

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A rigid spino-pelvic fixation to anchor long constructs is crucial to maintain the stability of long fusion in spinal deformity surgery. Many authors reported that S1 promontory (tricortical purchase) screws without supplemental fixation are associated with fixation failure which causes high pseudarthrosis rate and poor outcome234). Sacropelvic fixation is most commonly used during long segmental fusions extending to the sacrum for spinal deformity, correction of pelvic obliquity, high-grade lumbosacral spondylolisthesis (grade III or higher), sacrectomy, osteoporotic fractures or traumatic fractures, substantial osteoporosis in the setting of lumbosacral fusion36). In addition, revision of symptomatic lumbosacral pseudarthrosis with loosened S1 screws is another indication for extension of fixation to the pelvis. Iliac fixation with iliac screws is one of the most commonly used techniques for sacropelvic fixation. However, it requires separate fascial skin incisions or wide muscle dissection to expose the ilium or the use of offset connectors which might cause skin prominence over the posterior superior iliac spine. This increases operation time, possibility of deep wound infection, and risk of poor wound healing.
S2 alar-iliac (S2AI) screws have been described by O'Brien et al.7) in pediatric and adult populations, respectively. Besides obtaining immediate stability and proper biomechanical strength of constructs, the S2AI screws have some more advantages1). It could eliminate the need for cross-connectors which minimizes implant prominence because it might be placed in-line with S1 promontory screws. Additionally, it does not require the dissection of the subcutaneous tissue over the iliac crest or the sacral paraspinal muscle. The implant can be completely covered by an intact layer of muscle and minimally disturbed skin.
We report a free-hand insertion technique of S2AI screws which can reduce radiation exposure to the surgeons and surgical time, and the anatomic feasibility of the S2AI screw placement in-line with conventional iliac wing screw in four cadavers.
MATERIALS AND METHODS
Four Korean fresh-frozen human cadavers were procured and surgically dissected from proximal thoracic to pelvis, leaving bony structures and ligaments intact. Each specimen was inspected and examined under fluoroscopy to rule out deformities, prior surgery, or malignancy. 8.5×90 mm iliac screws (CD horizon® Legacy™ Spinal System, Medtronic, Memphis, TN, USA) were placed for the S2AI screw.
Surgical technique
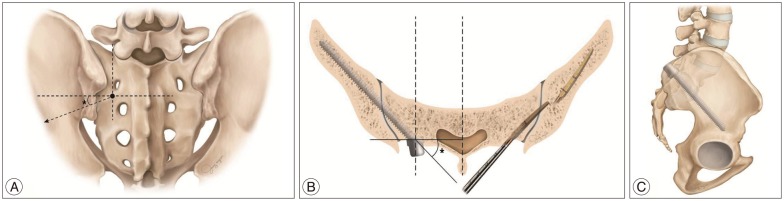
Free hand S2AI screw placement was performed using anatomic landmarks. The starting point of the S2AI screw is located at the midpoint between the S1 and S2 foramen and 2 mm medial to the lateral sacral crest (Fig. 1A). Additionally, the entry point for S2AI should be harmoniously located with S1 screw entry point. A 3 mm cutting burr was utilized to create posterior cortical breach, approximately 5 mm in depth. The gearshift was initially pointed dorsally to avoid penetration of the anterior sacrum (Fig. 1B). Gearshift was advanced from the desired starting point toward the sacro-iliac (SI) joint directing approximately 20° angulation caudally in sagittal plane and 30° angulation horizontally in the coronal plane connecting the posterior superior iliac spine (PSIS). After inserting the gearshift tip approximately 3–4 cm until reaching the SI joint, the gearshift was removed and confirmed 5 bony walls (medial, lateral, superior, inferior and bottom) through ball-tip probing. This step identifies the intraosseous placement of the screw trajectory. It could be hard to advance the gearshift because of the cortical wall of the SI joint. By cautious hammering the gearshift with the mallet, it could penetrate the cortical wall of the SI joint. After crossing the SI joint, the tip of the gearshift turned to face ventral (Fig. 1B). The gearshift was preceded through the cancellous channel of the ilium heading above the superior rim of the sciatic notch. It is important to make sure that surgeon to feel the bone of entire length of the tract. A ball-tip probe was utilized to palpate the 5 bony borders ensuring that the screw would be located intraosseously. At this point, if a soft tissue breach is palpated, there may be an opportunity to redirect the gearshift probe into an appropriate position into the iliac crest. If any wall including the anterior has been breached, the iliac wing crest may be salvageable. Otherwise, we place bone wax or gelfoam in the sacral hole to eliminate the bleeding and re-angle the pedicle finder with a more appropriate trajectory. The S2AI screw tract was under-tapped with a 2 mm less diameter tap than the intended screw. Following this, the tract is palpated again to make sure that the osseous borders are intact. This second palpation will often allow palpation of distinct bony ridges confirming intraosseous position and the tract length was remeasured by the length of the ball-tip probe marked with a hemostatic clamp. This measurement was compared directly adjacent to the screw to be placed to ensure appropriate screw length. Finally, the screw was inserted in the same direction until the screw head is placed in-line with S1 promontory screw head.
It is imperative that the surgeon document intraosseous placement via fluoroscopy or plain radiography. On the lateral and coronal plane radiograph, the S2AI screws should be placed above the superior rim of the sciatic notch (Fig. 1C). The most important structure to be avoided is the sciatic notch. However, rather than using a trajectory that passes far from the notch, the ideal trajectory of the S2AI screw is situated immediately above the notch so that the bottom threads of the screw will be in contact with the cortical bone forming the upper limit of the notch, providing a better pull-out strength5).
S2AI screw evaluation
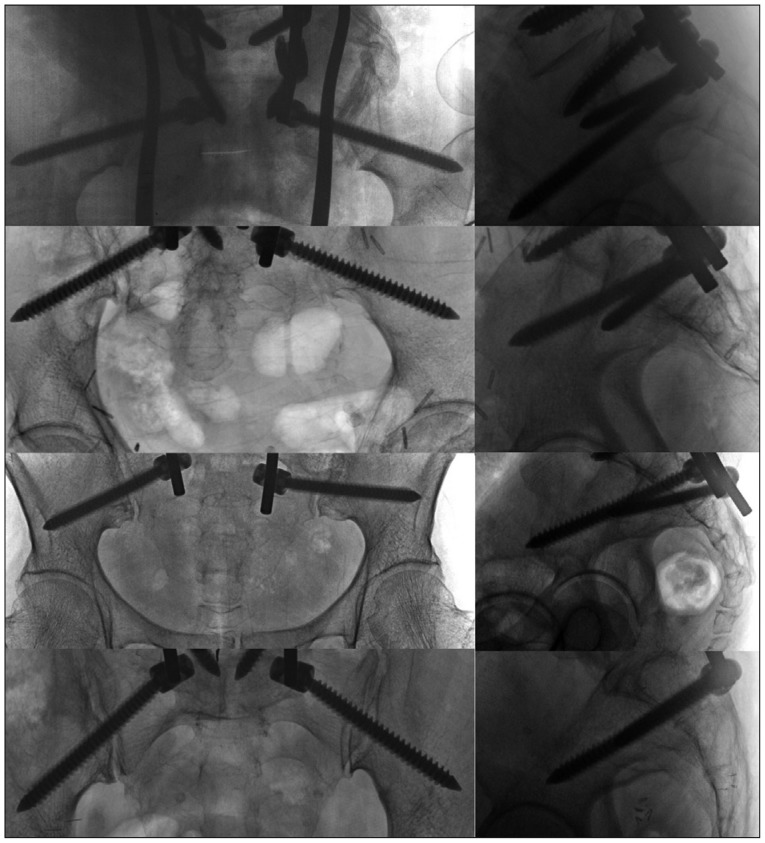
Our criteria for accurate placement were as follows; first, after under-tapping, two surgeons confirmed the screw trajectory was located intraosseously by palpating intact 5 bony walls using ball-tip probe. Second, we checked AP and lateral C-arm fluoroscopy; the screws should not violate sciatic notch, acetabulum; the screws should not evade the pelvic cavity; the screws should locate in the ilium.
RESULTS
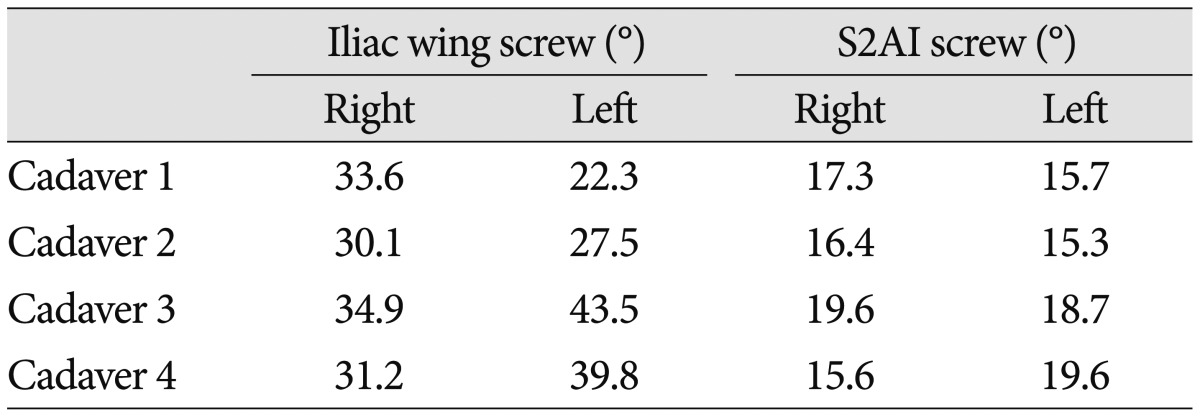
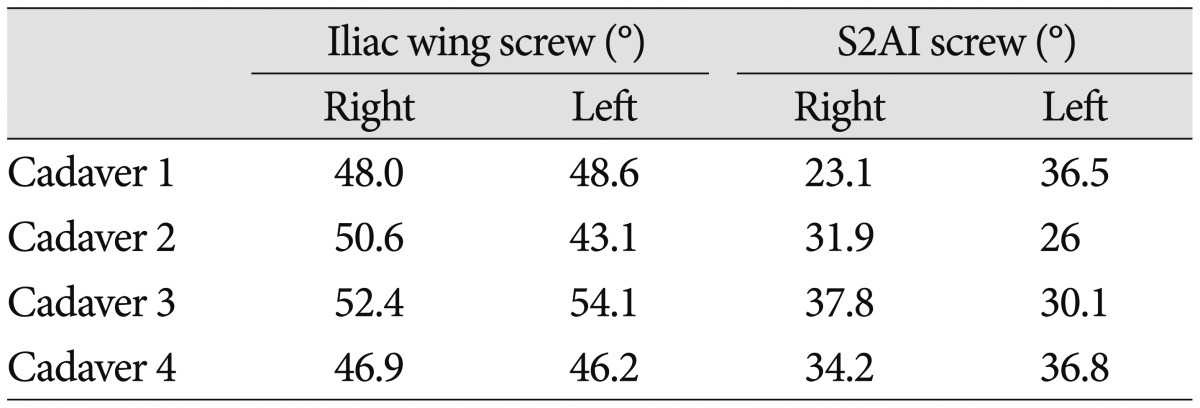
A total of eight S2AI screws were inserted in four cadavers. All screws inserted into the iliac crest were all evaluated by C-arm and naked eye examination. Among 8 S2AI screws, all screws were accurately placed (Fig. 2). The average caudal angle in the sagittal plane was 17.3±5.4°. The average horizontal angle in the coronal plane connecting the PSIS was 32.0±1.8°. The average caudal angles and horizontal angles of the conventional wing screw were 32.9±6.7°and 48.7±3.5°, respectively (Table 1, 2).
DISCUSSION
Solid distal fixation in spinal deformity surgery is essential for providing a strong support to maintain sagittal and coronal balance. S2AI screw fixation technique has more fixed segments and stable biomechanical torsion due to the direction and the length of the screws, leading to more reliable stability compared to traditional iliac screw fixation8). S2AI screw fixation technique provides as far anteriorly and laterally to the spine as possible. In addition, S2AI screws traverse the cortical bone of the sacrum, the SI-joint space, and the cortical bone of the ilium, which significantly enhances the pullout strength of the screws.
It has been reported that 60% of S2AI screws violated the articular cartilage of the SI joint, because the superior portion of the lateral projection of the sacrum to the ilium corresponds to an articular area7). However, fusion of the SI joint after placement of S2AI screws has proved to provide significant pain relief in patients with pain related to SI joint degeneration5).
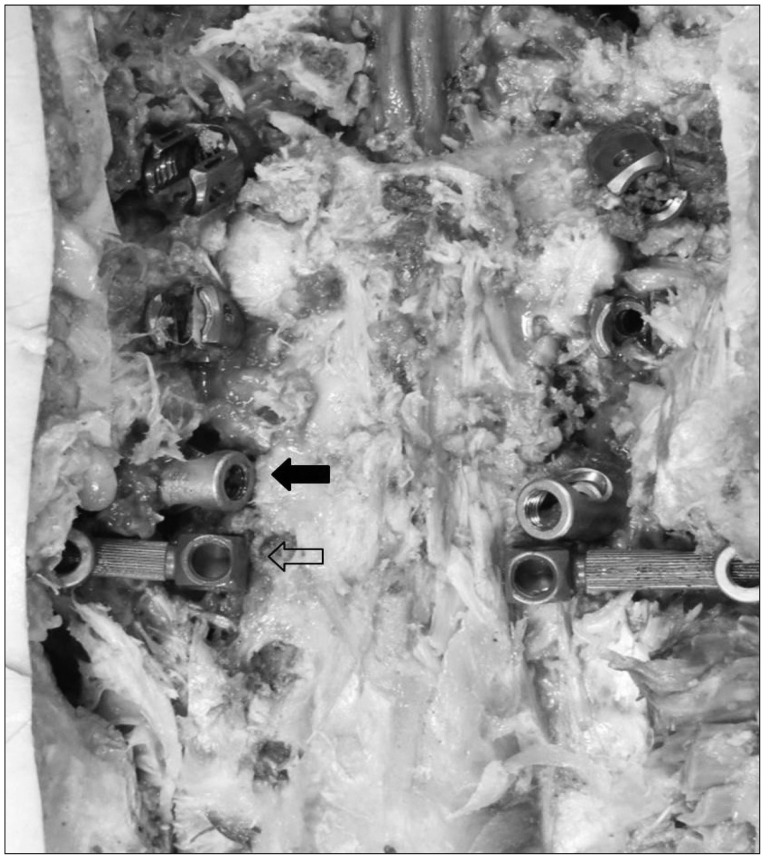
In this study, all S2AI screws were in-line with the S1 promontory screws. Furthermore, all S2AI screws were in-line with the conventional iliac wing screws with the offset connector (Fig. 3). We consider it is feasible for the S2AI screw to place in-line with the S1 promontory screws and the conventional iliac wing screws.
Screw placement under fluoroscopic guidance requires more surgical time and results in radiation exposure to surgeon during surgery. Surgeons should protect themselves from radiation exposure with wearing eyewear, thyroid shields, and lead aprons. However, protecting gears are heavy and wearing them causes fatigue to surgeons, which decreases surgeons' concentration. Even though a surgeon wore all the protecting gears mentioned above, the surgeon's hands could not be saved from the radiation exposure. The placement of pedicle screws or S2AI screws using a free hand technique is useful for surgeon minimalizing the radiation exposure from the fluoroscopy and reducing operation time.
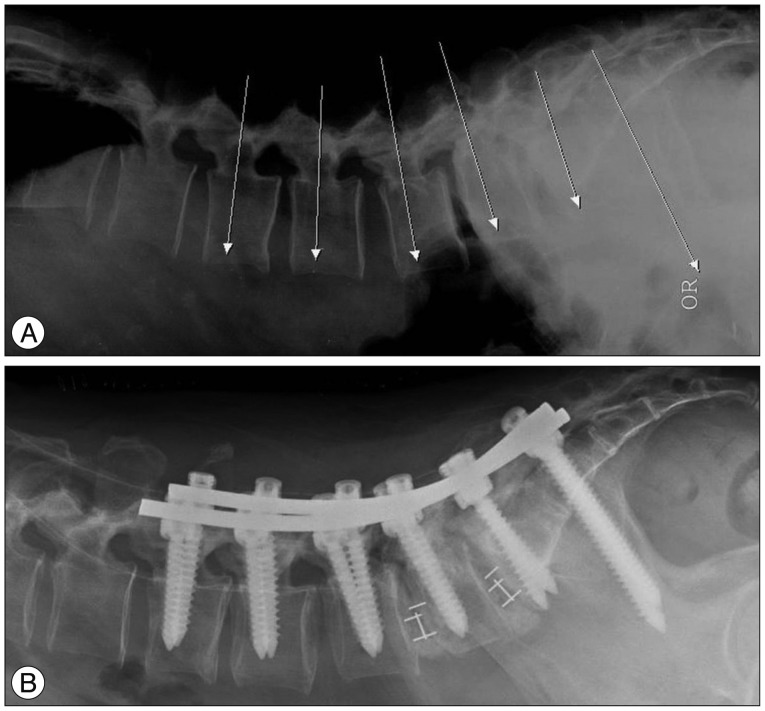
It deserves to mention our surgical tip for measuring the screw angle during the surgery. We take a portable lateral plain radiograph for leveling after flipping a patient. We draw imaginary lines for the ideal pedicle screw trajectory and S2AI screw trajectory on the lateral plain radiograph, which is placed just above the superior rim of the sciatic notch. These lines become a reference lines (Fig. 4). Based on the reference line, for free hand screw insertion, we can estimate or modify the pedicle screw angle and the caudal angle for the S2AI screw.
 XML Download
XML Download