

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In children obstruction of Magendie's foramen is mainly congenital while in adults it is mostly acquired. In this paper we present a rare case of hydrocephalus caused by the occlusion of Magendie's foramen by a membrane due to arachnoiditis.
CASE REPORT
History and examination
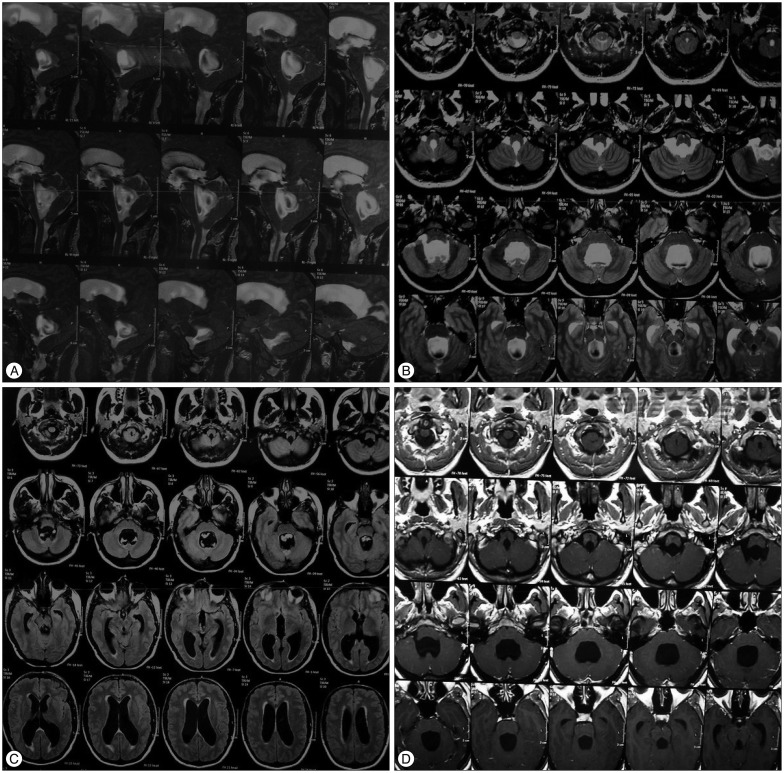
A 37-year-old woman was admitted to our emergency department with the chief complaint of headache that has gradually been deteriorating in the last month and was accompanied by blurred vision. The headache was worst in the morning and was localized in the frontal and occipital region. The patient also mentioned two episodes of vomiting and phonophobia along with the headache the last week. Physical examination was normal, however the patient complained for mild unsteadiness and recent memory loss. No loss of bladder control or urgency to urination was mentioned. As far as the patient's past medical history is concerned, an Epstein-Barr virus (EBV) infectious mononucleosis was described. The rest medical history was unremarkable. For evaluation of her symptoms the initial workup included a brain magnetic resonance imaging (MRI) which revealed significant ventricular dilatation of lateral, third and fourth ventricles with subependymal edema, without any gadolinium enhancement of the ventricular system or obvious obstruction. A T2W TSE study was also performed and demonstrated a turbulent flow of cerebelospinal fluid (CSF) in the fourth ventricle and back flow of CSF through the Monro's foramen to the lateral ventricles (Fig. 1). The patient had also undergone fundoscopic examination that showed bilateral papilledema.
Operation
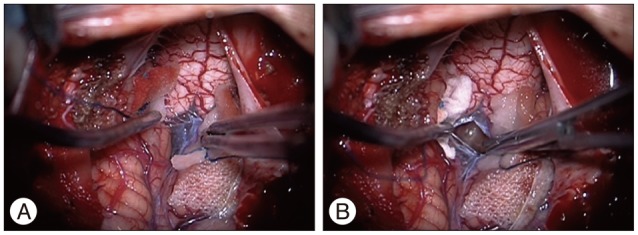
Based on the above findings a decompression on the foramen magnum was decided having established an obstruction at that level. The patient underwent a suboccipital craniotomy with C1 laminectomy. An occlusion of Magendie's foramen by a thickened membrane was recognized and the membrane was incised and removed, thus restoring the normal flow of cerebrospinal fluid between the fourth ventricle and the cerebellomedullary cistern (Fig. 2).
Postoperative course
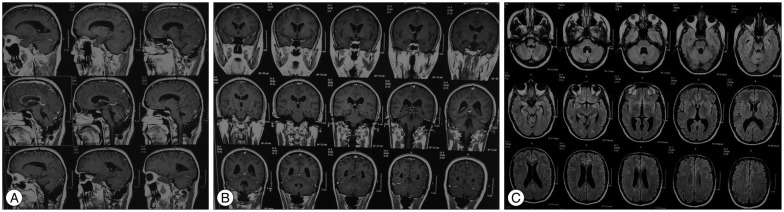
The postoperative course was uneventful. The new fundoscopic examination in two weeks revealed a reduction in papilledema and the second MRI scan showed a marked decrease in the size of the ventricles, showing therefore that cerebrospinal fluid flow through the ventricular system and subarachnoid space was restored (Fig. 3).
DISCUSSION
Membranous obstruction of the Magendie's foramen is a rare case of non communicating quadriventricular hydrocephalus. In children is usually congenital and related with Dandy-Walker Syndrome, Arnold-Chiari malformation, tuberous sclerosis, spina bifida, platybasia, achondroplasia, basilar impression and atlanto-occipital fusion9). In adults it is mostly acquired rather than congenital9). Acquired ventricuΙar outlet obstructions are reported in adults as well as children and generally occur in infection (meningoencephalitides, prenatal infection, shunting procedures, granulomatosis, venereal disease, influenza, ear-ocular-nasopharyngeal infection, Toxoplasmosis, Cysticercosis), head trauma, intraventricular hemorrhage, tumors or Arnold-Chiari malformation9,10).
Review of the literature regarding adults revealed only few cases of congenital membranous obstruction of the foramen of Magendie in which the obstruction was not associated with systemic illness or trauma2,3,6,7,9). Also only few cases related to idiopathic stenosis of the foramina of Magendie have been described1,4,5,8,10,12). The rare published cases of hydrocephalus caused by stenosis of the foramina of Magendie are usually associated with another disease, mainly Chiari Type I malformation5). In our case we present the occlusion of Magendie's foramen by a membrane due to arachnoiditis with the high suspicion of an EBV infectious mononucleosis11).
In the past the diagnosis was based on indirect data resulting from invasive methods such as ventriculography while in recent years it mainly results from brain MRI, MRI CSF flow and direct surgical exploration. However direct visualization of the membrane on MRI has been described in two cases10). Although MRI CSF flow study is more sensitive for the cerebral aqueduct, which is of smaller diameter and with an identifiable flow in the cephalocaudal axis than the fourth ventricle which is a larger structure and also has three outlets, this study is also very helpful in demonstrating Magendie's foramen obstructions. In our case, brain MRI with T2 weighted turbo spin-echo study was critical for the patient's management, as it demonstrated a turbulent flow of CSF in the third and fourth ventricle and back flow of CSF through the Monro's foramen to the lateral ventricles.
Preoperative radiological findings are very useful in deciding the appropriate surgical approach which includes the incision and removal of membrane with or without endoscopic third ventriculostomy (EVT) and CSF shunting5,10). The efficacy of ETV in the treatment of obstructive hydrocephalus and the absence of complications related to the presence of a CSF shunt, have encouraged the use of this method for treating obstructive hydrocephalus, including obstacles situated to the cerebral aqueduct and, in the fourth ventricle and the foramen of Magendie and Luschka as well5). Regarding our case a suboccipital craniotomy with C1 laminectomy was performed and the thickened arachnoid was incised and removed at the foramen of Magendie. This procedure restored the normal flow of cerebrospinal fluid between the fourth ventricle and the cisterna magna and was considered as curative because the patient remained free of symptoms thereafter. Nevertheless, a ventriculo-cisternal shunting and EVT have been proposed in case of a possible restenosis but taking the risk of catheter infection in the first case1,10).
CONCLUSION
In this study we confirm the existence of hydrocephalus caused by fourth ventricle outflow obstruction (Magendie's foramen) by a membrane probably on the basis of arachnoiditis. The obstructive nature of this rare entity is difficult to demonstrate, even on MRI images, because of the complex morphology of the fourth ventricle. Treatment with surgical exploration and incision of the thickened membrane proved to be a reliable method of treatment without the necessity of EVT or catheter placement.
 XML Download
XML Download