

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Typically, retropharyngeal hematomas have been reported to be related with anticoagulant therapy, iatrogenic injury, infections, foreign body ingestion, and vascular lesions145614161820). Although major trauma, such as cervical spinal fracture, has caused retropharyngeal hematomas61017), minor trauma is rarely related with a large retropharyngeal hematoma, and only a few cases of anterior longitudinal ligament (ALL) 1234567891011121314151617181920) injury related with retropharyngeal hematoma without fracture have previously been reported79121315).
The treatment of choice for retropharyngeal hematoma is generally considered to involve conservative care79121315). However, we experienced that early surgery on two rare cases with a life-threatening large retropharyngeal hematoma related with ALL injuries would be better for early recovery of patient. Here, the authors describe those two cases.
CASE REPORT
Case 1
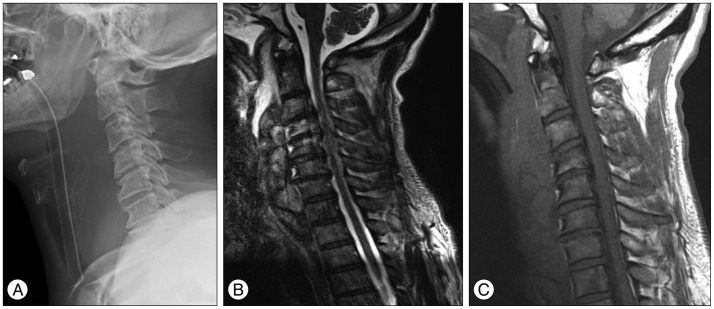
A 51-year-old man without any medical history including anticoagulant or antiplatelet treatment visited the emergency room with neck pain and dyspnea after falling 4 hours previously. There were no abnormal findings on neurological examination. Serious neck swelling was observed and lateral neck X-ray showed severe widening of the prevertebral space (Fig. 1A). Due to dyspnea progression, emergency endotracheal intubation was performed. T2-weighted sagittal magnetic resonance imaging (MRI) showed a longitudinal mass with heterogeneous signal intensity in the retropharyngeal space from the C3 to T2 levels. T1-weighted sagittal MRI also showed the longitudinal mass with low signal intensity. There was no definite fracture or ligament injury (Fig. 1B, C). Computed tomography (CT) with angiography also showed no definite fracture or vessel injury. We surmised that the MRI findings might be due to hematomas at different stages, but we were unable to determine the possible cause.
We decided to operate on the patient on the following day because it would take long time to wait for absorption of large amount of hematoma with an endotracheal tube.
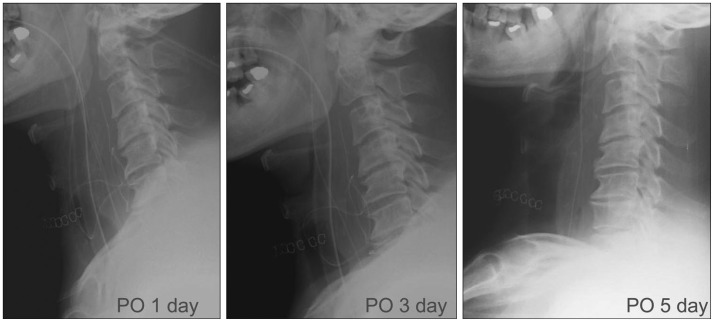
The usual right-sided Smith-Robinson approach was used. We easily found the hematoma capsule after esophageal retraction to the left side. Suction and irrigation were used to remove the dark-colored hematoma. After almost all of the hematoma was removed, we identified partial injury of the ALL at the C3-4 and C6-7 levels. After identifying that there was no vascular injury or active bleeding, closure was performed after leaving the drainage catheter. The duration of surgery was 30 minutes. After identifying a daily gradual decrease in prevertebral soft tissue thickness on serial lateral X-ray, extubation was performed on the fifth postoperative day (Fig. 2). The patient was discharged without any postoperative sequelae on the seventh postoperative day.
Case 2
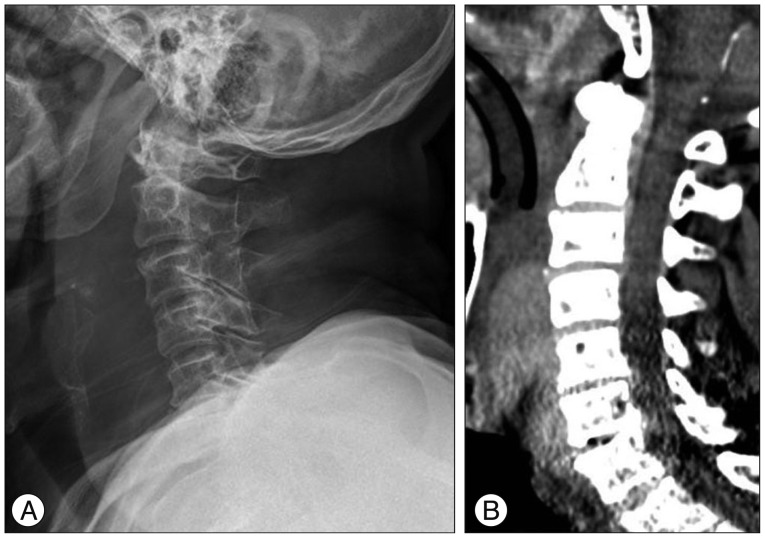
A man of 78 years of age without any medical history including anticoagulant treatment or antiplatelet showed dyspnea and neck swelling after falling. His forehead was seen to be bruised on physical examination. There were no abnormal findings on neurological examination. Because his dyspnea progressed, endotracheal intubation was performed. Although MRI was not
possible due to poor compliance, X-ray and CT angiography were performed. A lateral image X-ray showed diffuse prevertebral swelling and CT angiography showed prevertebral hematoma and a dark air density region at the C6-7 disc (Fig. 3). There was no fracture or vascular injury on CT angiography. The patient was suspected to have an ALL injury at the C6-7 level and early surgery was performed based on our experience in the above case. The same approach was used and hematoma removal was uneventful. ALL injury was identified at the C3-4 level
and the operation time was also 30 minutes. After identifying a daily gradual decrease in prevertebral soft tissue thickness on serial lateral X-ray, the patient was extubated on the fifth postoperative day. The patient was discharged without any postoperative sequelae on the eighth postoperative day.
DISCUSSION
The retropharyngeal space, which is located between the middle and deep layers of the cervical fascia, extends from the skull base to the superior mediastinum at the level of the second thoracic vertebra. Although compact, the retropharyngeal space is important in the neck because it is located dorsal to the airway. Upper airway obstruction due to retropharyngeal hematoma can be life-threatening8). Although no surgeon specializes in the anatomy of this region, this space is a route used by spine surgeons to access the cervical spine, and spine surgeons sometimes encounter postoperative retropharyngeal hematomas11). Thus, the retropharyngeal space is familiar to spine surgeons who can remove hematomas easily and quickly.
In the majority, a traumatic large amount of retropharyngeal hematoma occurs after a cervical vertebral fracture or vascular injury after high-energy accidents. However, a life-threatening large retropharyngeal hematoma caused by ALL injury has been rarely reported8121319). Thus, we could easily draw the difference between retropharyngeal hematomas with or without ALL injuries. In major trauma, we should consider much more conditions such as spinal cord injury or reconstruction of vessel or vertebrae in addition to removal of hematoma. Thus, we believe that retropharyngeal hematomas related with ALL injury developed after minor trauma can be easily treated and clinical course is better than above condition. Although a previous report recommended cervical fusion surgery to the patient9), we believed that more follow up without fusion would be better in a small tear of ALL like our patients.
The exact causes of hematomas in this space have not definitively been determined because almost all cases are managed conservatively by intubation or tracheostomy1319). However, CT angiography can show vessel injury via contrast leakage around the injured vessel. In the present cases, we were unable to find any vessel or ligament injury on preoperative examination. Although one report suggested that sagittal MRI can be used to find ALL injuries9), it is difficult to find small-sized ligament injuries on MRI. Moreover, MRI cannot be performed in some patients, such as the patient in the second case report. Thus, we believe that many previously reported cases of unknown causes that were conservatively managed might have involved small-sized ALL injuries and minor vascular injuries around the injured ligament, based on our experiences in these two cases.
The initial treatment of patients with a life-threatening large retropharyngeal hematoma should be airway management, such as endotracheal intubation or tracheostomy. Although the treatment of retropharyngeal hematoma is controversial, primarily conservative care is advocated for 2-4 weeks3891213). Surgical intervention is sometimes necessary, especially for patients with large-sized hematomas or when conservative treatment fails. We also believe that early surgery of life-threatening large hematoma will provide better outcomes than conservative treatment. The advantages of early surgical treatment include a short hospital stay, good prognosis, and rapid convalescence38). The surgical approach previously recommended was a transoral or anterior cervical approach23813). However, we believe that the anterior cervical approach that is simple and usually used for cervical spinal surgery is the most proper surgical route because a wide surgical field can be obtained and there is no chance of contamination, unlike with the transoral approach. After surgery, daily lateral X-ray follow-up is helpful for endotracheal tube removal.
 XML Download
XML Download