

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Nearly half of patients with ST-segment elevation myocardial infarction (STEMI) have multivessel disease (MVD) with significant stenoses in non-culprit vessels, and these patients showed higher risks of death or re-infarction after primary percutaneous coronary intervention (PCI). Achieving complete revascularization (CR) through multivessel PCI in these patients may not only reduce the risk of repeat revascularization but may also improve clinical outcomes by promoting recovery of myocardial perfusion. Indeed, several randomized clinical trials (RCTs) have shown the benefit of CR over culprit-only PCI in patients with STEMI1)2)3)4) and guidelines recommend multivessel PCI in STEMI patients.
Nevertheless, optimal strategy to select targets for non-culprit PCI has not been clarified. Revascularization of the non-culprit lesions can be performed based on either 1) angiographic severity assessed by diameter stenosis (DS) on visual estimation or quantitative coronary angiography, or 2) functional significance assessed by invasive physiologic indices, such as fractional flow reserve (FFR). While previous trials focused on the comparison between CR and culprit-only PCI, there exists a paucity of evidence as to which strategy is better when selecting the targets for non-culprit PCI. Although recent FLOWER-MI trial compared those 2 strategies,5) the results were inconclusive and several issues still remain. In this paper, we critically discuss and compare the safety and efficacy of different strategies for CR in patients with STEMI and MVD using a Bayesian network meta-analysis including all previous RCTs.1)2)3)4)5)6)7)8)9)10)11)12)13)14)15)16)
COMPLETE VERSUS CULPRIT-ONLY REVASCULARIZATION IN ST-SEGMENT ELEVATED MYOCARDIAL INFARCTION
Multiple RCTs have evaluated the role of CR in patients with STEMI and MVD (Table 1). In PRAMI trial, 465 patients with STEMI were randomly assigned into preventive PCI (CR) or no preventive PCI (culprit-only) groups.10) Patients assigned to the preventive PCI group underwent angiography-guided PCI of all non-culprit lesions with DS ≥50% during the index procedure. During a mean follow-up of 23 months, CR significantly reduced the primary outcome, a composite of cardiac death, nonfatal MI, or refractory angina (hazard ratio [HR], 0.35; 95% confidence interval [CI], 0.21–0.58; p<0.001).10) More recently, COMPLETE trial, by far the largest clinical trial on this topic, also showed the benefit of CR in STEMI patients.1) At a median follow-up of 3 years, the risk of composite of cardiovascular death or MI was significantly lower in the preventive PCI group compared with the culprit-only PCI group (HR, 0.74; 95% CI, 0.60–0.91; p=0.004).1) Thus, the above studies demonstrated that CR not only reduced the risk of repeat revascularization but also improved hard outcomes, supporting the importance of achieving CR in patients with STEMI and MVD.
Table 1
Characteristics of included studies
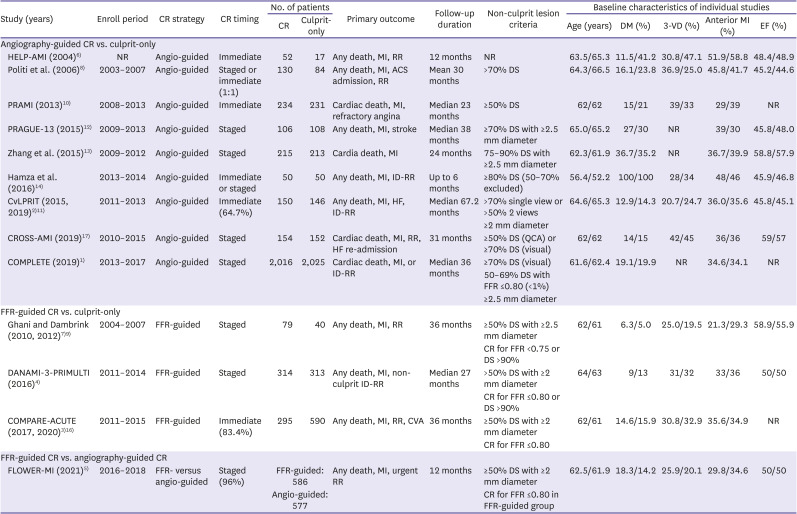
| Study (years) | Enroll period | CR strategy | CR timing | No. of patients | Primary outcome | Follow-up duration | Non-culprit lesion criteria | Baseline characteristics of individual studies | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CR | Culprit-only | Age (years) | DM (%) | 3-VD (%) | Anterior MI (%) | EF (%) | ||||||||
| Angiography-guided CR vs. culprit-only | ||||||||||||||
| HELP-AMI (2004)6) | NR | Angio-guided | Immediate | 52 | 17 | Any death, MI, RR | 12 months | NR | 63.5/65.3 | 11.5/41.2 | 30.8/47.1 | 51.9/58.8 | 48.4/48.9 | |
| Politi et al. (2006)8) | 2003–2007 | Angio-guided | Staged or immediate (1:1) | 130 | 84 | Any death, MI, ACS admission, RR | Mean 30 months | >70% DS | 64.3/66.5 | 16.1/23.8 | 36.9/25.0 | 45.8/41.7 | 45.2/44.6 | |
| PRAMI (2013)10) | 2008–2013 | Angio-guided | Immediate | 234 | 231 | Cardiac death, MI, refractory angina | Median 23 months | ≥50% DS | 62/62 | 15/21 | 39/33 | 29/39 | NR | |
| PRAGUE-13 (2015)12) | 2009–2013 | Angio-guided | Staged | 106 | 108 | Any death, MI, stroke | Median 38 months | ≥70% DS with ≥2.5 mm diameter | 65.0/65.2 | 27/30 | NR | 39/30 | 45.8/48.0 | |
| Zhang et al. (2015)13) | 2009–2012 | Angio-guided | Staged | 215 | 213 | Cardia death, MI | 24 months | 75–90% DS with ≥2.5 mm diameter | 62.3/61.9 | 36.7/35.2 | NR | 36.7/39.9 | 58.8/57.9 | |
| Hamza et al. (2016)14) | 2013–2014 | Angio-guided | Immediate or staged | 50 | 50 | Any death, MI, ID-RR | Up to 6 months | ≥80% DS (50–70% excluded) | 56.4/52.2 | 100/100 | 28/34 | 48/46 | 45.9/46.8 | |
| CvLPRIT (2015, 2019)2)11) | 2011–2013 | Angio-guided | Immediate (64.7%) | 150 | 146 | Any death, MI, HF, ID-RR | Median 67.2 months | >70% single view or >50% 2 views | 64.6/65.3 | 12.9/14.3 | 20.7/24.7 | 36.0/35.6 | 45.8/45.1 | |
| ≥2 mm diameter | ||||||||||||||
| CROSS-AMI (2019)17) | 2010–2015 | Angio-guided | Staged | 154 | 152 | Cardiac death, MI, RR, HF re-admission | 31 months | ≥50% DS (QCA) or ≥70% DS (visual) | 62/62 | 14/15 | 42/45 | 36/36 | 59/57 | |
| COMPLETE (2019)1) | 2013–2017 | Angio-guided | Staged | 2,016 | 2,025 | Cardiac death, MI, or ID-RR | Median 36 months | ≥70% DS (visual) | 61.6/62.4 | 19.1/19.9 | NR | 34.6/34.1 | NR | |
| 50–69% DS with FFR ≤0.80 (<1%) | ||||||||||||||
| ≥2.5 mm diameter | ||||||||||||||
| FFR-guided CR vs. culprit-only | ||||||||||||||
| Ghani and Dambrink (2010, 2012)7)9) | 2004–2007 | FFR-guided | Staged | 79 | 40 | Any death, MI, RR | 36 months | ≥50% DS with ≥2.5 mm diameter | 62/61 | 6.3/5.0 | 25.0/19.5 | 21.3/29.3 | 58.9/55.9 | |
| CR for FFR <0.75 or DS >90% | ||||||||||||||
| DANAMI-3-PRIMULTI (2016)4) | 2011–2014 | FFR-guided | Staged | 314 | 313 | Any death, MI, non-culprit ID-RR | Median 27 months | >50% DS with ≥2 mm diameter | 64/63 | 9/13 | 31/32 | 33/36 | 50/50 | |
| CR for FFR ≤0.80 or DS >90% | ||||||||||||||
| COMPARE-ACUTE (2017, 2020)3)16) | 2011–2015 | FFR-guided | Immediate (83.4%) | 295 | 590 | Any death, MI, RR, CVA | 36 months | ≥50% DS with ≥2 mm diameter | 62/61 | 14.6/15.9 | 30.8/32.9 | 35.6/34.9 | NR | |
| CR for FFR ≤0.80 | ||||||||||||||
| FFR-guided CR vs. angiography-guided CR | ||||||||||||||
| FLOWER-MI (2021)5) | 2016–2018 | FFR- versus angio-guided | Staged (96%) | FFR-guided: 586 | Any death, MI, urgent RR | 12 months | ≥50% DS with ≥2 mm diameter | 62.5/61.9 | 18.3/14.2 | 25.9/20.1 | 29.8/34.6 | 50/50 | ||
| Angio-guided: 577 | CR for FFR ≤0.80 in FFR-guided group | |||||||||||||
CR = complete revascularization; CVA = cerebrovascular accident; DM = diabetes mellitus; DS = diameter stenosis; EF = ejection fraction; FFR = fractional flow reserve; HF = heart failure; ID-RR = ischemia-driven repeat revascularization; MI = myocardial infarction; NR = not reported; QCA = quantitative coronary angiography; RR = repeat revascularization; STEMI = ST-segment elevation myocardial infarction; 3-VD = 3-vessel disease.
SELECTION OF NON-CULPRIT LESIONS FOR COMPLETE REVASCULARIZATION
Although CR has clearly been shown to be beneficial in patients with STEMI, clinical trials have used different criteria to select targets for non-culprit PCI (Table 1). In most studies, non-culprit lesions were assessed angiographically, and PCI was performed based on the angiographic lesion severity with a cutoff DS of 50% to 70%. In COMPLETE trial, CR was achieved by revascularizing non-culprit lesions with DS of ≥70% on visual assessment or 50–69% with positive FFR ≤0.80.1) However, less than 1% of the lesions were assessed by FFR. In fact, all the benefits of non-culprit PCI were observed among lesions with DS of ≥80% by visual assessment (≥60% on laboratory assessment).1) These results support the usefulness of an angiography-guided non-culprit PCI, especially when the degree of stenosis is clearly severe on visual assessment.
However, it should also be noted that the angiographic severity of non-culprit lesions can be overestimated in the acute phase of MI, which could lead to stenting hemodynamically nonsignificant lesions. In this regard, feasibility and usefulness of physiology-guided PCI have been studied in patients with acute coronary syndrome. In patients with STEMI, DANAMI-3-PRIMULTI and COMPARE-ACUTE trials consistently showed significantly better clinical outcome following FFR-guided CR compared with culprit-only PCI.3)4) These outcome trials support that FFR-guided PCI is also beneficial in patients with MI, and FFR-guided CR is an effective strategy in patients with STEMI and MVD.
PHYSIOLOGY- VERSUS ANGIOGRAPHY-GUIDED REVASCULARIZATION OF THE NON-INFARCT-RELATED ARTERIES
Although both angiography-guided and FFR-guided non-culprit PCI have been proven to be beneficial in patients with STEMI, there has been lack of evidence as to which strategy is better in this population. Recently published FLOWER-MI was the first RCT which directly compared angiography-guided versus FFR-guided CR in patients with STEMI and MVD.5) In this study, 577 and 586 patients were randomly assigned to angiography-guided or FFR-guided strategies, respectively. During 1-year follow up, there was no significant difference between the 2 strategies in primary outcome, a composite of death, MI, and urgent revascularization (HR, 1.32; 95% CI, 0.78–2.23; p=0.31). Authors noticed that the event-rate curves for the primary outcome diverged after 6 months and hypothesized that the untreated non-culprit lesions in the FFR-guided group could have worsened during the follow-up.
However, the results of this trial need to be interpreted with caution. First, the incidence of periprocedural MI, which was part of the primary outcome, was significantly higher in FFR-guided PCI group (7 out of 18 nonfatal MIs in FFR-guided group versus 2 out of 10 nonfatal MIs in angiography-guided group). Considering that the angiography-guided strategy resulted in more interventions, higher incidence of periprocedural MIs in FFR-guided group could be an artifact, thereby contributing to the numerical difference in the primary outcome. Second, 7 out of 9 deaths occurring in the FFR-guided group were due to non-cardiac etiologies (e.g., cancer, end-stage renal disease, post-trauma hemorrhage, or acute pancreatitis) and only 2 deaths were cardiac related, whereas 7 out of 10 deaths occurring in the angiography-guided group were cardiac related. Third, although failure rates of the non-culprit PCI were reported to be same in both groups (4.7% for each), 5 non-culprit PCIs in FFR-guided group resulted in post-procedure thrombolysis in myocardial infarction (TIMI) flow of 0, whereas none in angiography-guided group had post-procedure TIMI flow of 0. Fourth, 15.7% of interrogated lesions had missing FFR value, suggesting lack of core laboratory validation of FFR values in the trial. These facts raise concerns regarding the reliability of results of this trial. Despite these concerns being unfavorable to the FFR-guided strategy, there was no significant difference in clinical outcomes between the 2 strategies, and significantly less PCI and stents were required in the FFR-guided strategy.
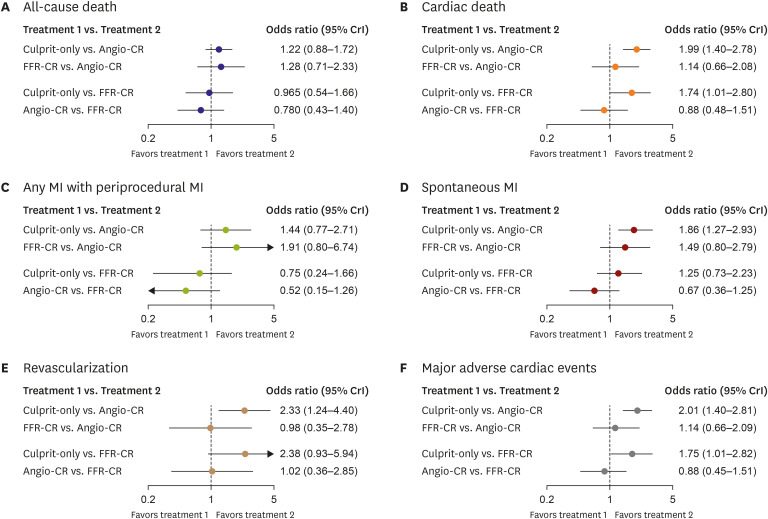
To further investigate this topic, we performed a network meta-analysis using the Bayesian extension of the hierarchical random-effects model to extract indirect comparison results in pairs. As shown in Figure 1, both angiography-guided and FFR-guided CR strategies were associated with lower risks of cardiac death and MACE compared with culprit-only PCI strategy. There was no significant difference between angiography-guided and FFR-guided CR strategies in the risk of all-cause death, cardiac death, MI, revascularization, and MACE. In sensitivity analysis, non-significant trend of MI favoring angiography-guided CR was mostly affected by the results of a small trial which compared FFR-guided CR with culprit-only PCI.7)9) In studies of Dambrink et al.7) and Ghani et al.,9) there were significantly more deaths (5.1% vs. 0%) and MIs (17.7% vs. 0%) in the FFR-guided CR group than the culprit-only PCI group,9) which were not seen in more recent, larger trials.3)4) This suggests that the results of the trial could have been biased. Furthermore, heterogeneous definitions of MI (especially, periprocedural MI) among the studies were major sources of bias in interpreting comparative prognosis between angiography-guided and FFR-guided strategies. Nevertheless, the overall results of the current network meta-analysis emphasize the importance of CR in patients with STEMI and MVD, regardless of the strategy for non-culprit PCI.
Figure 1
Network meta-analysis comparing culprit-only PCI, FFR-guided, and angiography-guided CR.
(A-F) Results from network meta-analysis using the Bayesian extension of the hierarchical random-effects model are presented.
ACS = acute coronary syndrome; Angio-CR = angiography-guided complete revascularization; Culprit-only = culprit-only percutaneous coronary intervention; CR = complete revascularization; CrI = credible interval; CVA = cerebrovascular accident; DM = diabetes mellitus; DS = diameter stenosis; EF = ejection fraction; FFR = fractional flow reserve; FFR-CR = fractional flow reserve-guided complete revascularization; HF = heart failure; ID = ischemia-driven; MI = myocardial infarction; NR = not reported; QCA = quantitative coronary angiography; RR = repeat revascularization; VD = vessel disease.
FUTURE PERSPECTIVES
We discussed the importance of CR in patients with STEMI and compared different strategies to select targets for non-culprit PCI. Based on the results of available trials and the present network meta-analysis, both angiography-guided and FFR-guided CR would provide similar benefits over culprit-only PCI in patients with STEMI and MVD. Considering the benefit of angiography-guided CR was mostly seen among non-culprit lesions with DS of ≥80% on visual assessment,1) and that FFR would be concordant in most of those lesions, it may be reasonable to consider revascularization of such severe lesions without further tests. If the non-culprit lesions are intermediate in severity or unclear based on visual assessment, FFR-guided strategy can be used as a reliable and objective tool to select targets for non-culprit PCI, providing similar benefits with less stents compared with an angiography-guided strategy. In addition, comparable outcomes between the 2 strategies allow the operators to choose one strategy over the other based on various factors, such as operator experience, availability of physiologic assessment, and overall cost, until more data become available. It should be noted that there has been very limited evidence regarding the direct comparison between angiography-guided and FFR-guided strategies. Therefore, the results from the current network meta-analysis should be regarded as hypothesis generating.
Ongoing FRAME-AMI (NCT02715518) trial which directly compare angiography-guided and FFR-guided strategies will provide more insight into the optimal CR strategy in patients with STEMI and MVD. Another interesting question is whether preventive PCI of non-culprit lesions, according to the intravascular imaging-based vulnerability would prevent future events. The concept of vulnerability-guided PCI has not yet been proven to be beneficial in this population. Future studies such as the OCT CONTACT trial (NCT04878133) will test this concept.
CONCLUSIONS
In Bayesian network meta-analysis of 13 RCTs, both angiography-guided and FFR-guided CR strategies showed significantly lower risk of MACE than culprit-only PCI in patients with STEMI and MVD. However, there was no significant difference between angiography-guided and FFR-guided CR strategies in the risk of MACE and its individual components including all-cause death, cardiac death, MI, and revascularization. Further RCT is needed to evaluate direct comparison between angiography-guided and FFR-guided CR strategies in patients with STEMI and MVD.
 XML Download
XML Download