

 PDF
PDF Citation
Citation Print
Print



Bell’s palsy is an acute idiopathic peripheral facial nerve paresis or paralysis.1234567 It is the most common type of peripheral facial palsy,23568 with an annual incidence of 11.5-53.3 per 100,000.246 Although the etiology of Bell’s palsy is unclear, reactivation of latent Herpes simplex virus type 1 (HSV-1) infection in the geniculate ganglion, ischemia, and autoimmune reaction have been suggested as causes.6
Ramsay Hunt syndrome is characterized by peripheral facial palsy and Herpes blisters in the head and neck area. Hearing loss, tinnitus, vertigo, and otalgia can accompany facial palsy in Ramsay Hunt syndrome, which is caused by reactivation of latent Varicella zoster virus.9 The annual incidence of Ramsay Hunt syndrome has been reported to be 2.2–5 per 100,000.9
In Korea, the national health care system is composed of conventional medicine and traditional Korean medicine (TKM), which are both covered by the National Health Insurance Service. Thus, patients with Bell’s palsy or Ramsay Hunt syndrome can visit medical institutions, Korean medical institutions, or both.
Considering the parallel national health care system of medicine and TKM, we investigated the distribution of medical service uses for Bell’s palsy and Ramsay Hunt syndrome between medicine and TKM using population-based data in Korea.
This retrospective study included data from the National Health Insurance Service National Sample Cohort of Korea, which is a 2% representative subsample of all National Health Insurance Service data. All people in Korea are obligated to join the National Health Insurance Service, and the results of this study are based on the whole population in Korea.
From 2006 to 2015, patients who presented to a medical or Korean medical institution outpatient clinic twice or more or those with admission once or more under the diagnostic code of Bell’s palsy (G51.0) and without that of Herpes zoster (B02) in the International Classification of Diseases (ICD) were defined as those with Bell’s palsy. Patients who fit the same criterion but for ICD codes of both Bell’s palsy (G51.0) and Herpes zoster (B02) were defined as those with Ramsay Hunt syndrome. Use of medical service was defined as treatment with at least one steroid medication under the diagnostic codes of Bell’s palsy or Ramsay Hunt syndrome. TKM service use included patients who received TKM procedures such as acupuncture, moxibustion, cupping, and meridian treatment.
Patients with Bell’s palsy or Ramsay Hunt syndrome were divided into those who used medical service only, those who used TKM service only, those who first used medical service and then TKM service, and those who first used TKM service and then medical service. The distribution of medical service use for Bell’s palsy and Ramsay Hunt syndrome was analyzed in total and according to sex, age, residence, and household income level.
The differences between medical service uses were analyzed using the χ2 test. Statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA). In all analyses, P < 0.05 was considered to indicate statistical significance.
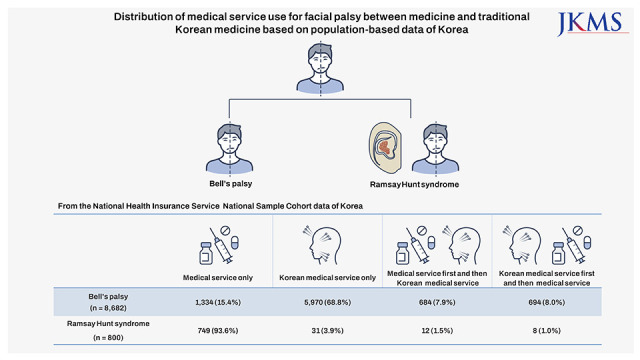
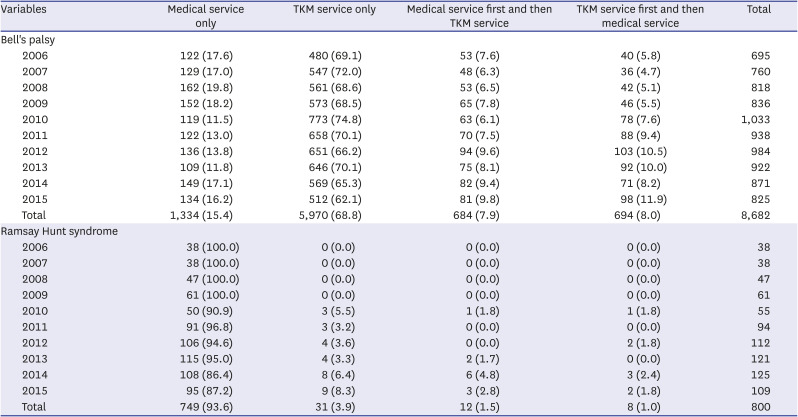
There were 8,682 patients with Bell’s palsy and 800 patients with Ramsay Hunt syndrome. For Bell’s palsy, there were 5,970 (68.8%) patients who used TKM service only, 1,334 (15.4%) patients who used medical service only, 694 (8.0%) patients who first used TKM service and then medical service, and 684 (7.9%) patients who first used medical service and then TKM service. For Ramsay Hunt syndrome, there were 749 (93.6%) patients who used medical service only, 31 (3.9%) patients who used TKM service only, 12 (1.5%) patients who first used medical service and then Korean medical service, and 8 (1.0%) patients who first used TKM service and then medical service (Table 1).
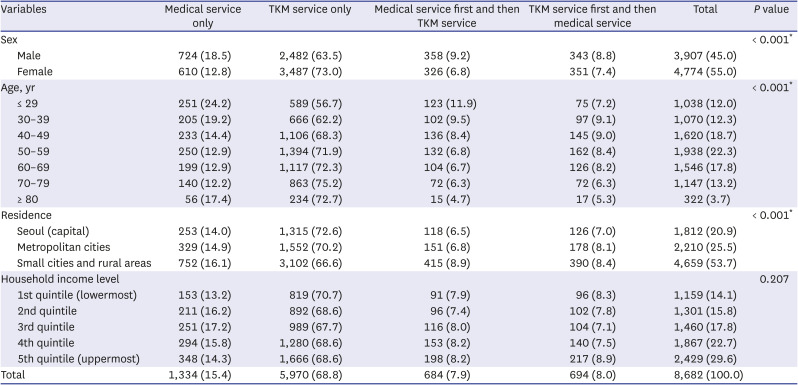
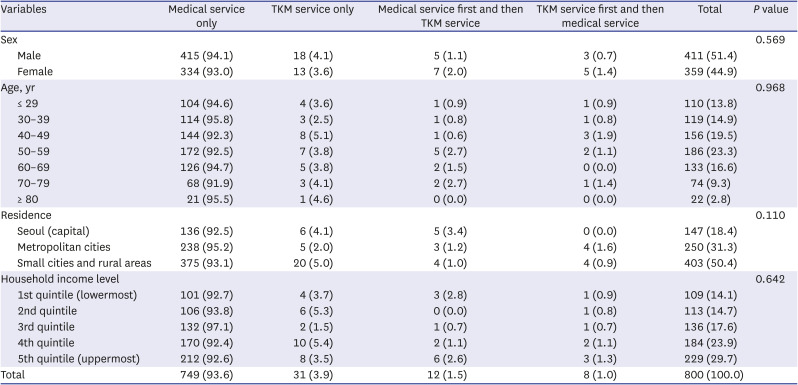
For patients with Bell’s palsy, the distribution was different significantly according to sex, with female patients more frequently using TKM service than male patients. The distribution also was different significantly according to age, revealing that older patients used TKM service more than did younger patients. The distribution was different significantly according to residence, with patients in capital and metropolitan cities more frequently using TKM service compared to those in small cities and rural areas. The distribution was not different significantly according to household income level (Table 2). For patients with Ramsay Hunt syndrome, the distribution was not different significantly according to sex, age, residence, or household income level (Table 3).
Because the national health care system is constituted of both medical and TKM services, Korean people have a choice of treatment system. Based on a nationwide survey of 21,787 patients, the proportion of TKM service uses for nerve, nerve root, and plexus disorders (G50-G59 in ICD), which included facial palsy, was 68.7%, which was the second highest of the diseases treated with TKM.10 In a study using the 2017 National Survey for the Usage of TKM, 72.0% of respondents had positive subjective perception of the effect of TKM for facial nerve paralysis.11 Park et al.12 reported that 25.4% of Korean people utilized TKM service yearly with higher proportions in the elderly and women in 2017 based on National Health Insurance Statistical Yearbook.
In Kim et al.’s study7 using the Korean Health Insurance Review and Assessment National Patient Sample data in 2016, the proportions of medical service use, TKM service use, and both medical and TKM service uses for peripheral facial palsy were 23.3%, 54.4%, and 22.3%, respectively. Female and older patients more frequently used TKM service. Similarly, the present study revealed that patients with Bell’s palsy more frequently used TKM service only, with highest use in females and older patients.
Household income level seems not to be associated with the preference for TKM service use for Bell’s palsy. Patients with Bell’s palsy who resided in capital and metropolitan cities used TKM service significantly more than those who resided in small cities and rural areas. These results might be attributed to the larger number of TKM institutions in large cities, resulting in high accessibility.
Furthermore, we investigated the distribution and order of medical service use in patients with Ramsay Hunt syndrome. In contrast to Bell’s palsy, for Ramsay Hunt syndrome, which can induce additional symptoms such as vesicular rash on the external ear, otalgia, hearing loss, or vertigo rather than facial palsy only, most patients used medical service. This might be because those with symptoms such as hearing loss or vertigo might first visit an otolaryngologic or neurologic clinic.
The strong recommended treatment for patients 16 years or older with Bell’s palsy is oral steroids within 72 hours of symptom onset based on high-quality randomized controlled trials with a preponderance of benefit over harm.28 Inflammation and edema induce facial nerve compression and can be treated with anti-inflammatory medications such as oral corticosteroids to result in recovery of facial nerve function.2 Oral antiviral medication can be added to oral steroids within 72 hours of symptom onset for patients with Bell’s palsy.28 Combined treatment of steroids and antiviral agents has been recommended for patients with Ramsay Hunt syndrome.19
Acupuncture is one of the most common procedures in Korean medicine. Among TKM service users for facial palsy, 98.3% received acupuncture based on the Korean Health Insurance Review and Assessment National Patient Sample data, also population-based.7 Acupuncture is not recommended for treatment of Bell’s palsy due to poor quality of randomized controlled trials.2 Despite a report that acupuncture had an effect on sequelae of Bell’s palsy,13 systematic reviews and meta-analyses have shown poor evidence of efficacy and safety.1358
The main treatment for Bell’s palsy and Ramsay Hunt syndrome is steroid medication. Kim et al. mentioned that approximately half of TKM service users for facial palsy did not receive steroids.7 Although approximately 70% of Bell’s palsy patients with complete paralysis and 94% of patients with incomplete paralysis recovered completely without treatment,2 both medical and TKM institutions keep in mind that steroid treatment should be recommended for patients with facial palsy at the acute phase.
There are several limitations in this study. First, the distribution of medical service use was analyzed based on diagnostic codes and medication or treatment claim codes and might not reflect the real use of medical services. However, a large number of patients was analyzed over a long time period. Second, costs, number of visits, interval of visits between medical and TKM services, and treatment outcomes according to medical service were not analyzed. In this study, we intended to verify the overall distribution of medical service use for Bell’s palsy and Ramsay Hunt syndrome. Despite these limitations, we present the distribution of medical service use for Bell’s palsy and Ramsay Hunt syndrome and the preferences of patients with facial palsy for medicine or TKM.
In conclusion, the proportion of TKM service use was higher than that of medical service use in patients with Bell’s palsy, while the opposite was found in patients with Ramsay Hunt syndrome.
 XML Download
XML Download