

 PDF
PDF Citation
Citation Print
Print



By August 2021, the cumulative number of pregnant women with coronavirus disease 2019 (COVID-19) in South Korea was 731 (< 0.3% of all cases).1 Nevertheless, few hospitals admitted late-pregnant women with COVID-19. Since the autumn of 2021, the number of COVID-19-affected pregnant women has increased, and the delay in bed assignment emerged as a social problem.
Newborns of mothers with COVID-19 are assumed to have severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection until test results are available. Isolation care requirements of newborns make hospital allocation for late-pregnant women with COVID-19 difficult. Although rooming-in is promoted in many guidelines,2345 a neonatal intensive care unit (NICU) is the only suitable environment for appropriate care of an isolated neonate in most hospitals in Korea. Therefore, Korean guidelines recommend that newborns should be immediately isolated in a negative-pressure room or a private room in the NICU if no negative-pressure rooms are available.6 Considering exposure risks in NICUs, clinicians are reluctant to place newborns with maternal COVID-19 in non-negative-pressure rooms. Given the on-going COVID-19 pandemic and limited resources, the risk of intrauterine and perinatal SARS-CoV-2 transmission and need for negative-pressure isolation rooms should be examined. This study aimed to describe clinical characteristics and hospital courses of infants born to SARS-CoV-2-positive mothers and suggest ways to resolve the shortage of isolation rooms in this context.
The management of labor and delivery of pregnant women with COVID-19 at the National Medical Center was based on the latest Korean Society of Pediatric Infectious Diseases guidelines.7 All mothers with COVID-19 delivered via cesarean section in isolation in a negative-pressure operating room. The newborn resuscitation area was 2 m away from the mother. Mothers wore masks during the delivery. After routine resuscitation (drying, stimulation, and suctioning) and additional resuscitative measures, as required, newborns were moved in a closed transport incubator to private negative-pressure rooms in the nursery and were separated from unaffected newborns. Newborn evaluation and care, SARS-CoV-2 testing, and criteria for discontinuing isolation were performed according to the latest guidelines.7 After 2 consecutive negative SARS-CoV-2 polymerase chain reaction (PCR) tests on nasopharyngeal and oropharyngeal samples at 24 hours and 48 hours after birth, newborns with maternal COVID-19 were released from quarantine and cared for with other newborns in the nursery until discharge. Infants were fed formula milk during maternal isolation.
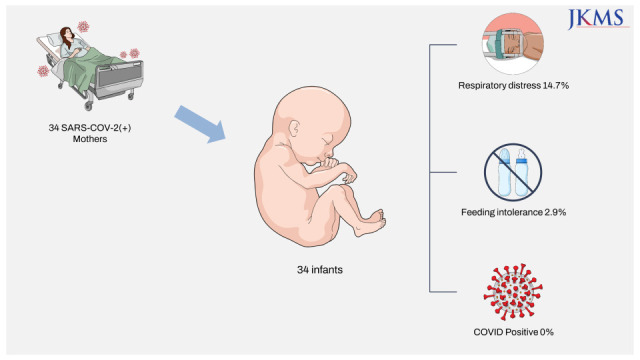
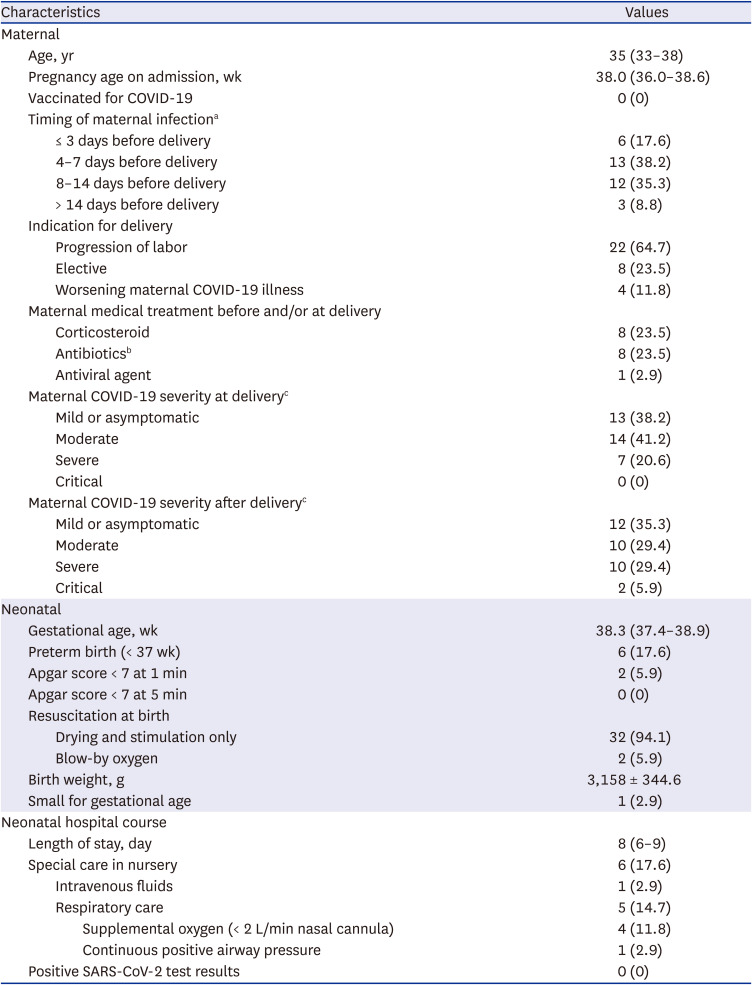
Between December 2020 and December 2021, 34 women with gestational age ≥ 35 weeks delivered 34 newborns during their isolation period. According to the U.S. National Institutes of Health COVID-19 Treatment Guidelines criteria,8 7 (20.6%) cases had severe COVID-19 before delivery and 5 (14.7%) cases progressed to severe illness after delivery. A total of 15 (44.1%) postpartum women had severe or critical COVID-19 or body temperature ≥ 38.0°C. Mother and newborn characteristics are presented in Table 1.
The median gestational age at birth was 38.3 weeks. Six (17.6%) infants were born preterm. No infants required advanced resuscitation such as chest compressions, positive-pressure ventilation, or medication at birth. During the hospital stay, 6 (17.6%) infants required specialized care. One infant with feeding intolerance required intravenous fluid therapy. Five infants had respiratory distress and required respiratory support: 4 with supplemental oxygen via a nasal cannula and 1 with nasal continuous positive airway pressure. The final diagnoses were transient tachypnea of the newborn (n = 3), delayed transition (n = 1), and meconium aspiration syndrome (n = 1). The infants with respiratory distress improved shortly and were weaned to room air within 48 hours of age. Overall, 17 (50.0%) mother–infant dyads (mothers with mild or moderate illness and without fever and infants not requiring specialized care) remained well during the entire hospitalization.
The SARS-CoV-2 PCR test results of all 34 newborns were negative at 24 hours and 48 hours after birth. After release from a median of 3 days (interquartile range, 2–3 days) of quarantine, the newborns were cared for in the nursery with non-COVID-19-exposed newborns. The 23 (67.6%) newborns stayed in the nursery until their mother was discharged. On follow-up phone calls made by nurses within 7 days after discharge, all infants remained in good condition and there were no additional confirmed cases of COVID-19 among them.
Previous reports on newborns of mothers with COVID-19 in Korea reported about 4 infants born at full term via cesarean section and immediately separated from their mothers.91011 No infant tested positive for SARS-CoV-2. Our findings are consistent with those of previous case studies managed using a similar policy. Worldwide, the mother-to-infant transmission rate of SARS-CoV-2 is reported to be in the range of 7–13%1213 based on studies published before the implementation of the current guidelines, potentially overestimating the true incidence. In contrast, U.S. studies with larger sample sizes reported virtually no mother-to-infant transmission of SARS-CoV-2, despite high rates of rooming-in and direct breastfeeding.14151617
An infant born to a mother with COVID-19 and requiring neonatal intensive care and respiratory support should be admitted to a private room with the potential for negative room pressure or to one with a door.218 For an infant with mild respiratory distress, which does not require positive pressure ventilation, a private room may be an adequate preventive strategy.18 Under a more stringent policy, stable newborns with respiratory support of up to 2 L/min of oxygen via a nasal cannula can be placed in neutral pressure rooms with precautions.19 According to these criteria, only 1 (2.9%) infant in our study required a negative-pressure isolation room. Approximately 12–15% of infants of mothers with COVID-19 were admitted to the NICU in previous studies including early preterm infants.151620 The proportion of infants requiring aerosol generating procedures (AGPs) is estimated to be in the range of < 12–15% and even lower for late-preterm and full-term infants. Because intrauterine infection of SARS-CoV-2 is rare, and the risk of postnatal transmission is low while rooming-in with appropriate precautions,17 the risk of airborne SARS-CoV-2 transmission in newborns, independently of being separated from the mother immediately after birth, is likely very low. If negative-pressure isolation rooms are selectively used for newborns requiring AGPs, resource availability for lower-risk cases may improve.
Half of the mother–infant dyads in our study remained well during their hospital stay. Rooming-in, if practiced, might have helped relieve the burden of hospital overcrowding because it requires a single patient room for the mother and infant. Mother-to-infant transmission of SARS-CoV-2 during rooming-in is rare, provided that adequate droplet and contact precautions are taken. In studies evaluating rooming-in for infants born to SARS-CoV-2-positive mothers, most mother–infant dyads safely roomed-in.141517
,
212223 Separating mothers and newborns may not be warranted to prevent SARS-CoV-2 transmission. Based on accumulating evidence and given the benefits of breastfeeding and mother–infant contact, many guidelines recommend rooming-in unless precluded by the mother or newborn condition.2345 In general, mothers are eligible for rooming-in under the following conditions: no need for respiratory support or supplemental oxygen, body temperature < 38°C, stable vital signs, and ability to take care of the baby. Newborns are eligible for rooming-in when they are well-appearing, with a gestational age ≥ 35 weeks and birth weight ≥ 2,000 g, physical examination findings within normal limits, vital signs within the reference ranges, and skilled in feeding.1523 Temporary separation of the newborn from the mother during hospital stay may be inevitable for either maternal or neonatal reasons. When rooming-in is interrupted, the newborn may be isolated in a private room unless AGPs are required.
Our study had some limitations. First, this was a single-center study. Our results should be interpreted with caution because they may have been influenced by the strict policy implemented at our institution. Second, this study did not include cases requiring neonatal intensive care for maternal or fetal indications, thus limiting the generalizability of the results to pregnant women with initially severe COVID-19 illness, with a gestation age of 21–34 weeks and early preterm infants, or with a high-risk fetus. Despite these limitations, this study presented data on the largest number of SARS-CoV-2-positive mother–newborn dyads in Korea to date. Furthermore, our study suggests that most infants with gestational age ≥ 35 weeks can be safely isolated in a private room and are clinically well enough to room-in with their mother. A negative-pressure room can be spared for infants requiring AGPs. The change in isolation policy may help resolve the shortage of newborn isolation rooms and ensure safe delivery by mothers during the COVID-19 pandemic. Further multicenter studies with larger patient cohorts are required to elucidate the characteristics and outcomes of SARS-CoV-2-positive women and their newborns in South Korea.
 XML Download
XML Download