

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Bronchopulmonary dysplasia (BPD) is characterized by prolonged oxygen dependency or ventilator support of preterm infants.12 Various perinatal factors may affect BPD development, including lung damage and impaired alveolar and vascular development.123 Efforts have been made to predict the occurrence of BPD soon after birth4 and to prevent BPD in preterm infants using various ventilator strategies5 and the early caffeine use.6 However, the incidence of BPD has not decreased over the past 10 years in infants born at less than 30 weeks of gestation in Korea.7 Apart from postnatal care, prenatal management is important to prevent BPD. Hypertension during pregnancy (HDP) has been reported as a risk factor for BPD.89101112 HDP (including pre-eclampsia) causes various prenatal morbidities, including preterm birth, intra-uterine growth restriction, and maternal complications.1314 The placental pathology of HDP is characterized by placental insufficiency, decreased fetal perfusion, and intrauterine growth restriction; these are also risk factors for BPD.1516 We performed this meta-analysis to examine the association between maternal HDP and neonatal BPD in the preterm infants.
METHODS
Search strategy and study selection
We searched PubMed, EMBASE, the Cochrane Library, and the KoreaMed database for relevant studies. We used the following search terms: infant, premature, neonate, pregnancy-induced hypertension, pre-eclampsia, eclampsia, hypertension, BPD, and/or chronic lung disease. The last search was performed on June 18, 2019. The titles and abstracts of all articles were initially screened, and the full-text articles were then reviewed by two authors (Park HW and Lim G) using predefined selection criteria. We excluded case reports, case series, review articles, editorials, and comments. The reference lists of included studies were manually searched, as were other electronic databases. No language restriction was imposed; studies were translated if necessary.
Inclusion and exclusion criteria
We included randomized controlled trials, observational studies (cohort studies or case-control studies), and cross-sectional studies in the analysis. Single-arm cohort studies without comparison groups, case reports, case series and animal studies were excluded. Types of HDP included gestational hypertension, pre-eclampsia-eclampsia and pre-eclampsia superimposed on chronic hypertension (based on a report from the National High Blood Pressure Education Program Working Group14). The definition of elevated blood pressure (BP) varied among the studies, including systolic BP (sBP) ≥ 140 mmHg and/or diastolic BP (dBP) ≥ 90 mmHg,816171819202122232425262728293031323334353637 an increase in sBP ≥ 25 mmHg and/or dBP ≥ 15 mmHg29 and sBP ≥ 145 mmHg and/or dBP ≥ 95 mmHg3839 after week 20 of gestation. Pre-eclampsia was defined as sBP ≥ 160 mmHg and/or dBP ≥ 110 mmHg with proteinuria, an increased creatinine level, a decreased platelet count, elevated hepatic enzyme levels, cerebral or visual symptoms (including headache), or persistent epigastric pain.1440 The combination of hemolysis, elevated liver enzyme levels, and low platelet count was considered to indicate hemolysis, elevated liver enzymes, and a low platelet count (HELLP) syndrome. Eclampsia was defined as a combination of seizures and pre-eclampsia.14 Pre-eclampsia superimposed on chronic hypertension was defined as pre-eclampsia in women exhibiting chronic hypertension prior to pregnancy.14 The definition of BPD varied among studies; some16202224253137 used the National Institutes of Health consensus,41 while others defined BPD as either oxygen dependency 28 days postnatally184243 or at 36 weeks of postmenstrual age.81218212327282930323334353638394244454647
Data extraction and study quality assessment
Park HW and Lim G independently extracted data via full-text review of selected studies. We recorded first author names, year of publication, country of origin, study design, period, and population; definitions of HDP and BPD, sample size, and BPD rates in the HDP and non-HDP groups. We assessed study quality using the Newcastle-Ottawa Scale,48 which has three domains: selection (four items), comparability (one item), and outcomes (three items). All eight items are awarded one point, except comparability (two points). Total scores range from 0 to 9: 0–3 points reflect low quality, 4–5 points moderate quality, and ≥ 6 points high quality. Any discrepancy in quality scoring or data interpretation was resolved via discussion with a third reviewer (Park YM).
Data synthesis and statistical analysis
We meta-analyzed the relationship between maternal HPD and BPD using Comprehensive Meta-Analysis software (version 3.3; Biostat Inc., Englewood, NJ, USA). We used a random-effects model if heterogeneity was present and a fixed-effects model if heterogeneity was absent. We used the I2 statistic to evaluate statistical heterogeneity among studies. If I2 > 50%, significant between-study heterogeneity is present. We performed sensitivity analysis by removing each study individually from the analysis, and performed cumulative analyses to detect changes over time. We performed subgroup analyses according to the definition of pre-eclampsia. Funnel plot symmetry was assessed, and the Begg and Mazumdar rank correlation test and Egger regression test were performed to assess publication bias. We defined publication bias as funnel plot asymmetry or a P value < 0.05 in either the Begg and Mazumdar rank correlation test or Egger regression test. We also followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis checklist of 2009 (Supplementary Table 1).
RESULTS
Literature search and selection
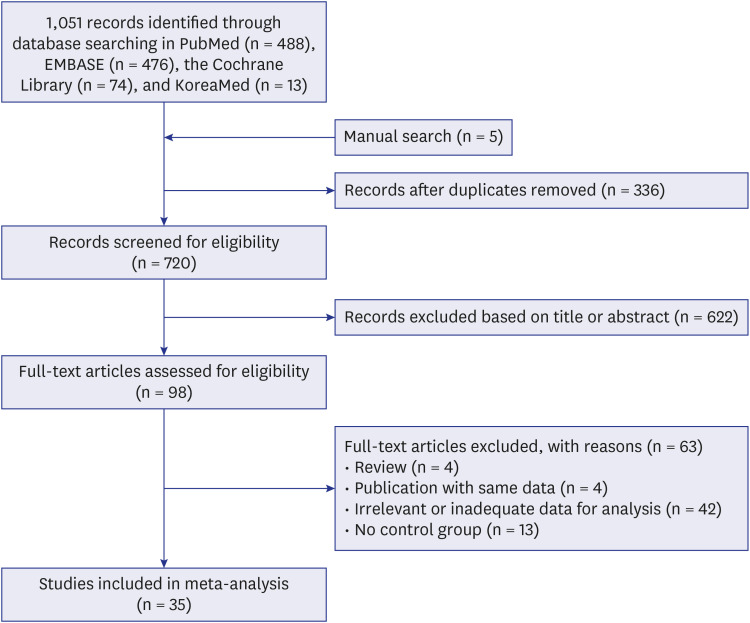
A flowchart of the study inclusion/exclusion process is shown in Fig. 1. Of 1,056 studies obtained via database and manual searching, 336 duplicates were removed. Of the remaining 720 studies, 622 were excluded based on title or abstract review, and a further 63 during full text review. We finally included 35 studies.
Characteristics of the included studies
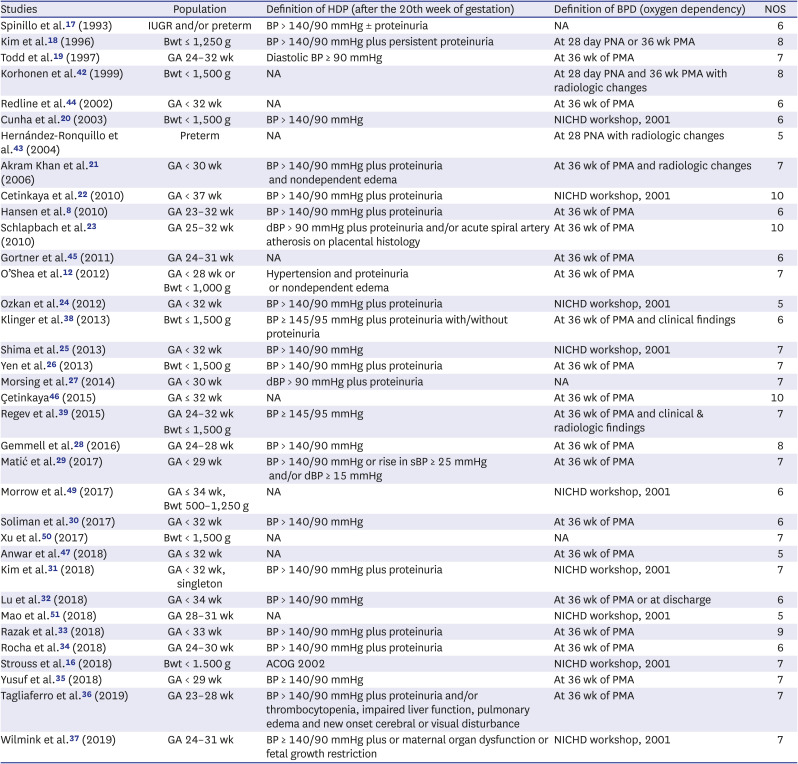
The characteristics of the included studies are shown in Table 1.812161718192021222324252627282930313233343536373839424344454647495051 A total of 97,399 infants were included in the meta-analysis. Based on a BPD definition of oxygen requirement at 36 weeks of gestation, the incidence of BPD was 32.0% (3,768 of 12,445 cases) in the HDP group and 29.1% (18,101 of 62,152 cases) in the non-HDP group. Based on a BPD definition of oxygen requirement at 28 days of age, the incidence of BPD was 27.6% (205 of 640 cases) in the HDP group and 25.5% (444 of 1,743 cases) in the non-HDP group. The incidence of severe BPD was 25.4% (91 of 358 cases) in the HDP group and 14.3% (144 of 1,007 cases) in the non-HDP group. The incidence of undefined BPD was 9.0% (16 of 177 cases) in the HDP group and 25.8% (64 of 248 cases) in the non-HDP group.
Table 1
Characteristics of studies included in this meta-analysis
| Studies | Population | Definition of HDP (after the 20th week of gestation) | Definition of BPD (oxygen dependency) | NOS |
|---|---|---|---|---|
| Spinillo et al.17 (1993) | IUGR and/or preterm | BP > 140/90 mmHg ± proteinuria | NA | 6 |
| Kim et al.18 (1996) | Bwt ≤ 1,250 g | BP > 140/90 mmHg plus persistent proteinuria | At 28 day PNA or 36 wk PMA | 8 |
| Todd et al.19 (1997) | GA 24–32 wk | Diastolic BP ≥ 90 mmHg | At 36 wk of PMA | 7 |
| Korhonen et al.42 (1999) | Bwt < 1,500 g | NA | At 28 day PNA and 36 wk PMA with radiologic changes | 8 |
| Redline et al.44 (2002) | GA < 32 wk | NA | At 36 wk of PMA | 6 |
| Cunha et al.20 (2003) | Bwt < 1,500 g | BP > 140/90 mmHg | NICHD workshop, 2001 | 6 |
| Hernández-Ronquillo et al.43 (2004) | Preterm | NA | At 28 PNA with radiologic changes | 5 |
| Akram Khan et al.21 (2006) | GA < 30 wk | BP > 140/90 mmHg plus proteinuria and nondependent edema | At 36 wk of PMA and radiologic changes | 7 |
| Cetinkaya et al.22 (2010) | GA < 37 wk | BP > 140/90 mmHg plus proteinuria | NICHD workshop, 2001 | 10 |
| Hansen et al.8 (2010) | GA 23–32 wk | BP > 140/90 mmHg plus proteinuria | At 36 wk of PMA | 6 |
| Schlapbach et al.23 (2010) | GA 25–32 wk | dBP > 90 mmHg plus proteinuria and/or acute spiral artery atherosis on placental histology | At 36 wk of PMA | 10 |
| Gortner et al.45 (2011) | GA 24–31 wk | NA | At 36 wk of PMA | 6 |
| O’Shea et al.12 (2012) | GA < 28 wk or Bwt < 1,000 g | Hypertension and proteinuria or nondependent edema | At 36 wk of PMA | 7 |
| Ozkan et al.24 (2012) | GA < 32 wk | BP > 140/90 mmHg plus proteinuria | NICHD workshop, 2001 | 5 |
| Klinger et al.38 (2013) | Bwt ≤ 1,500 g | BP ≥ 145/95 mmHg plus proteinuria with/without proteinuria | At 36 wk of PMA and clinical findings | 6 |
| Shima et al.25 (2013) | GA < 32 wk | BP > 140/90 mmHg | NICHD workshop, 2001 | 7 |
| Yen et al.26 (2013) | Bwt < 1,500 g | BP > 140/90 mmHg plus proteinuria | At 36 wk of PMA | 7 |
| Morsing et al.27 (2014) | GA < 30 wk | dBP > 90 mmHg plus proteinuria | NA | 7 |
| Çetinkaya46 (2015) | GA ≤ 32 wk | NA | At 36 wk of PMA | 10 |
| Regev et al.39 (2015) | GA 24–32 wk | BP ≥ 145/95 mmHg | At 36 wk of PMA and clinical & radiologic findings | 7 |
| Bwt ≤ 1,500 g | ||||
| Gemmell et al.28 (2016) | GA 24–28 wk | BP > 140/90 mmHg | At 36 wk of PMA | 8 |
| Matić et al.29 (2017) | GA < 29 wk | BP > 140/90 mmHg or rise in sBP ≥ 25 mmHg and/or dBP ≥ 15 mmHg | At 36 wk of PMA | 7 |
| Morrow et al.49 (2017) | GA ≤ 34 wk, Bwt 500–1,250 g | NA | NICHD workshop, 2001 | 6 |
| Soliman et al.30 (2017) | GA < 32 wk | BP > 140/90 mmHg | At 36 wk of PMA | 6 |
| Xu et al.50 (2017) | Bwt < 1,500 g | NA | NA | 7 |
| Anwar et al.47 (2018) | GA ≤ 32 wk | NA | At 36 wk of PMA | 5 |
| Kim et al.31 (2018) | GA < 32 wk, singleton | BP > 140/90 mmHg plus proteinuria | NICHD workshop, 2001 | 7 |
| Lu et al.32 (2018) | GA < 34 wk | BP > 140/90 mmHg | At 36 wk of PMA or at discharge | 6 |
| Mao et al.51 (2018) | GA 28–31 wk | NA | NICHD workshop, 2001 | 5 |
| Razak et al.33 (2018) | GA < 33 wk | BP > 140/90 mmHg plus proteinuria | At 36 wk of PMA | 9 |
| Rocha et al.34 (2018) | GA 24–30 wk | BP > 140/90 mmHg plus proteinuria | At 36 wk of PMA | 6 |
| Strouss et al.16 (2018) | Bwt < 1.500 g | ACOG 2002 | NICHD workshop, 2001 | 7 |
| Yusuf et al.35 (2018) | GA < 29 wk | BP ≥ 140/90 mmHg | At 36 wk of PMA | 7 |
| Tagliaferro et al.36 (2019) | GA 23–28 wk | BP > 140/90 mmHg plus proteinuria and/or thrombocytopenia, impaired liver function, pulmonary edema and new onset cerebral or visual disturbance | At 36 wk of PMA | 7 |
| Wilmink et al.37 (2019) | GA 24–31 wk | BP ≥ 140/90 mmHg plus or maternal organ dysfunction or fetal growth restriction | NICHD workshop, 2001 | 7 |
HDP = hypertension during pregnancy, BPD = bronchopulmonary dysplasia, NOS = The Newcastle-Ottawa Scale, IUGR = intrauterine growth restriction, BP = blood pressure, NA = not available, Bwt = birth weight, PNA = postnatal age, PMA = postmenstrual age, GA = gestational age at birth, NICHD = National Institute of Child Health and Human Development, dBP = diastolic blood pressure, sBP = systolic blood pressure, ACOG = American College of Obstetricians and Gynecologist.
Results of pooled meta-analysis
Of the 35 eligible studies, 29812161819212223242526282930313233343536373839444546474950 evaluated the relationship between HDP and BPD defined as an oxygen requirement at 36 weeks of gestation, and 81820242536374243 evaluated the relationship when BPD was defined as an oxygen requirement at 28 days of postnatal age. Two studies2436 evaluated the relationship between HDP and severe BPD, and three172750 the relationship between HDP and undefined BPD. Five studies1824253637 described one or more outcomes of BPD.
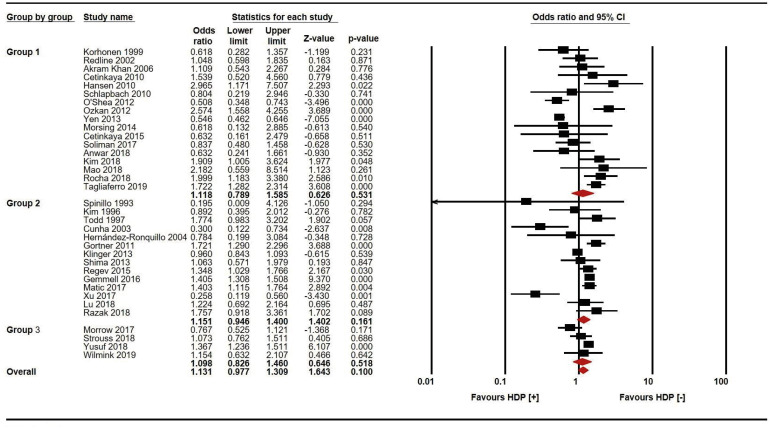
Regardless of the definition of hypertension, BPD was not associated with HDP in the overall analysis (odds ratio [OR], 1.131; 95% confidence interval [CI], 0.977–1.309; P = 0.100; Fig. 2). Subgroups were defined according to the definition of HDP: subgroup 1, pre-eclampsia and/or eclampsia and/or HELLP; subgroup 2, other HDP except chronic hypertension; subgroup 3, HDP including chronic hypertension. BPD was not associated with any HDP subgroup (Fig. 2).
Fig. 2
Meta-analysis of the relationship between maternal pre-eclampsia and neonatal bronchopulmonary dysplasia: subgroup analysis based on the definition of HDP. Subgroups were defined according to the definition of HDP: subgroup 1, pre-eclampsia and/or eclampsia and/or HELLP; subgroup 2, other HDP except chronic hypertension; subgroup 3, HDP including chronic hypertension.
HDP = hypertension during pregnancy, HELLP = hemolysis, elevated liver enzymes, and a low platelet count, CI = confidence interval.
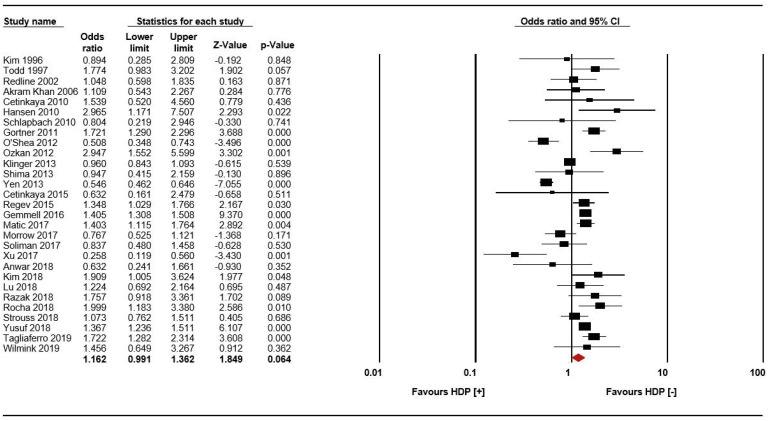
Maternal HDP was not significantly associated with BPD defined as an oxygen dependency at 36 weeks of gestation (OR, 1.162; 95% CI, 0.991–1.362; P = 0.064; Fig. 3). In the meta-analysis of the relationship between maternal HDP and BPD based on oxygen dependency at 36 weeks of gestation, significant between-study heterogeneity was evident (P < 0.001; I2 = 86.07%) so a random-effects model was used. The Begg and Mazumdar rank correlation test (P = 0.302), Egger regression test (P = 0.494) and funnel plot (Supplementary Fig. 1) showed no evidence of publication bias. The data did not change when each study was sequentially removed or added (Supplementary Fig. 2).
Fig. 3
Meta-analysis of the relationship between maternal pre-eclampsia and neonatal bronchopulmonary dysplasia defined as an oxygen requirement at 36 weeks of gestational age.
HDP = hypertension during pregnancy,, CI = confidence interval.
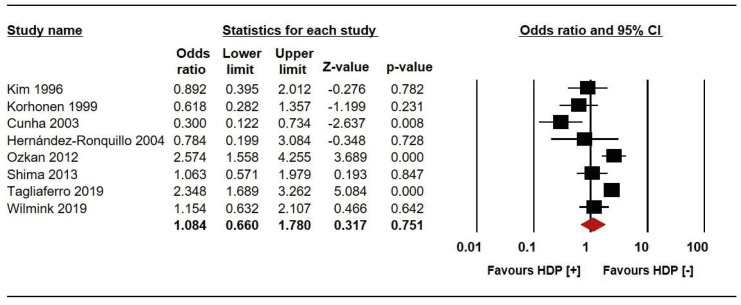
Maternal HDP was not significantly associated with BPD defined as oxygen dependency at 28 days of age (OR, 1.084; 95% CI, 0.660–1.780; P = 0.751; Fig. 4). In the meta-analysis of the relationship between maternal HDP and BPD defined as oxygen dependency at 28 days of age, significant heterogeneity was evident among the studies (P < 0.001; I2 = 78.92%) so a random-effects model was used. Both the Begg and Mazumdar rank correlation test (P = 0.035) and Egger regression test (P = 0.011) revealed evidence of publication bias. Thus, we performed trim and fill adjustments and the results did not change (OR, 1.084; 95% CI, 0.660–1.780) (Supplementary Fig. 3). No changes were seen in the sensitivity (Supplementary Fig. 4A) or cumulative (Supplementary Fig. 4B) analysis.
Fig. 4
Meta-analysis of the relationship between maternal pre-eclampsia and neonatal bronchopulmonary dysplasia defined as an oxygen requirement at 28 days of postnatal age.
HDP = hypertension during pregnancy, CI = confidence interval.
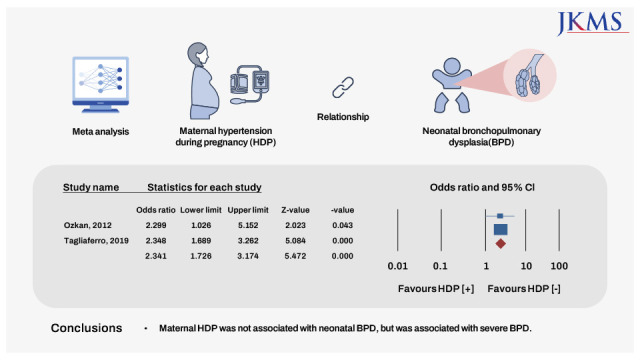
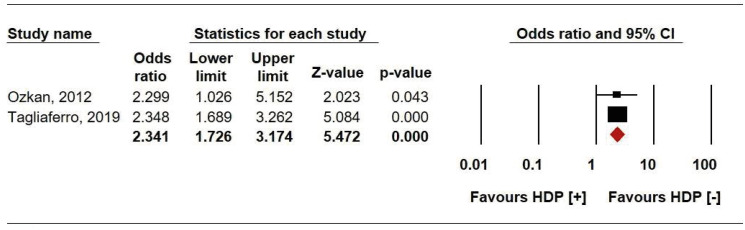
Maternal HDP was significantly associated with severe BPD (OR, 2.341; 95% CI, 1.726–3.174; P < 0.001; Fig. 5). There was no significant between-study heterogeneity (P = 0.963; I2 = 0%) so a fixed-effects model was used. Publication bias could not be evaluated because of the small number of studies. Sensitivity and cumulative analyses revealed no significant changes.
DISCUSSION
The incidence of HDP is 2–8%.91314 HDP can cause maternal and fetal complications including preterm birth, intrauterine growth restriction, and fetal death.13 Early onset (before 33 weeks of gestation) and severe disease are associated with increased risks of maternal and perinatal morbidity.1314 HDP includes gestational hypertension, pre-eclampsia/eclampsia, pre-eclampsia superimposed on chronic hypertension, and chronic hypertension.5253 Pre-eclampsia is defined by the American College of Obstetricians and Gynecologists as hypertension with proteinuria, or new-onset thrombocytopenia, renal insufficiency, impaired liver function, pulmonary edema, or cerebral or visual symptoms.53 Among the 35 studies included in this meta-analysis, 10 did not define HDP.22384243444749505154 HDP was diagnosed based on BP and proteinuria in 15 studies81216182122232426273133343637 and on the basis of BP only in 10.171920252829303539
BPD is a chronic lung disease requiring oxygen or ventilator support; many antenatal and postnatal factors, and preterm birth, affect BPD development.12 Pre-eclampsia, one of several antenatal factors, is characterized by impaired lung alveolar and vascular development.255 Changes in the levels of several anti-angiogenic and angiogenic factors have been reported in women with pre-eclampsia.815315657585960 Angiogenic factors affect fetal lung development (especially pulmonary vascular growth and alveolarization) in animal models.565961 It has been suggested that increased levels of anti-angiogenetic factors and/or inhibition of the angiogenic pathway in women with pre-eclampsia could inhibit fetal vascular or alveolar lung development56; this is the “new BPD” described by Jobe1 and Abman.62 However, the strength of the relationship between HDP and BPD varied among previous reports.8266364 The BPD risk of infants born to mothers with pre-eclampsia was elevated (unadjusted OR, 1.29; adjusted OR, 1.59) in the studies of Hansen et al.8 and Bi et al.9 (unadjusted OR, 2.96; adjusted OR, 18.7). On the contrary, HDP reduced the risk of BPD in the study of Yen et al.26 and had no association with BPD of preterm infants in other reports.122223 Although HDP overall was associated with BPD in the study of Bi et al.,9 pre-eclampsia was not and pre-eclampsia/HELLP (pooled result) was only marginally associated with BPD in the unadjusted model. We found that maternal HDP was not significantly associated with BPD defined as an oxygen dependency at either 36 weeks of gestation (OR, 1.162; 95% CI, 0.991–1.362; P = 0.064; Fig. 3) or 28 days of age (OR, 1.132; 95% CI, 0.743–1.724; P = 0.563; Fig. 4), unlike previous studies.89 Moreover, the incidence of BPD and duration of mechanical ventilation did not differ between the pre-eclampsia and non-pre-eclampsia groups in the study of Shin et al.65 It is possible that we found no association between HDP and BPD (other than severe BPD) because the clinical definitions of BPD were inconsistent. The risk of BPP in the HDP group without fetal growth restriction did not differ from that of the group without HDP, and maternal HDP was associated with BPD in cases exhibiting antenatal fetal growth restriction.10 Dravet-Gounot et al.11 explored the association between fetal growth restriction and BPD in neonates born to mothers with pre-eclampsia. Pre-eclampsia onset before 34+0 weeks of gestation (early onset), which causes fetal growth restriction, constituted only 5–20% of all pre-eclampsia cases, most of which were late-onset and thus did not cause fetal growth restriction or changes in umbilical artery blood flow.66 As early onset pre-eclampsia increases the risk of neonatal morbidity, pre-eclampsia during a critical phase of development and/or the prolonged actions of anti-angiogenetic and/or angiogenic factors may be associated with BPD.1314 We assume that continued and severe pre-eclampsia causing fetal growth restriction compromises lung development and causes BPD.
We found that maternal HDP was significantly associated only with severe BPD (OR, 2.341; 95% CI, 1.726–3.174; P < 0.001; Fig. 5). Bi et al.9 reported an association between HDP severity and BPD but the duration of ventilator support and oxygen administration are likely to vary by clinician and medical unit66; mild-to-moderate BPD does not reflect lung status. However, severe BPD always requires respiratory assistance or high concentrations of oxygen. BPD can be diagnosed without additional testing based on the physiologic definition of BPD if an infant requires over 30% oxygen or positive pressure ventilation (invasive or non-invasive).66 Severe BPD has been further subclassified based on the need for invasive mechanical ventilation (or not).67 Clinically, type 2 severe BPD is defined as a need for invasive mechanical ventilation, and is associated with poorer outcomes (including death, pulmonary hypertension, and neurodevelopmental impairment) than is type 1 BPD (defined as a need for oxygen or non-invasive mechanical support68).
Our work had certain limitations. First, data on the time of HDP onset were unavailable, and we did not evaluate the associations of changes in the levels of anti-angiogenic and angiogenic factors with HDP or neonatal BPD. It was inevitable because of limitations of a meta-analysis based on only the results of previously reported studies. Second, this meta-analysis showed an association between maternal HDP and severe BPD. However, only a small number of studies have described the BPD severity. Additional clinical studies are needed to verify the relationship between maternal HDP and severe BPD.
In conclusion, we found no association between maternal HDP and neonatal BPD, other than severe BPD. Further studies should evaluate the relationships of HDP onset and/or changes in the levels of HDP-associated anti-angiogenetic and angiogenic factors with neonatal BPD.
 XML Download
XML Download