162b2 vaccine on October 5, 2021, 63 days after the first dose. He had not taken any medication earlier except tuberculosis medication between August 2020 and March 2021. In addition, there were no specific findings in the family history and psychosocial history. On physical examination, the initial vital signs were stable, and mild pitting edema was seen in both legs. Any other signs, such as arthralgia, redness, sensation of heat on the skin, and skin rash were not observed. Routine laboratory assessments obtained 201 days prior to receiving a second dose vaccine were normal for serum creatinine (sCr) of 0.97 mg/dL (reference range: 0.5–0.10) and estimated glomerular filtration rate (eGFR) of 96.6 mL/min/1.73 m2 (reference range: 60–180) (Table 1). The serum levels of acute phase reactants were normal for white blood cell (WBC) was 7,700 /mm3 and C-reactive protein was 0.7 mg/dL.
Table 1
Laboratory results

| Variables | Days relative to second vaccine dose | Reference range | |||
|---|---|---|---|---|---|
| −201 | +21 | +41 | +56 | ||
| BUN, mg/dL | 19 | 59 | 52 | 51 | 8.0–21 |
| sCr, mg/dL | 0.97 | 3.05 | 2.41 | 1.51 | 0.5–1.0 |
| eGFR, mL/min/1.73 m2 | 96.6 | 24.0 | 31.9 | 56.2 | 60–180 |
Acute kidney injury (AKI) at admission was observed with sCr levels of 3.05 mg/dL, blood urea nitrogen (BUN) of 59 mg/dL (reference range: 8.0–21) and an eGFR of 24.0 mL/min/1.73 m2 (Table 1). Dipstick urine test showed proteinuria (3+), hematuria (many red blood cells under high-power field [HPF], and epithelial cells [0–4 under HPF]) but was negative for glucose, WBCs, bacteria, and hyaline casts. The random urinary protein-creatinine ratio (UPCR) was 3,438 mg/g*Cr.
The following tests were found to be within the normal range: Complement component 3: 88.95 mg/dL (reference range: 90–180), Complement component 4: 39.97 mg/dL (reference range: 10–40), immunoglobulin (Ig) A 189.40 mg/dL (reference range: 70–400), IgM 100.91 mg/dL (reference range: 40–230), IgG 973.92 mg/dL (reference range: 700–1,600), rheumatoid factor 8.23 IU/mL (reference range: 0–14), antistreptolysin O 91.1 IU/mL (reference range: 0–200), rapid plasma reagin 0.3 RU (reference range: 0.1–1.0). Negative findings were confirmed in the following tests: test for hepatitis B, hepatitis C, human immunodeficiency virus, cryoglobulinaemia, antinuclear antibodies, anti-glomerular basement membrane antibodies, anti-double stranded DNA antibodies, anti-phospholipase A2 receptor antibodies, and lupus anticoagulant test.
Anti-proteinase-3 antibodies were not determined, whereas MPO antibodies were elevated at 38.6 IU/mL (reference range: < 3.5). A renal biopsy was performed 29 days after the second vaccination. On histological examination, 21 glomeruli were identified, among which nine cellular crescents and two fibrous crescents were identified. Diffuse necrotising and crescentic glomerulonephritis with mild interstitial inflammation was confirmed using a light microscope (Fig. 1). In addition, a paucity of immune deposits was confirmed by immunofluorescence microscopy. According to histological findings, pauci-immune ANCA-related glomerulonephritis was confirmed, and finally, MPA was diagnosed.
Fig. 1
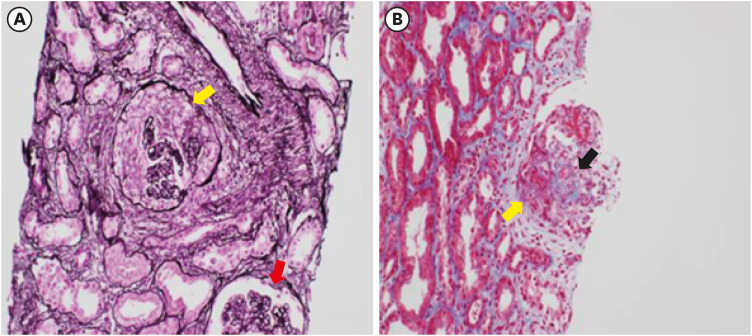
Light microscopic findings. (A) A glomerulus shows a global cellular crescent (yellow arrow) and normal glomeruli without crescents (red arrow) (Periodic acid-silver methenamine and Masson stain, ×100) (B) Another glomerulus shows a segmental cellular crescent (yellow arrow) with fibrinoid necrosis characterized by fibrin extravasation (black arrow) (Masson’s trichrome stain, ×100)
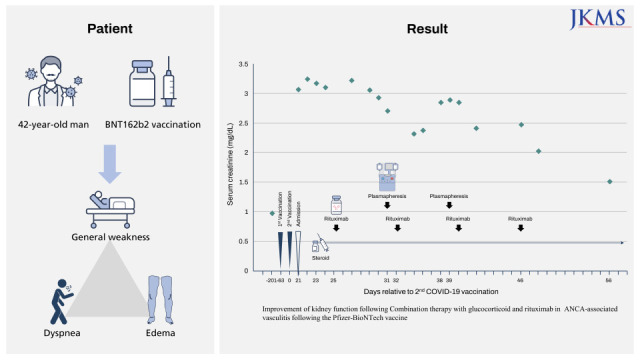
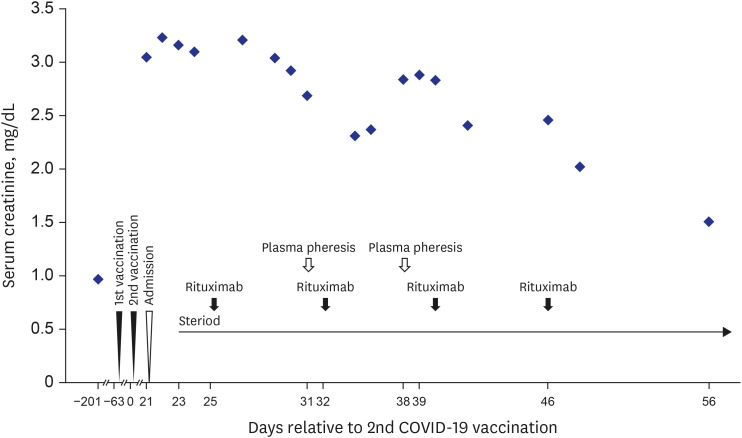
Combination therapy with glucocorticoid and rituximab was administered as induction therapy, and plasma exchange was additionally performed. Methylprednisolone (500 mg) was administered intravenously for three days, and thereafter, oral prednisolone (1 mg/kg) was administered. A bolus of 622 mg of rituximab was administered intravenously for 4 weeks (375 mg/m2 every week). Plasma exchange was performed twice because of the patient’s reluctance. He was discharged on November 16, 2021, 19 days after induction therapy. On November 30, 2021, the patient visited the outpatient clinic, 33 days after induction therapy. He said that general weakness still remained mild, but other symptoms were improved. Actually, kidney function was partially restored (Table 1 and Fig. 2). Nephrotic-range proteinuria (random UPCR, 4,203 mg/g*Cr) was still observed, but anti-MPO antibodies decreased to 19.6 IU/mL. There were no side effects. The current treatment was effective, and no side effects were found, so we decided to follow up with him as an outpatient and reduce the steroid dose.
DISCUSSION
We reported that MPA occurred in a healthy man after the administration of the BNT162b2 vaccine in Korea, firstly. It is accepted that the COVID-19 mRNA vaccine is safe and effective, although the COVID-19 vaccine has been used only for approximately 2 years. However, serious adverse events are rarely reported as vaccination rates increase. Several cases of MPA after COVID-19 mRNA vaccine administration have been reported, and MPA occurred after the second dose of vaccine.13141516 Hematuria and proteinuria, which are representative of kidney involvement, were also observed. Except for one patient with normal kidney function at diagnosis of MPA,16 three patients with AKI recovered kidney function after immunosuppressive treatment.131415 Similar to previous reports, MPA in our case occurred after the second dose of vaccine and is currently improving with rituximab and steroid treatment.
In influenza immunization, which is an mRNA vaccine like BNT162b2 vaccine, there have been several cases of AAV following vaccination, and a causal relationship and its mechanism have been studied.891011 It is hypothesised that the molecular similarity between vaccine components and antigens on the surface of human neutrophils after vaccination induces the production of pathogenic ANCA or hypersensitivity of the vaccine to viral RNA induces the production of ANCA.918 AAV may have occurred after COVID-19 mRNA vaccination by a mechanism similar to AAV following other vaccinations. Enhanced immune response after the second vaccination could promote pathogenic ANCA, eventually leading to AAV. However, the exact mechanism by which COVID-19 mRNA vaccines induce AAV other than through temporal causality has not yet been elucidated. MPA could be also a random event unrelated to vaccination. Additional causality studies are required to establish safer vaccination policies.
In AAV, the patient mortality rate was 19–50% at 5 years, and kidney survival rates at 5 years were 70–80%, depending on the severity of kidney involvement at diagnosis.192021 In a comparative study, early treatment in the absence of advanced nephrosclerosis produced a positive effect in 70–80% of patients with ANCA-associated rapid progressive glomerulonephritis.22 Crescent glomerulonephritis was confirmed in five patients with AAV following COVID-19 mRNA vaccination in previous studies, including our report. In all patients, renal function was restored. Although few cases have been reported, the prognosis for vaccine-associated AAV may be better than that for AAV caused by other causes.
Because of several case reports of AAV onset following COVID-19 vaccination, we may have reasonable suspicion and bring forward the diagnosis and treatment of rare AAV following COVID-19 vaccination. Currently, COVID-19 vaccines are being considered for an annual booster shot, such as seasonal boosters for flu and respiratory syncytial viruses. We suggest that MPA needs to be considered if patients have acute kidney injury, proteinuria, and hematuria after vaccination.
 XML Download
XML Download