

 PDF
PDF ePub
ePub Citation
Citation Print
Print


treatINTRODUCTION
Congenital dermal sinus (CDS) is a congenital anomaly that develops anywhere in the midline along the neuraxis1). CDS belongs to a group of disorder called occult spinal dysraphism in which skin covers most of the defect of the neuraxis and overlying tissues, except for a small skin ostium of the dermal sinus tract. In the lumbosacral area, the skin ostium of the dermal sinus tract is usually situated above the gluteal folds, which is an important clue for differentiating it from benign sacrococcygeal dimples2).
CDS is a very uncommon disease. However, the clinical importance of CDS is that some patients with the anomaly can develop severe infection of the central nervous system, such as bacterial meningitis and spinal cord abscesses, through the dermal sinus tract3). Therefore, pediatricians should be alert for the possibility of CDS when examining a dimple in the midline of scalp and back. Overlooking CDS or misdiagnosing the anomaly as a benign sacrococcygeal dimple may lead to a catastrophic infection and cause serious neurological deficits4).
We encountered a 12-month-old girl who presented with a pyomyelia in the whole spinal cord. Further evaluation showed a small skin ostium in the upper sacral area and a CDS leading into the spinal canal. Unfortunately, a detailed history report revealed that the skin ostium was detected early in her neonatal period by the parents, but they thought it was a benign skin lesion with little clinical importance. Despite surgical evacuation of the abscess and infection control, the patient showed grave neurological deficits. This case emphasizes the crucial importance of gaining knowledge of and directing clinical attention to differentiating a potentially life-threatening anomaly from benign lesions, and primary physicians are urged to be vigilant in understanding and diagnosing CDS.
CASE REPORT
A 12-month-old girl visited the emergency room with a high fever and progressive paraparesis. The patient had normal development and began to walk at approximately 10 months of age. She had developed a fever of up to 39.5℃ 15 days prior to the visit. While visiting a local clinic, she was diagnosed with pharyngitis and received antibiotics and antipyretics. Her fever subsided but repetitive vomiting started 10 days prior. Five days ago, her high fever returned again. From then, she intermittently showed lethargic symptoms and was unwilling to walk. She received additional examinations for infectious disease and supportive treatment for days, and finally, the local physician decided to transfer her to our hospital, when she showed overt paraparesis.
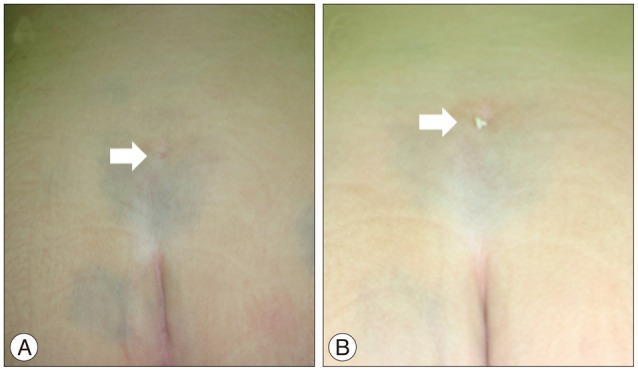
Upon arrival at the emergency room, she was acutely ill-looking and lethargic. Her vital signs were as follows : heart rate 137 beats/min; blood pressure 123/56 mm Hg; respiratory rate 28 breaths/min; body temperature 38.6℃. She was alert but exhibited quadriparesis. Her motor grade was I/I for upper extremities and 0/0 for lower extremities. She also exhibited profound hypesthesia below the C4 dermatome. Bilateral biceps jerks were weak, and bilateral knee and ankle jerks were absent. No meningeal irritation sign was observed. A palpable mass was found in her abdomen, which was determined to be a distended bladder. There was a tiny dimple in the midline of the upper sacral area (Fig. 1). It was located above the gluteal folds, approximately 6 cm away from the anus. A small amount of whitish thick discharge was squeezed from the dimple by manual pressure. A laboratory examination revealed blood leukocytosis (15500/µL), decreased hemoglobin (10.9 g/dL), decreased hematocrit (31.6%), and elevated C-reactive protein (5.83 mg/dL).
The febrile illness and rapidly ascending quadriparesis indicated an infectious disease of the central nervous system involving the spinal cord. The high-lying midline skin dimple with discharge added suspicion of an underlying infected dermoid. A detailed history was collected and revealed that her parents had found the skin dimple during her neonatal period, but they thought it was an innocent lesion that did not require further investigation.
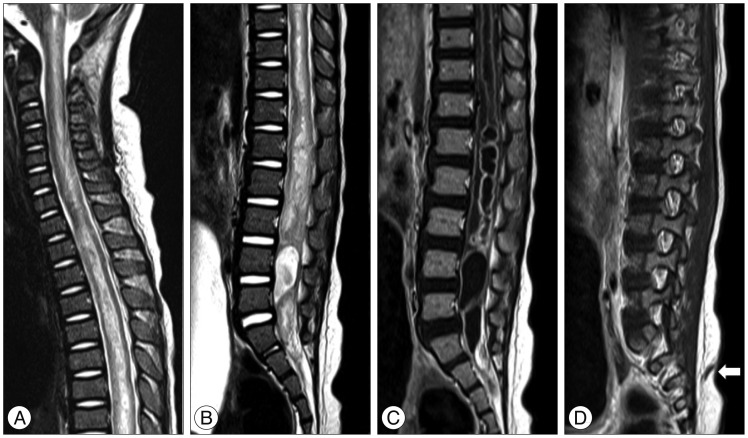
Spinal magnetic resonance imaging (MRI) was immediately obtained (Fig. 2). The MRI revealed diffuse high signal intensity along the spinal cord up to the medulla oblongata. There was a low-lying conus down to the S3 level. An enlarged central canal and thick gadolinium-enhancement of the lining up to the T1 level was observed. There were multiple cystic dilatations with rim enhancement in the lumbosacral cord. A dermal sinus tract ran obliquely upward from the conus at the S3 level to the skin. An infected CDS with massive holocord pyomyelia was diagnosed.
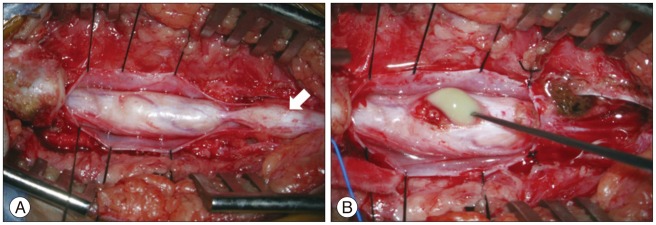
An emergency operation for abscess evacuation and untethering was performed. The sinus tract was followed from the skin ostium. There were multiple dermoid cysts along the sinus tract entering the dural sac through the fascial and bone defect (Fig. 3). After a multi-level laminectomy, the dural sac was opened and a thickened spinal cord was observed. A dorsal midline myelotomy was made and noxious green-colored pus was discharged from the abscess. The abscess cavity and syrinx were flushed with saline. Finally, the sinus tract was resected just distal to the last root.
Multiple pathogens were suspected and the patient received vancomycin and cefotaxime for empirical therapy. Later, Peptoniphilus asaccharolyticus and an unidentified anaerobic rod were isolated from the pus and we added metronidazole to the drug regimen. She received the triple antibiotics for 6 weeks following the operation. Her fever subsided quickly, but profound neurological deficits remained. The lower extremity weakness improved only slightly, and spasticity ensued. She had weakness in both hands (C8-T1 level). Horner syndrome in the left side with ptosis and anhydrosis of face was observed. Sensory function in the trunk and lower extremities improved slightly but incompletely. She had a neurogenic bladder and clean intermittent catheterization (CIC) was required. She was followed post-surgery for 2 years. Serial spinal MRIs showed gradual shrinkage of the residual T2 high signal intensity and enhancement in the spinal cord. In this time period, she never developed another bout of the febrile episode. She regained grasp function in both hands, particularly in the right hand. She can move her legs slightly, but she is still wheelchair-bound and needs CIC for bladder care.
DISCUSSION
CDS is a rarely encountered anomaly in clinical practice. Because of its low incidence rate, many clinical series on CDS include data accumulated over decades1,2). Nonetheless, CDS is an important disorder that is emphasized in pediatric textbooks. The sinus tract can be a potential route of a life-threatening infection to the central nervous system; thus, CDS requires early detection and surgical treatment. Therefore, clinicians should be alert when examining skin dimples in the midline on the back.
One major obstacle to correctly diagnosing CDS is that there exists a benign entity called a sacrococcygeal dimple, and its incidence rate is far higher than that of CDS6). Sacrococcygeal dimples are innocuous lesions located just over the coccygeal area7). They are typically small (<5 mm in width) and are located in the midline in the gluteal folds within 2.5 cm from the anus. It is not accompanied skin stigmata, such as hemangiomas, elevated masses, tails, or hairy patches. Kriss and Desai7) reported that none of the 180 simple dimples satisfying these criteria were associated with occult spinal dysraphism in imaging studies. Atypical dimples located higher on the back, although not pathognomonic of occult spinal dysraphism, are of high risk and warrant further evaluation. Sometimes, whether a skin dimple is benign is not easy to determine by inspection alone6). In such cases, spinal ultrasonography is an easy method for resolving the problem.
In this patient, the skin dimple was clearly located high on the back away from the coccygeal area. Unfortunately, there was a chance to detect the presence of CDS and enough time to prevent the catastrophe. Currently, primary physicians are keen to diagnose hidden anomalies such as occult spinal dysraphism. Knowledge and precautions against such a disorder are common even among the general public. However, erroneous information is still widespread and a decision-making mistake may lead to irreversible damage to the patient4). Ramnarayan et al.10) reported a clinical course of 9 patients with CDS. Interestingly, all the patients were previously examined by medical personnel (family doctor, pediatrician, or general practitioner) and they made no action or gave just empirical treatment with antibiotics before significant neurological deficits or meningitis developed. Inspection of the whole body is a routine for neonates and midlines in the scalp and back should be included in this procedure. For any atypical dimples, further imaging or consultation with a pediatric neurosurgeon is recommended8,9). Elton and Oakes5) further emphasized that surgical exploration is mandatory for dermal sinus tracts located above the gluteal folds.
Spinal intramedullary abscesses are a severe complication of CDS. Among the various septic presentations of CDS, meningitis is the most common and spinal intramedullary abscess is the least common finding3). Prompt surgical drainage of the abscess cavity through a dorsal midline myelotomy is the best choice to control the infection and to enhance functional recovery. In the literature, some patients attained complete recovery of neurological functions, but others had only a partial improvement after surgery11). The outcome may depend on the degree of septic involvement of the spinal cord and the time to diagnosis and surgical intervention. In the series of Ramnarayan et al.10), all patients over the age of 1 year had purulent infection or neurological deficits at presentation, and surgical morbidity paralleled the time interval to definitive treatment. Our patient had partial recovery of neurological deficits after treatment and rehabilitation. A delay in the proper diagnosis from the onset of fever and gait disturbance may prevent optimal recovery despite emergency surgical intervention.
CONCLUSION
Failure to detect a CSD may lead to catastrophic infection in the central nervous system. An early diagnosis and prompt surgical intervention are required before the onset of severe infection. Clinicians should be alert to any atypical-looking skin dimples in the midline of infants and children.
 XML Download
XML Download