

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pituitary adenomas reported an overall prevalence of 16.7%8) comprise a diverse group of tumors. Histologically, pituitary adenomas are considered to be benign. However, they may grow large and extend into surrounding structures resulting in neurological complications including visual impairment6). If pituitary adenomas are not treated, vision will continue to deteriorate and blindness might result29).
Typically, nonfunctioning adenomas present as macroadenomas that cause neurological symptoms due to intracranial mass effects since hormonal inactivity leads to a delay in diagnosis compared with functioning pituitary adenomas6). It has been reported that 96.5% of nonfunctioning adenomas present as macroadenomas and that 67.8% of patients with these tumors experience visual defects10). For nonfunctioning pituitary adenomas, neurosurgery is the treatment of choice20,35).
Functioning pituitary adenomas that secrete prolactin account for 40 to 60% of pituitary adenomas. Treatment of these tumors can be begun with a dopamine-agonist such as bromocriptine. Surgical resection, usually with the trans-sphenoidal approach, should be considered for pituitary adenomasthat secrete prolactin and show rapid deterioration in visual function as well as adenomas that secrete adrenocorticotropic hormone, growth hormone, or thyroid-stimulating hormone. When medical and sur-gical treatments are unsuccessful, radiotherapy may be used post-operatively35).
The principal neurological criterion on which surgical management decisions are often based is deterioration of visual fields24). A relationship exists between severity of visual impairment and tumor size36). However, there are few data currently available to provide a more quantitative correlation between adenoma size and severity of visual impairment. The aim of this study was to investigate the quantitative relationship between pituitary macroadenoma size and degree of visual impairment. Improvement in vision after surgical resection was also evaluated.
MATERIALS AND METHODS
The medical records of patients with pituitary adenoma who were treated with trans-sphenoidal adenectomy (TSA) between January 2009 and January 2011 were reviewed retrospectively.
The inclusion criteria were the following : 1) received TSA for pituitary adenoma and with follow-up more than 6 months; 2) underwent regular follow-up in the neurosurgery and ophthalmology departments of Kaohsiung Chang Gung Memorial Hospital; 3) underwent complete ophthalmologic examination including best-corrected visual acuity (BCVA), slit-lamp biomicros-copy, intraocular pressure, dilated fundus examination, and visual field (VF) test before and 6 months after surgery; 4) underwent brain MRI before and after surgery; 5) pituitary adenoma with vertical size >1 cm as determined by MRI images. Vertical size was measured using contrast-enhanced T1-weighted coronal image and defined as the height from the lowest portion of the tumor to the top of the tumor. Giant pituitary adenoma was defined as a tumor with a maximum diameter measuring ≥40 mm.
Patients were excluded if they had ophthalmologic disorders or other intracranial lesions that might affect the results of the BCVA and VF tests, recurrence of pituitary tumor after surgery, or VF test results or MRI images of poor or unreliable quality.
In order to measure the size of the adenoma, the maximum optic chiasm displacement, and the direction of adenoma expansion, high resolution MRI series images with contrast were obtained. Because the shape of the adenoma could be irregular, only the vertical dimension of the adenoma was used to define the size. Regarding the distance that the optic chiasm moved from its original position due to growth of the adenoma, the method proposed by Ikeda and Yoshimoto18) in 1995 was utilized. In this method, two reference lines are drawn to help calculate the distance between the observed optic chiasm and its original position. One reference line is drawn between the frontal base and the posterior clinoid process on the sagittal image, and the other reference line is drawn at the upper surface of the bilateral internal carotid artery on the coronal image. Then, the maximum distance between the reference line and the lower surface of the optic chiasm is measured on each image. Recognizing the direction that the adenoma expands is more straightforward since it is determined on MRI images using the naked eye. There are three different directions in which adenomas tend to expand : the suprasellar area, infrasellar area, and parasellar area/cavernous sinus.
A VF test was to be performed by Goldmann perimetry within a week before TSA was carried out2). In this study, I-4e stimulus (size : 1/4 mm2, brightness : 0 dB) and II-4e stimulus (size : 1 mm2, brightness : 0 dB) were used to determine the VF defect. The Snellen visual acuity chart, placed 6 m (20 feet) from the patient, was used to measure BCVA. Conversions from the Snellen fraction to the minimum angle of resolution or recognition and the decimal notation were obtained37).
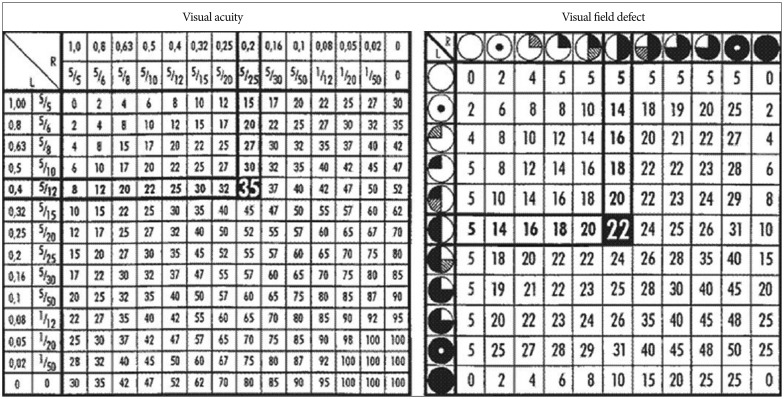
Visual impairment score (VIS) developed by the German Ophthalmological Society was calculated by adding the scores of the tables for assessing BCVA and the VF defects; each table combined the findings for both eyes (Fig. 1)19,29). This method was originally used by Fahlbusch and Schott9) to analyze the visual status and surgical outcome of patients with tuberculum sellae and planum spenoidale meningioma. According to the scores obtained (ranging from 0 to 100), visual impairment could be further divided into the following four grades :
The correlation between preoperative VIS/postoperative VIS and other variables (age/sex/the vertical size of tumor/parasellar invasion of tumor/tumor type/the position of the optic chiasm/optic atrophy) was then evaluated.
Statistical analysis
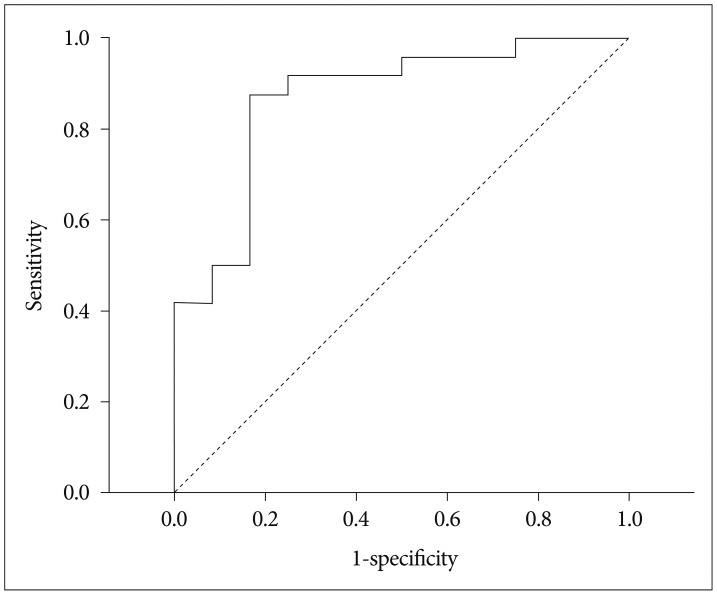
The patients' demographics and characteristics were presented as mean±standard deviations (SDs) for continuous variables and n (%) for categorical variables. Differences in continuous variables among pituitary adenoma types were compared using the Kruskall-Wallis test and Mann-Whitney U test for pair-wise comparisons because the data were not normally distributed; differences in categorical variables among pituitary adenoma types was compared using Fisher's exact test due to limited cell numbers being less than five. Dispersion of pre-operative (Pre-OP) and post-operative (Post-OP) grade of VIS by patients' pituitary adenomas were graphed as a bar as percentage of VIS grade. For the ordinal data of VIS grade, difference in VIS grade between Pre-OP and Post-OP for a given type of pituitary adenoma was compared using the Wilcoxon signed ranks test; difference in VIS grade for pairwise comparison among pituitary adenomas was performed using the Mann-Whitney U test for Pre-OP and Post-OP, respectively. All statistical assessments were two-tailed and considered significant at p<0.05. An adjusted p=0.0167 (p=0.05/3) was also considered for the pair-wise comparisons. Statistical analyses were performed using SPSS 15.0 statistics software (SPSS Inc., Chicago, IL, USA). Patients with macroadenomas (>1 cm to ≤4 cm) were divided into two groups according to the tumor size cut-off for determined via receiver operating characteristic curve based on the maximization of the Youden's index rounded to the nearest whole number. The Youden's index, equal to the sum of sensitivity and specificity minus one, is used for calculating optimal thresholds on medical tests11).
RESULTS
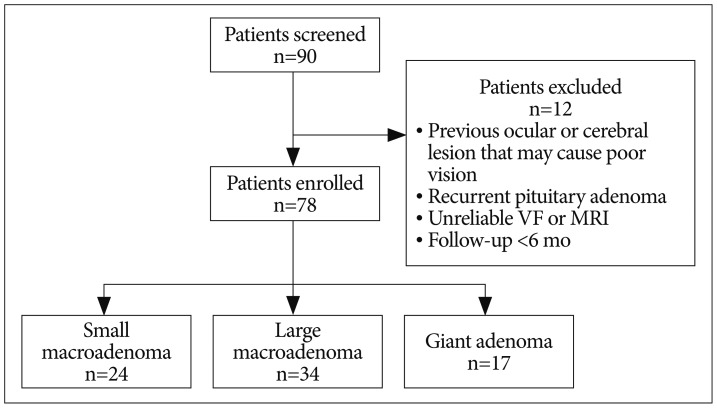
A total of 78 patients (37 females and 41 males) with a mean age of 47.1 years were included. Patients with macroadenomas (>1 cm to ≤4 cm) were divided into two groups according to the cut-off tumor size of 2 cm (Fig. 2). Among the 78 patients, 24 had small macroadenoma (>1 cm to ≤2 cm), 37 had large macroadenoma (>2 cm to ≤4 cm), and 17 had giant adenoma (>4 cm) (Fig. 3). One male patient with a giant adenoma but without suprasellar extension was included in the study because the patient did not meet the exclusion criteria. This patient's tumor had a vertical size of 5.5 cm but the optic chiasm displacement was only 1.05 cm in the sagittal view and 1.13 cm in the coronal view which is even less than the average optic chiasm displacement of the large macroadenoma group (1.3 cm and 1.7 cm, respectively). This patient had a preoperative VIS of 17 and postoperative VIS of 0.
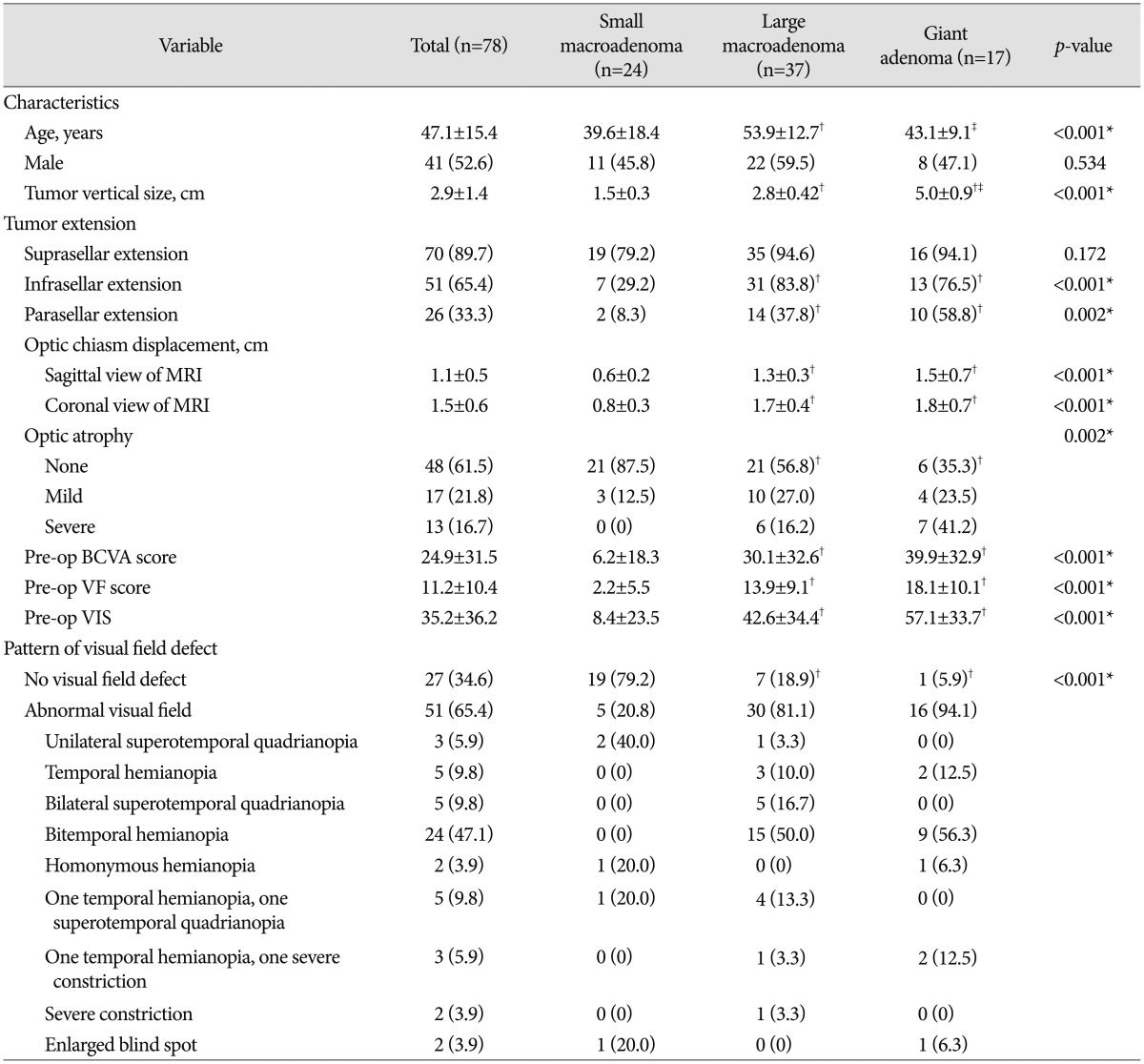
Table 1 shows the subjects' baseline demographics and clinical characteristics categorized by preoperative pituitary adenoma size. The baseline demographics and clinical characteristics were significantly different among pituitary adenoma sizes with regard to age, vertical size, tumor type, initial symptom, infrasellar extension, parasellar extension, chiasm displacement, optic atrophy, pre-operative BVCA and VF scores and VIS (all p<0.05) (Table 1).
Regarding the visual field defect pattern, patients with large macroadenoma and giant adenoma had a higher rate of abnormal visual field than patients with small macroadenoma (small macroadenoma : 20.8%, large macroadenoma : 81.1%, giant adenoma : 94.1%; p<0.001). Among the patients with abnormal visual field defect, the most frequent pattern that occurred was bilateral bitemporal hemianopia, especially for the patients with large macroadenoma and giant adenoma (small macroadenoma : 0%, large macroadenoma : 50%, giant adenoma : 56.3%) (Table 1).
The data for extent of resection are presented in Table 2. A significantly smaller proportion of patients with giant adenoma had total resection compared with patients with small macroadenoma (p<0.0167), Table 2 also shows the duration of follow-up for each group. There was a significant difference in duration of follow-up (p<0.05) among the groups.
Table 3 summarizes the improvement in BVCA score, VF score, VIS, and recurrence rate of pituitary adenoma postoperatively. The BVCA score from pre-operation to post-operation decreased in small macroadenoma, large macroadenoma, and giant adenoma patients by 0.5, 15.8, and 27.0, respectively (p<0.01). The VF score from pre-operation to post-operation in small macroadenoma, large macroadenoma, and giant adenoma patients decreased by 0.5, 7.9, 7.7, respectively (p<0.01). The visual improvement score from pre-operation to post-operation decreased by 1.0, 23.5, and 33.3 in small macroadenoma, large macroadenoma, and giant adenoma patients, respectively (p<0.001). The improvement of VIS post-operatively in large macroadenoma and giant adenoma patients was significantly better than that in small macroadenoma patients (both p<0.0167). However, there was no significant difference between large macroadenoma and giant adenoma patients (Table 3).
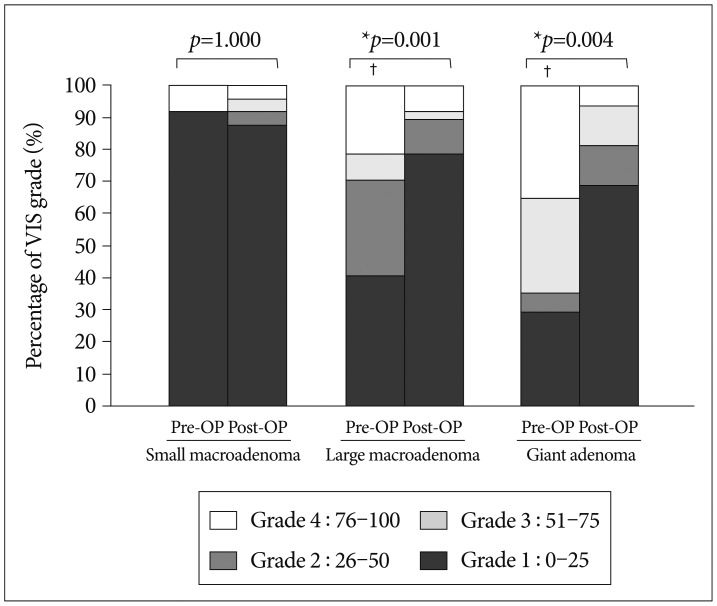
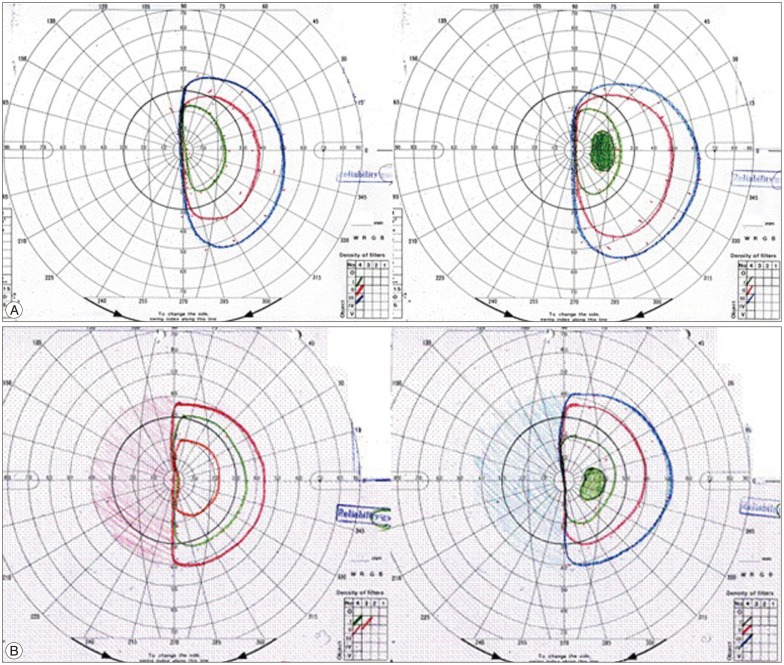
The preoperative and postoperative percentages of VIS grade for patients are also presented by types of pituitary adenoma in Fig. 4. The VIS grade was stratified as four levels : grade 1 (VIS : 0-25), grade 2 (VIS : 26-50), grade 3 (VIS : 51-75), grade 4 (VIS : 76-100). Similarly as is shown for VIS in Table 2, the preoperative dispersion of VIS grade either in large macroadenoma or in giant adenoma were both different than in small marcoadenoma (both p<0.0167). Furthermore, there was no significant difference in postoperative VIS grade among the three sizes of pituitary adenoma. In addition, the postoperative VIS grade of patients with either large macroadenoma or giant adenoma improv-ed with respect to preoperative VIS grade (both p<0.05) (Fig. 4). Fig. 5 show examples from individual cases of pre-operative and post-operative VF defects.
With regard to postoperative adenoma recurrence, the patients with either small macroadenoma or large macroadenoma had a higher recurrence rate than those with giant adenoma (small macroadenoma : 91.7%, large macroadenoma : 89.2%, giant adenoma : 52.9%; p=0.003) (Table 3).
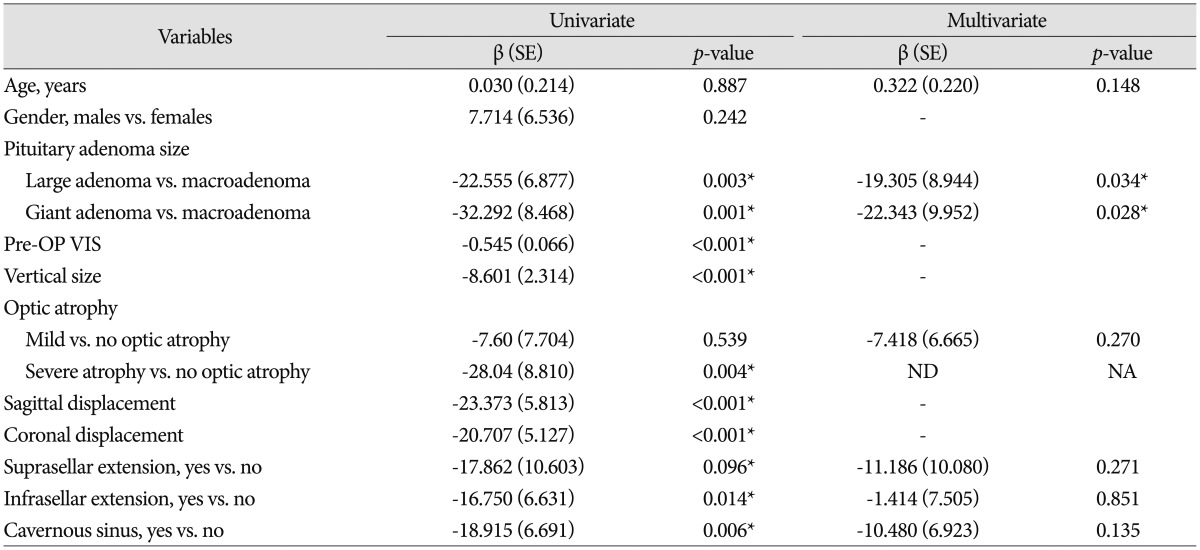
The results of univariate and multivariate analysis to identify factors that influence VIS improvement are shown in Table 4. Univariate analysis indicated that improvement in VIS might be influenced by pituitary adenoma size, preoperative VIS, vertical size, severe optic atrophy, sagittal displacement, coronal displacement, suprasellar extension, infrasellar extension, and cavernous sinus. Variables with a significance level of p<0.02 were selected for multivariate analysis, The results of multivariate analysis showed that the only factor that independently influenced VIS improvement was increasing pituitary adenoma size which was significantly related to decreased VIS improvement.
DISCUSSION
Pituitary adenomas are usually classified into microadenomas, macroadenomas, and giant adenomas according to their size13,15,16,22). The larger the pituitary adenoma is, the higher is the risk of optic chiasm or optic nerve compression1,7,17). In general, the size of macroadenomas range from 1 to 4 cm. Smaller macroadenomas typically will not result in any visual field defect or visual impairment, whereas the larger ones will usually cause severe visual disability. From what is known so far, there has been no research that 1) investigated the relation between the severity of the visual impairment and the different sizes of macroadenomas, and 2) has subdivided macroadenomas into 2 groups on the basis of the degree of visual involvement. Our study clearly indicated that pituitary adenomas less than 2 cm usually have no or only a minimal effect on the visual pathway. Thus, to emphasize which tumors are a threat the macroadenomas between 1 and 4 cm were further subdivided into 2 groups : 1) "small macroadenomas"-tumors with less than 2 cm in size, and 2) "large macroadenomas"-tumors ranging from 2 to 4 cm.
The typical visual field defect, bitemporal hemianopia, is due to the anatomical compression of the optic chiasm, which contains the crossing nasal fibers of each optic nerve26). Nevertheless, the visual field defect actually depends on the relation between the optic chiasm and the tumor itself. If the tumor is anterior to the optic chiasm or if the patient has an anatomical post-fixed chiasm, conditions such as central scotoma, arcuate scotoma, and monocular visual constriction can be noted. If the tumor compresses the optic tracts or the patient has a pre-fixed chiasm, a homonymous hemianopia may be seen12,30,33). In our report, 2 patients presented with left homonymous hemianopia before TSA. The tumor size was 2 cm (small macroadenoma) in one patient and 7.05 cm (giant macroadenoma) in the other. The MRI images revealed that the patient with a small macroadenoma had a pre-fixed optic chiasm, and the patient with a giant macroadenoma had a right temporal base extension.
We found that large macroadenomas and giant adenomas leading to visual impairment are mostly nonfunctioning adenomas (97.8%). This result is consistent with previous reports1,14,25), and can be explained by the absence of endocrine symptoms, which often result in a delay of the diagnosis since there are no visual symptoms1). This explanation is consistent with what Monteiro et al.27) have mentioned previously that nonfunctioning and prolactin-secreting adenomas are the most likely pituitary tumors associated with visual impairment.
Recent studies have revealed a relationship between the size of pituitary adenoma and VF defects. These studies clearly illustrated that patients with larger tumors tended to have VF abnormality, and that the severity of VF defects is closely related to tumor size24,33,27). Lee et al.23) also proved that there is a close correlation between VF defects and 3-dimensional tumor volume which has a significantly positive correlation with pattern SD (standard pattern deviation) of Humphrey perimetry. Generally speaking, larger volume tumors will usually result in a higher risk of compression at the optic chiasm; however, this relationship is not found when tumor extension mainly occurs at the infrasellar or parasellar region instead of the suprasellar region. In fact, we found that if the adenoma grows in the vertical direction, it will usually result in more severe visual impairment. If the adenoma grows in the horizontal direction, it will usually cause less vision damage, but there is a greater chance of adenoma recurrence3,34). This is because horizontal growth of the adenoma may invade the cavernous sinus which makes it difficult for the surgeon to completely remove the tumor. Therefore, only the vertical size of adenomas was investigated in this study.
Some of the previous studies have already discussed the relationship between the optic chiasm position and visual loss. Ikeda and Yoshimoto18) found that visual impairment occurred when the displacement of the optic chiasm was more than 8 mm above the reference line on the sagittal image and more than 13 mm above on the coronal image on brain MRI. Monteiro et al.27) have also shown that tumor exceeding 10 mm above the sagittal standard line and 12 mm above the coronal standard line had a significant effect on visual loss. The findings of these studies are similar to what was found in this study, which showed that significant visual impairment (VIS grade ≥2) occurred when the optic chiasm was moved by the tumor more than 11.2 mm above the reference line on the sagittal view and more than 15.3 mm on the coronal image.
With regard to visual improvement after surgery, there were 47 cases in total, and 13 out of the 47 patients (27.67%) had a complete recovery. Visual improvement occurred in 88.7% (47 of 53 patients) of patients. Previous series have reported that visual improvement depends on the surgical approach, ranging from 74.7-93.4%28,29,39,40). In this study, patients with large macroadenomas or giant adenomas experienced greater visual improvement after surgical resection compared with patients who had micro- or small macroadenomas, but patients with smaller pituitary adenomas still had a better visual outcome. Gnanalingham et al.'s14) findings were comparable. They believed that better preoperative visual acuity and a smaller degree of impairment in preoperative VF would have a better effect on the visual outcome.
There have been contradictory results in previous studies regarding predictive factors for recovery of vision. Müslüman et al.29) found that tumor size was not significantly associated with the postoperative visual impairment score but preoperative visual deficit and the time interval between the initial visual symptom and surgery were significantly associated with the postoperative visual impairment score. A shorter duration of symptoms, younger age, and a better preoperative BCVA have been reported to be associated with better postoperative recovery of VF by some investigators5,14) but not others31,32). The reason for this inconsistency is not clear, but the difference between previous data and our study could be due to different parameters in studied patients, such as the differences in preoperative BCVA and VF defect. Also, the extent of surgical resection can also be an important factor. The greater the extent of resection of large macroadenomas and giant adenomas, the better the visual outcome.
Undoubtedly, vision can rapidly improve within minutes or days after tumor resection21). Among all surgical resection procedures, TSA is likely the most effective for providing rapid relief of visual symptoms in patients with a pituitary adenoma4,38). Thus, early surgical resection of the tumor should be considered for patients with a large or giant macroadenoma causing visual loss in order to preserve their vision.
CONCLUSION
Results from this study show that pituitary adenomas larger than 2 cm cause defects in vision while adenomas 2 cm or smaller do not cause significant visual impairment. Trans-sphenoidal adenectomy in patients with large macroadenomas and giant adenomas resulted in immediate and significant improvements in vision. However, the final visual outcome in patients with these larger adenomas was poorer than that of patients with adenomas 2 cm or smaller in size. These results suggest that patients with pituitary adenomas larger than 2 cm should undergo prompt surgical resection to prevent further vision loss and to improve post-operative vision outcome.


 XML Download
XML Download