

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Breast cancer is a common malignancy with a high mortality rate among women. Different medical imaging modalities, such as magnetic resonance imaging (MRI), ultrasound, and mammography, are largely used to evaluate primary breast lesions. Other techniques such as computed tomography (CT), F-18 Fluorodeoxyglucose positron emission tomography (F-18 FDG PET), and bone scan are used to assess distant metastatic lesions. F-18 FDG PET, which can cover the body from the skull base to the thigh in one scan, is beneficial for evaluating distant metastasis.123 Simultaneously, F-18 FDG PET has been of interest to policymakers owing to its relatively high cost. Effective December 1, 2014, the National Health Insurance Service amended the F-18 FDG PET reimbursement criteria to induce reasonable medical use. Detailed amended criteria can be found in the Supplementary Table 1.
When medical providers submit a claim to the Health Insurance Review and Assessment Service (HIRA) for reimbursement of services provided to patients, the HIRA collect data. National Health Insurance in South Korea covers approximately 98% of individuals of Korean nationality, and all medical institutions claim insurance reimbursement for their medical practice to the HIRA. The HIRA database includes patient records, such as sex, age, diagnoses, treatments, procedures, surgical history, and prescription drugs for reimbursement.4
Interrupted time series (ITS) analysis is a widely used regression-based method to compare changes before and after an interventional event. Many researchers have used this tool to assess the impact of a number of interventions on healthcare.5678 This study investigated the effect of F-18 FDG PET reimbursement criteria amendments using ITS analysis.
METHODS
Retrieval of HIRA claim data
We retrospectively analyzed the inpatient and outpatient data from HIRA between January 1, 2013 to December 31, 2018. The claim data included female patients older than18 years who were diagnosed with primary breast cancer (C50) according to the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10), including primary and secondary diagnoses and a cancer-specific deductible insurance code in Korea (V193).
Statistical analysis
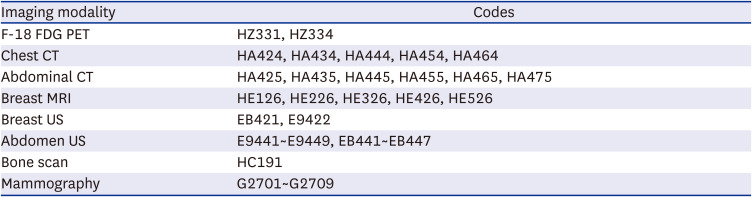
We performed ITS analysis for the number of each medical imaging modality and the total medical imaging cost of the breast cancer patients.9 The total medical imaging cost included all imaging studies after a patient is given the diagnosis code. ITS analysis evaluated the immediate and long-term effects of F-18 FDG PET reimbursement criteria amendment. Segmented linear regression model with aggregated data was used which includes segments of pre-intervention and post-intervention. The autoregressive model was applied to adjust autocorrelation error and seasonal product. The codes used in this study are summarized in Table 1. The total medical imaging cost was modified with an increase rate of medical fee which annually announced by the HIRA based on the 2018 financial year. A two-tailed test was performed for statistical significance (P < 0.05), and all analyses were performed using SAS 9.4 version (SAS Institute, Cary, NC, USA).
Table 1
Codes used for evaluation
RESULTS
Number of each medical imaging modality
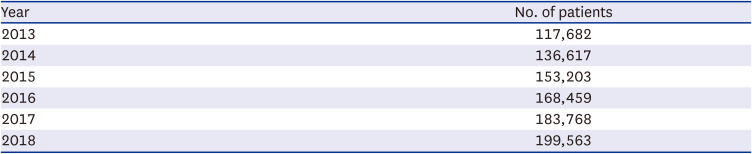
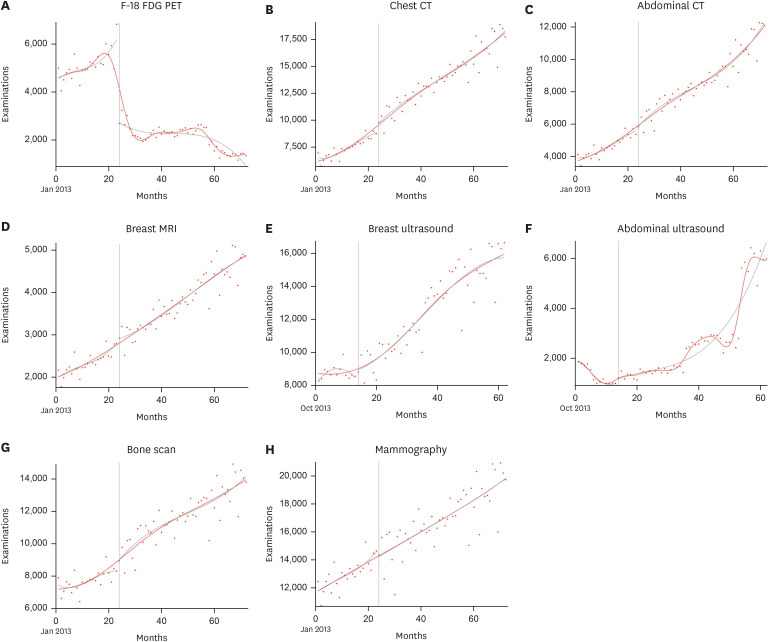
The annual numbers of breast cancer patients analyzed (Table 2) showed a steady increase from 117,682 in 2013 to 199,563 in 2018. As shown in Table 3 and Fig. 1, the number of F-18 FDG PET images showed an increasing trend before the amendment in F-18 FDG PET reimbursement criteria, which dramatically decreased immediately following the modification and continuously decreased with time. The chest and abdominal CT examinations showed an increasing trend before the amendment and some statistically significant changes immediately following the introduction of the modification. At the long-term follow-up, a statistically significant increase was observed compared with the movement before the amendment. The number of breast MRI examinations was not affected by the modification and showed a steadily increasing trend every year. The numbers of breast and abdominal ultrasound examinations did not show significant changes immediately after the amendment, but did show substantial changes at the long-term follow-up. There was no statistically significant trend in the number of bone scan examinations before the amendment. However, it showed a considerable increase immediately after the amendment and at the long-term follow-up. The mammography examinations showed an increasing trend before the amendment, but no statistically significant change was observed immediately after and at the long-term follow-up.
Table 2
Number of claimed breast cancer patients in each year
| Year | No. of patients |
|---|---|
| 2013 | 117,682 |
| 2014 | 136,617 |
| 2015 | 153,203 |
| 2016 | 168,459 |
| 2017 | 183,768 |
| 2018 | 199,563 |
Table 3
Interrupted time series analysis
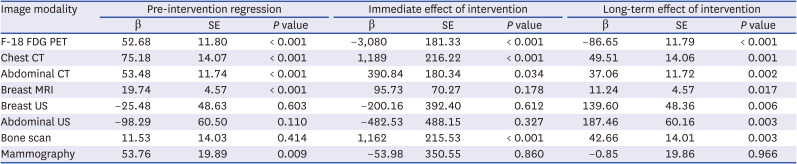
Fig. 1
Interrupted time series analysis (each medical imaging modality). (A) F-18 FDG PET. (B) Chest CT. (C) Abdominal CT. (D) Breast MRI. (E) Breast ultrasound. (F) Abdominal ultrasound. (G) Bone scan. (H) Mammography.
F-18 FDG PET = F-18 Fluorodeoxyglucose positron emission tomography, CT = computed tomography, MRI = magnetic resonance imaging.
Total medical imaging cost
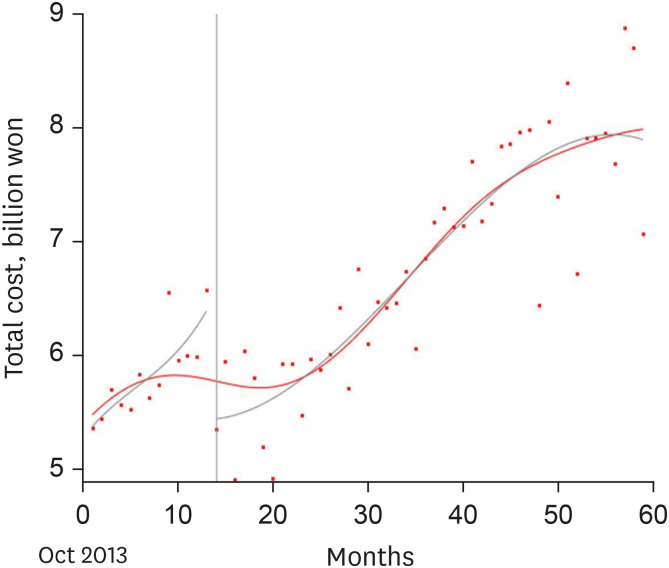
As seen in Fig. 2, the total medical imaging cost for the breast cancer patients claimed in every month showed an increasing trend before the amendment (β = 5,475, standard error [SE] = 1,992, P = 0.008) and rapid change immediately after (β = −103,317, SE = 16,152, P < 0.001). Compared with the trend before the amendment, there was no significant difference at the long-term follow-up (β = −912, SE = 1,981, P = 0.647).
DISCUSSION
This study investigated the effect of healthcare policies, such as reimbursement criteria on clinical practice. Imaging modalities for evaluating distant metastases such as F-18 FDG PET, chest CT, abdominal CT, and bone scan showed significant changes after the amendments in F-18 FDG PET reimbursement criteria. However, imaging modalities for assessing primary breast lesions, such as breast MRI, breast ultrasound, and mammography, did not change immediately after the amendment as per the ITS analysis undertaken. We need to consider another reimbursement criteria amendment for abdominal ultrasound that came into effect on April 1, 2018 in the future study.
The number of F-18 FDG PET examinations dramatically decreased after the F-18 FDG PET reimbursement criteria were amended. However, the total medical imaging cost for a breast cancer patient did not change statistically significantly at the long-term follow-up due to the increase in cost of other medical imaging modalities to evaluate the distant metastases.
Two ways to reduce health insurance expenditure for reducing expensive medical imaging examinations that can be considered are: reducing the cost by limiting the reimbursed price and the number of studies performed by restricting the reimbursement criteria. While the former can induce an increased total number of examinations performed, the latter can generate expensive alternative modalities thereby increasing the cost of medical imaging. This study shows that despite the dramatic decrease in F-18 FDG PET examination, the long-term total cost toward medical imaging for breast cancer did not significantly change due to increasing number of other studies such as CT, MRI, and bone scan.
Andersen's behavioral model is commonly used as a theoretical model for medical services. This model suggests that people use medical services according to predisposing, enabling, and need factors; healthcare policy is indicative as an enabling factor.10
Moreover, according to changes in healthcare policies, medical personnel and institutions seek changes in the form of treatment, and the difference in the use of medical services also increases. Studies on the effects of domestic healthcare policies on medical use have mainly focused on identifying the impact of strengthening insurance coverage for cancer and other serious diseases.
Studies on healthcare coverage, in particular, those based on the analysis of the increase or decrease use of medical equipment or service due to changes in health insurance policies, show variable results; and global studies have shown a similar trend.1112
The limitations of this study are as follows: First, non-reimbursed items were not included because we only analyzed claims data from the HIRA. Second, the differences between the stages of breast cancer could not be analyzed. Third, the total imaging cost included all imaging studies after a patient is given the diagnosis code. Fourth, the period following the amendment is not long enough; hence, breast cancer prognosis may have not been extensively considered. Fifth, the period before the amendment is not long enough due to the contract on the Joint Project on Quality Assessment Research through the HIRA, we were only able to acquire data after 2013.
Nevertheless, we believe that this study provides valuable data to health policymakers by demonstrating that the amendment of the F-18 FDG PET reimbursement criteria can affect the healthcare behaviors of practicing clinicians. However, till date, there is no report documenting the effect of F-18 FDG PET reimbursement criteria on healthcare behaviors. Hence, this study can be used to frame an appropriate healthcare policy related to amendments of reimbursement criteria.
 XML Download
XML Download