

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Computed tomography (CT) scan for initial evaluation of traumatic brain injury (TBI) is well established1171922). Repeated CT scan is also performed for TBI occasionally. But the indication and timing for repeated CT scans in pediatric patients are not well established236). It may expose the patients to unnecessary harmful radiation exposure especially in children8). Besides, it may increase the cost of hospital care and there were some risks during transporting patients and sedation for irritable or incooperative patients. Accordingly, some authors argued that routine repeated CT scan should be avoided without evidence of clinical deteriorations421). On the other hands, some studies had shown that routine repeated CT scan could detect the progression of hemorrhage earlier and prevent or minimize the secondary brain injury with early intervention91418). In our study, patients were classified into several small groups according to the trauma mechanisms, type and amount of hemorrhage and initial Glasgow Coma Scale (GCS) to identify which influenced on the therapeutic plans or outcomes based on the repeated CT scan.
MATERIALS AND METHODS
All patients of age 0 to 18 years that had come and admitted to our hospital for head trauma between March, 2007 and December, 2013 were enrolled and retrospective chart review was done. Almost all patients had taken repeated CT scan at least two times before discharge. Patients were classified into 8 subgroups according to trauma mechanisms. Type and amount of hemorrhage or fracture and changes in the amount of hemorrhage on repeat CT were analyzed as well as initial GCS, Glasgow Outcome Scale (GOS), 6 months after trauma, need for surgical intervention. Severity of trauma based on GCS was classified into mild (GCS 13-15), moderate (9-12), severe (3-8) TBI groups. Lesions found at initial CT scan were classified into several groups including epidural hemorrhage (EDH), subdural hemorrhage (SDH), intracerebral hemorrhage (ICH), subarachnoid hemorrhage (SAH) or intraventricular hemorrhage (IVH), skull fracture without hemorrhage and diffuse axonal injury (DAI). We measured volume of hemorrhage from each CT scans to identify whether there were progressions or not. Patient's age, sex and interval between initial and repeated CT scan, GOS were recorded.
Evaluating factors (intracranial lesions classification and volume measurement and mechanism of injury)
Positive findings revealed from CT was classified into several types. These types included EDH, SDH, ICH, DAI, skull fracture without hematoma, SAH or IVH. Focal petechial deep white matter hematoma was regarded as DAI. Multiple lesions in a patient were recorded separately for the proper analysis. The volume of hematoma was measured by simple summation formula (0.5×height×depth×length)15). and classified into 3 groups (0-9 cc small, 10-19 cc medium, 20-29 cc large) according to their amount. All patients were classified into 8 subgroups according to the mechanism of injury with chart review. These included motor vehicle collision, pedestrian struck, bicycle collision, motorcycle collision, falls, beating, sports and suicidal accident.
Indications of surgery
Epidural hematoma greater than 30 cc was evacuated regardless of the patient's neurological status such as GCS score5). Another types of lesions such as SDH, ICH, depressed skull fracture, surgery was considered by CT findings including amount, depth and midline shifting correlated with patient's clinical status.
Statistical analysis
Risk factors of progression on repeated CT and of need for delayed surgery were analyzed with t-test for continuous variables such as age group with presenting as mean±standard deviation (SD) and Pearson's chi-square test for categorical variables such as sex, GCS, mechanism of injury, type of lesions. Independent associations were also analyzed by binary logistic regression with calculating odds ratios (ORs) and confidence intervals (CIs). At a later time, multivariate logistic regression was used to compare differences between the amount of hematoma for each types of lesions that caused delayed surgical intervention. The SPSS version 20.0 (IBM Corporation, Armonk, NY, USA) was used and p-values less than 0.05 were considered statistically significant.
RESULTS
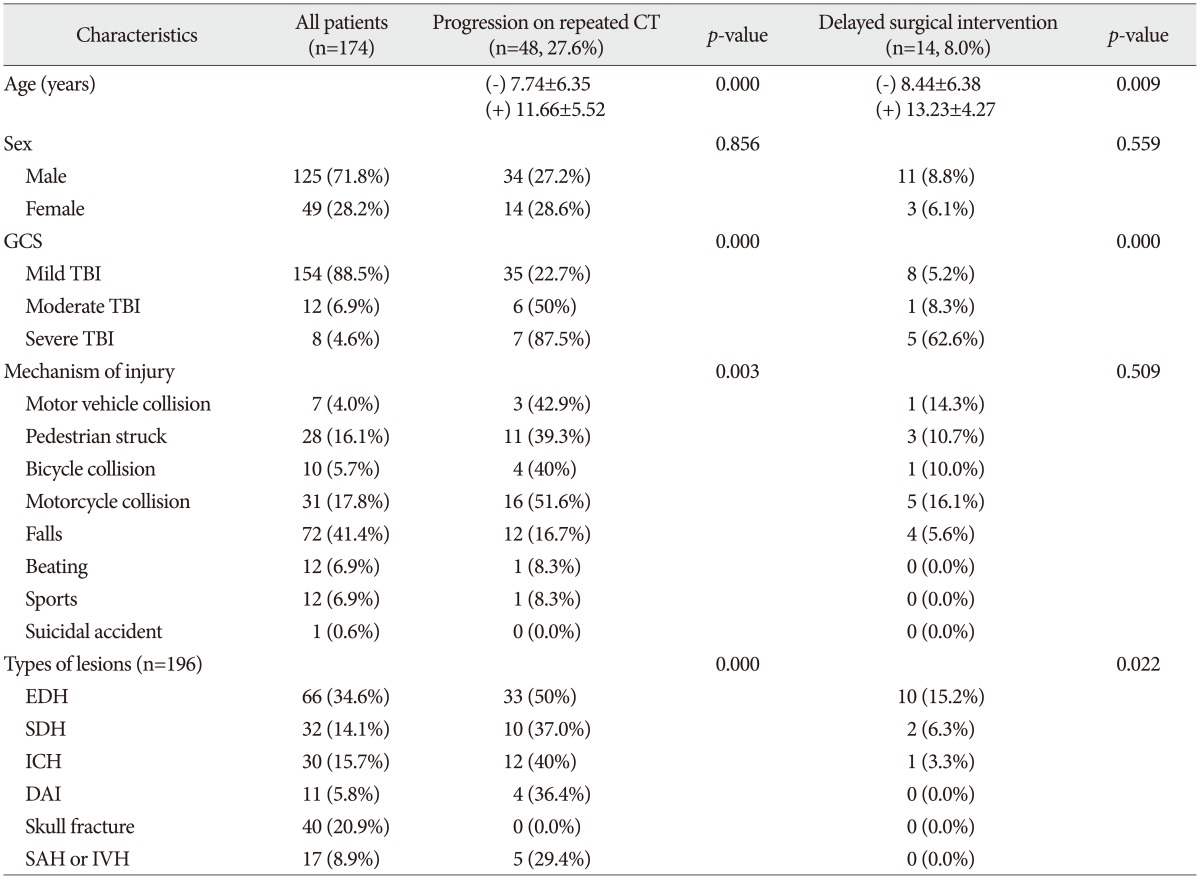
Total 269 patients were admitted to our hospital for traumatic brain injury between March, 2007 and December, 2013. 9 patients underwent immediate emergency operation. Total 174 patients received repeat head CT within 24 hr after initial head CT scan. 125 (71.8%) patients were male and 49 (28.2%) patients were female. Mean age was 5.7 years with range from 1 month to 19 years. There were 154 (88.5%) mild TBI, 12 (6.9%) moderate TBI and 8 (4.6%) severe TBI based on GCS score. Falls (n=72, 41.4%) were leading cause among mechanism of injury groups, followed by motorcycle collisions (n=31, 17.8%). Total 196 lesions were found among 174 patients and EDH (n=66, 34.6%) was the leading type of lesions followed by skull fracture (n=40, 20.9%), ICH (n=30, 15.7%), SDH (n=32, 14.1%) in order. Number of total patients and lesions categorized by progression on repeated CT and delayed surgical intervention were recorded on Table 1.
Progression of intracranial lesions on repeated CT scan
Of the 174 patients who underwent repeat head CT, progression of intracranial lesions on repeat CT scan were found at 48 (27.6%) patients. Using t-test, age differences were found between progression on repeated CT and non progression. Progression on repeated CT group (mean±SD, 11.66±5.52) were significant older than non progression group (mean±SD, 7.74±6.35). Logistic regression analysis was performed and progression of volume of hematoma were determined for age, sex, initial GCS score, mechanisms of trauma, lesion types. Results of analysis was demonstrated on Table 2. Among those groups, age (OR 1.09, p=0.013), moderate TBI (OR 5.06, p=0.022), severe TBI (OR 34.62, p=0.002), EDH (OR 10.31, p<0.001) had significant relationship with progression of volume of hematoma. ICH (OR 3.00, p=0.067) was relatively found to be at risk of progression. Using Pearson's chi-square test, there was significant differences among mechanism of injury groups (p=0.003) between progression on repeated CT and non progression on repeated CT groups with leading percentage of progression in motorcycle collision groups (n=16 of 31, 51.6%). But logistic regression revealed no such significant findings as an independent risk factor of progression on repeated CT. Another types of intracranial lesions, sex, mechanism of trauma were not significantly associated with progression.
Delayed surgical intervention
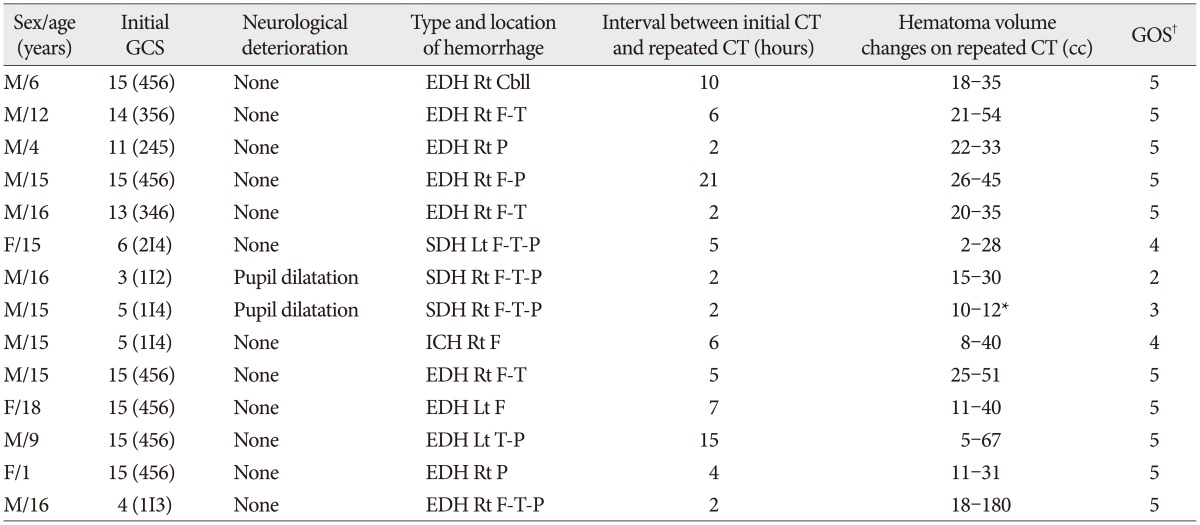
Multivariate logistic regression analysis for the risk factors of delayed surgery was performed same as hematoma expansion. Results of analysis was demonstrated on Table 3. Severe TBI group (OR=136.17, p<0.001), EDH group (OR=14.95, p=0.012) were significantly associated with delayed surgical intervention. Age was not significantly associated (p=0.263) in contrast to being significantly associated with progression on repeated CT. Among 174 patients who received repeat CT, 14 (8.0%) patients underwent delayed surgical intervention with or without clinical deterioration after repeat CT. 10 patients for EDH, 2 patients for SDH, 1 patient for ICH, 1 patient for brain swelling with midline shifting underwent surgery for hematoma evacuation or decompression. Table 4 demonstrate characteristics of patients underwent delayed surgery. Among these patients, only two patients had neurological deterioration (pupillary dilatation) and performed immediate follow up head CT scan before surgery. Their characteristics were described on Table 4. All patients who underwent surgery was found to have volume of hematoma more than 30 cc on their repeat CT scan except one patient that had progression of swelling.
Type of hematoma and volume associated with surgical intervention
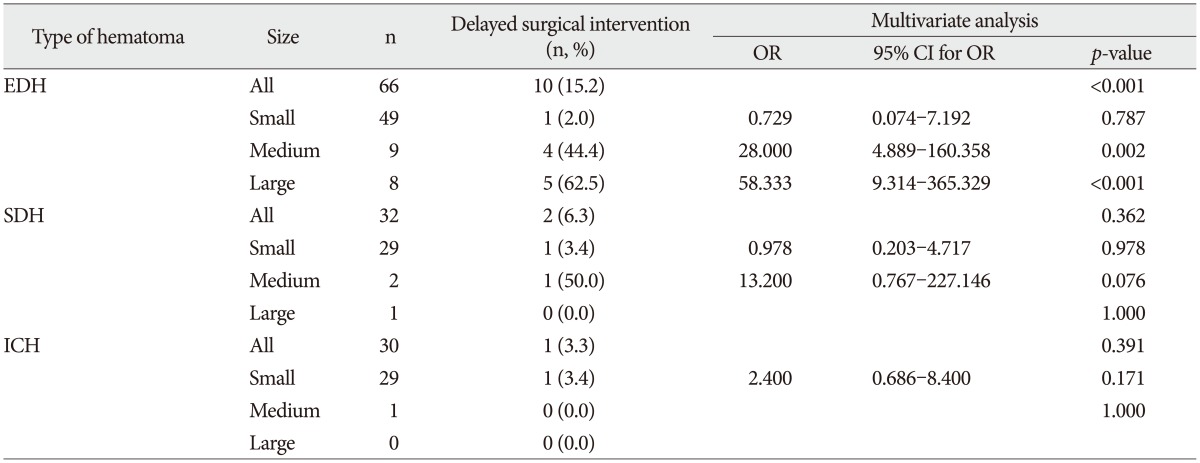
Further multivariate logistic regression analysis was performed for each type of hematoma and its volume. Results of analysis was demonstrated on Table 5. EDH, SDH, ICH were included for analysis and each were divided into 3 groups according to the initial amount (0-9 cc small, 10-19 cc medium, 20-29 cc large). Of these lesions, EDH more than 10 cc groups were significantly at an increased risk of progression more than 30 cc and underwent surgery. Medium EDH (OR=28.00, p=0.002), large EDH (OR=58.33, p<0.001) were associated to progression comparison to small EDH (OR=0.73, p=0.787). Another hematoma groups were not significantly associated.
DISCUSSION
It is much harder to perform exact neurologic examination for the pediatric patients than adult patients. Occasionally it may lead to miss the early deterioration of their neurologic status and delay the golden time for intervention. Besides, all acute traumatic brain lesions have a chance to be progressive479111314161823). For these reasons, routine repeat head CT scan was performed in many pediatric patients. In our study, there were 48 (27.6%) progression on repeat CT among 174 patients and 14 (8.0%) patients underwent delayed surgical intervention. It is similar result to previous studies that progression on routine repeat CT reported 21-50% and need for delayed surgical intervention after repeat CT reported 1-24%2610131418).
Our study focused on the risk factors of progressive intracranial lesions and need for delayed surgical intervention including mechanisms of injury, type of intracranial lesions, GCS scores. But mechanisms of injury had no relations with progression of lesions or delayed surgical intervention on logistic regression in our study. But our study had limited records about severity of trauma mechanism, such as height of falling down, velocity of vehicle accident and so to perform more precise study, such things should be considered.
Several previous studies demonstrated that lower GCS score is a risk factor of injury progression as present study231320). Thorson et al.20) revealed that GCS score of less than 15 is associated with injury progression, and Lee et al.13) argued that severe head trauma (GCS 3-8) patients had more chance to have progression of repeat CT than in moderate head injury (GCS 9-12) patients. Aziz et al.2) showed that repeat head CT should be taken routinely in patients with intracranial hemorrhage with GCS score of 8 or less. Bata and Yung3), also concluded that of children with moderate to severe TBI, repeat head CT is more likely to alter management. As similar to those previous studies, our study demonstrated that moderate to severe TBI (GCS<13) had significant relationship with progression of volume of hematoma and severe TBI (GCS<9) was significantly associated with delayed surgical intervention after repeat head CT. On the other hand, some previous studies712) revealed that routine repeated CT is not recommended for the pediatric TBI patients. Kochanek et al.12) reviewed previous studies about pediatric TBI. Their level III recommendation based on previous study7), routine repeated CT may not be indicated in the absence of neurologic deterioration or increasing intracranial pressure (ICP). But ICP monitoring including extra-ventricular drainage, ICP probe insertion is an invasive procedure, especially more difficult to perform on pediatric patients. So there is limitation on the detection of neurologic decline and ICP monitoring in pediatric patients.
Among various types of intracranial lesions, EDH seemed to be at a risk of progression on repeat CT and EDH more than 10 cc was significantly associated with progression more than 30 cc and undergoing surgery in our study. These findings were similar to several previous studies. Howe et al.10) argued that routine repeat CT without clinical deterioration shoud be avoided but children with EDH had a higher potential for progression and routine repeat CT seems to be indicated in those cases. Durham et al.6) revealed EDH, SDH, cerebral edema, and intraparenchymal hemorrhage as a high risk lesions of progression and recommended repeated CT imaging without signs of clinical detereioration in pediatric TBI. In our study, as well as EDH revealed to be a risk factor of progression, ICH (OR 3.00, p=0.067) relatively found to be at risk of progression. In our study, differs from those previous studies, volume of hematoma was measured and demonstrated EDH more than 10 cc was at a risk of progression more than 30 cc and undergoing surgery among various hematoma lesion types. Washington and Grubb24) measured hematoma volume on serial head CT and revealed only an ICH>10 cc was independently associated with the risk of progression. This finding differed from our study but their study population was adult patients. In our study, 14 patients underwent surgery after repeated head CT. 2 patients had clinical deterioration (pupil dilatation) and underwent surgery after immediate repeated CT. Their outcomes were worse (GOS 2 and 3) than other patients underwent surgery after routine repeated CT without clinical deteriorations as seen on Table 3. These findings may suggest that early detection of the progression of hemorrhage prevent or minimize the secondary brain injury with early intervention as some authors emphasized.91418) Even a patient with initial GCS score 4 with EDH 18 cc on initial head CT and underwent surgery after routine repeat CT revealed expansion of hematoma to 110 cc had excellent outcome (GOS 5). In that case, no significant neurologic decline was found before routine repeated head CT.
CONCLUSION
Our study demonstrated that severe TBI (GCS below 9) or EDH more than 10 cc were significantly at an increased risk of hematoma expansion and altered management plans such as performing delayed surgical intervention. So in those cases, clinicians may consider repeated CT scan regardless of patient's neurological deterioration to minimize the complications. Routine repeated head CT is not necessary for EDH less than 10 cc, other types of intracranial lesions, mild to moderate TBI (GCS 9-15) patients regardless of their mechanism of injury.


 XML Download
XML Download