

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
We are living in the aging society with rapid increase of the proportion of aged population. Accordingly, geriatric syndrome became an important medicosocial issue recently45). Muscle wasting is one of the main changes of aging human body, which was introduced by Rosenberg79,80) as the term sarcopenia in 1989. The loss of muscle mass is estimated about 8%/decade from 40 to 70 years of age, and then it becomes faster up to 15%/decade35). Sarcopenia has been widely known to be the decreased mass and strength of skeletal muscle by an aging process, but there are still debates in its definition67).
The European Union Geriatric Medicine Society (EUGMS) made a Sarcopenia Working Group, the European Working Group on Sarcopenia in Older People (EWGSOP), in 2009, and reported the European consensus on definition and diagnosis of sarcopenia in 201020). This European consensus seemed to trigger interest and attention for sarcopenia at many countries including Korea. The first annual meeting of Korean Sarcopenia Society was held at 2013. In 2014, the Asian consensus for sarcopenia was reported by the Asian Working Group for Sarcopenia (AWGS)14). There are several well-known operational definitions of sarcopenia based on skeletal muscle mass index (SMI)3,47,70,72), but the definition of EWGSOP combined both the quantitative factor (SMI) and qualitative factors (strength and function)20). The definitions are crucial for not only diagnosis but also treatment strategy of sarcopenia.
Sarcopenia is known to associate with various age related disorders, obesity15), metabolic syndrome83), cardiovascular disease83), osteoporosis23,58), and stroke86). It already became hot topic for clinical and basic researches in the various medical fields like endocrinology, cardiology, rehabilitation medicine, and orthopedics. Most of the researchers are convincing the sarcopenia will make a tremendous and multidirectional impact on medical care system in the near future. But, most of neurosurgeons do not seem to have interests in the muscle condition which may have effects on clinical courses of some neurosurgical diseases.
In this paper, up-to-date information of sarcopenia is introduced with review of literature. The relationship of sarcopenia with neurosurgical disorders and the roles of neurosurgeons are also discussed.
DEFINITION AND DIAGNOSTIC ASSESSMENTS
Sarcopenia can be characterized by progressive loss of SMI and muscle strength with increasing risk of physical disability, poor quality of life, and sometimes death22,34). There are several definitions based on muscle mass. The dual energy X-ray absorptiometry (DXA) and bioelectrical impedance analysis (BIA) can be used for assessing SMI, and magnetic resonance imaging (MRI) and computerized tomography (CT) for muscle cross-sectional area (CSA).
The first reported definition of sarcopenia is based on DXA3). DXA can measure the appendicular SMI (ASM) at the fat free muscle mass of arm and leg96). The definition of sarcopenia with DXA is the reduction of ASM/height2) less than or equal to two standard deviations (SD) comparing to the sex specific mean reference values of a young age (18-40 years) group3).
SMI measured by BIA can be used for definition of sarcopenia. Class I and II sarcopenia are defined as the SMI less than one and two SD comparing to that of the sex specific mean reference value of young age (18-39 years) group, respectively47).
CSA of muscle by MRI or CT is considered to be the most accurate data. The body weight (BW) corrected quadriceps (Qc) muscle CSA (Qc muscle CSA/BW) reflects thigh muscle mass71). Qc Sarcopenia can be defined as the BW corrected Qc muscle CSA more than 1 SD below the mean reference value of younger age (<60 years) group72).
However, the muscle mass itself is not enough for diagnosis of sarcopenia because it is not correlated with its strength34,46). The EWGSOP definition includes SMI and muscle function, requiring
2 or 3 criteria among three diagnostic criteria (low muscle mass, low muscle strength, and low physical performance) for diagnosis
of sarcopenia20). The tools for assessing sarcopenia recommended
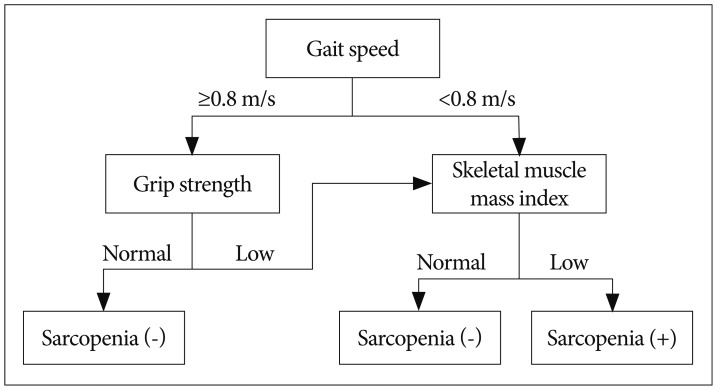
by EWGSOP are CT, MRI, and DXA for muscle mass, grip strength for muscle strength53), and short physical performance battery (SPPB) or gait speed for physical performance36,37,100). SPPB score is total points of three tests, balance, gait speed, and chair stand, scoring between 0-4 for each test with maximum score of 1236). Cut-off points for the three components differ according to the technique used for assessment. The cut-off points for SMI measured with DXA are 7.26 kg/m2 for men and 5.5 kg/m2 for women by Baumgartner method3), 7.23 kg/m2 for men and 5.67 kg/m2 for women by Newman method70), and 7.25 kg/m2 for men and 5.67 kg/m2 for women by Delmonico method22). Cut-off points for the muscle strength are <30 kg for men and <20 kg for women by Laurentani method53) or different muscle strength levels according to BMI introduced by Fried et al.31). Cut-off point for the physical performance is SPPB score ≤8 or gait speed <0.8 m/s37,100). The EWGSOP-suggested diagnostic algorithm is started with the measurement of gait speed for the patient older than 65 years (Fig. 1); 1) With the gait speed >0.8 m/s, no sarcopenia is defined as the grip strength is normal, but SMI should be measured as a final assessment for diagnosis of sarcopenia when the grip strength is subnormal, 2) With the gait speed ≤0.8 m/s, SMI is the next step as a final assessment for diagnosis of sarcopenia.
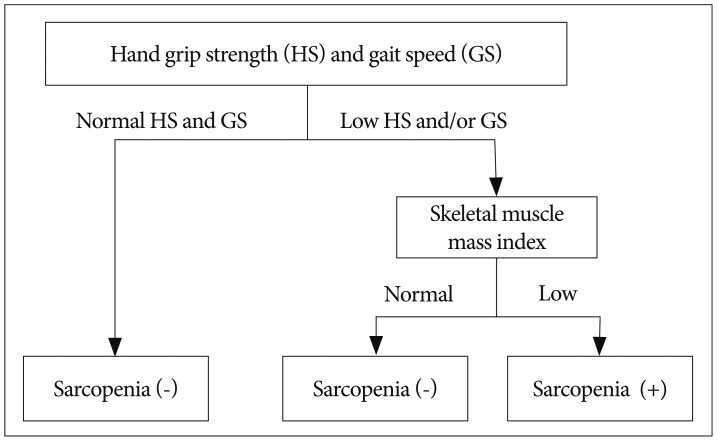
The AWGS recommended cut-off points are SMI <7.0 kg/m2 for men and <5.4 kg/m2 for women by DXA or <7.0 kg/m2 for men and <5.7 kg/m2 for women by BIA, handgrip strength <26 kg for men and <18 kg for women, and gait speed ≤0.8 m/s14). The diagnostic algorithm of AWGS for sarcopenia starts with checking both handgrip strength and gait speed (Fig. 2). When the handgrip strength and/or gait speed less than cut-off points, then muscle mass is measured for diagnosis of sarcopenia14).
Baumgartner et al.3) reported the prevalence of sarcopenia about 13-24% in the older patients (65-70 years) and increased up to 50% in the patients over 80 years of age, and it was higher in male group. Another study reported the prevalence of sarcopenia varies 6-15% in the subjects over 65 years of age with higher prevalence in male group63). Sarcopenia also seemed to increase the rate of disability about 4.1 times and 3.6 times more in male and female groups comparing to the non-sarcopenic patients3).
PATHOPHYSIOLOGY
Classically, skeletal muscle fibers are divided into two types, type 1 and 269). Type 1 fibers are known to be white muscle, fatigue resistant and slow fibers specialized for phasic contraction (e.g., marathon)38). Type 2 fibers are red muscle, faster and stronger than Type 1 fibers specialized for continuous contraction (e.g., weight lifting)38). The fatigue resistance of slow fibers related primarily with the use of oxidative metabolism by Type 1 fibers whereas glycolytic metabolism by Type 2 fibers77). The Type 2 fibers are known to be the primary target for age related muscle atrophy28). Varieties of factors, neurodegeneration, endocrinological environment, inflammatory dysfunction, and obesity have been proposed as the causes of sarcopenia.
The age related decrease in the number of motor neurons in spinal cord52) and peripheral nerve fibers and synaptic vesicles in neuromuscular junction24) had been reported to reduce SMI.
Hormonal factors for maintaining muscular protein metabolism, growth hormone, insulin-like growth factor-1, corticosteroids, androgens, vitamin D, and insulin, are known to decrease with age influencing on SMI negatively25,50,84,85,92,103).
Some pro-inflammatory factors, interleukin-6 (IL-6), plasminogen activator inhibitor 1, and C-reactive protein, were reported to increase in plasma in the elderly people, which is closely related with the age related increase of body fat mass (adipokines)13,42). The low level inflammation by the increased pro-inflammatory factors with wasting of protein and energy seems to have effect on the sarcopenia in the elderly with obesity (sarcopenic obesity)49,87,88). Myokines, myogenic hormone like factors including IL-6, IL-8, IL-15, brain-derived neurotropic factor, and fibroblast growth factor-21, are known to increase during exercise showing protective effect in contrast to the harmful effect of adipokines for skeletal muscle75,76,95). IL-6 and IL-15 secreted from muscles are able to induce lipolysis of fat, so called "muscle-fat crosstalk"76).
Skeletal muscle can be regenerated through activation of satellite cells, undifferentiated mononuclear myogenic cells in skeletal muscles9,61). The satellite cells are known to be the adult stem cells of muscle, which tend to decrease in number and function with age40,74). According to previous reports, aged satellite cells show tendency to differentiate into adipose and fibrotic tissues7,90). Myostatin, a member of transforming growth factor-beta family, can inhibit muscle growth62). Myostatin is thought to inhibit satellite cells proliferation according to previous studies about the relationship between myostatin level and satellite cell population in skeletal muscles12,98). Activin A is known to inhibit muscle growth through binding with type II activin receptor55). Both myostatin and activin A were also reported to inhibit bone mineralization by osteoblast26,27). In contrast to the negative effect of myostatin and activin A on muscle and bone, follistatin can play a role of enhancing muscle growth and bone mineralization by antagonizing both myostatin and activin A26,33). Myostatin and activin A have been observed to increase with age, whereas follistatin did not show correlation with age2,56). The activin A-myostatin-follistatin system means the interactions among the three factors and seems to play an important role in both muscle growth and bone mineralization during aging process6). The terms "muscle-bone interaction" and "muscle-bone cross-talk" are hence proposed according to the concept that skeletal muscle and bone continuously affect and modulate each other's biological properties not only biomechanically but also endocrinologically17,39).
OTHER SYNDROMES RELATED WITH SARCOPENIA
Sarcopenic obesity
Sarcopenic obesity is the imbalance between muscle and fat mass, a combination of decreased SMI and increased visceral fat, in elderly people104). It is closely associated with reduced muscle strength and physical activity, metabolic disorders, and sometimes age related mortality18,82,88,104). In sarcopenic obesity, the decrease physical activity by muscle atrophy results in accumulation of body fat which will increase the levels of pro-inflammatory factors leading to muscle atrophy81,87). In addition, the muscle loss can induce metabolic disorders related with insulin resistance because skeletal muscle is the largest organ response to insulin51,104).
Sarco-osteoporosis and osteosarcopenic obesity
It seems that there are fragility fractures in the patients without osteoporosis according to BMD study or without high fracture risk calculated with World Health Organization fracture assessment tool94,97). The increased fracture risk with age seems to be greater than the age related reduction of BMD48). Recent studies revealed that patients with both osteoporosis and sarcopenia (sarco-osteoprosis) showed greater risk for fracture4,19). Buehring et al.8) reported the prevalences of sarcopenia, osteopenia, and sarco-osteopenia were about 15%, 17%, and 5% of the population with age ≥60 years.
Osteosarcopenic obesity was introduced by Ormsbee et al.73) in 2014 to define the individuals with obesity, low BMD, and sarcopenia. They said the obesity in addition to the pre-existing sarco-osteoporosis would exacerbate the metabolic disorders leading to poor physical function and quality of life. But there are still debates without conclusive diagnostic criteria for osteosarcopenic obesity even though it is one of the top emerging significant public health issues.
Frailty
Fried et al.31) first proposed definition for frailty in 2001 as an age related syndrome including weight loss, exhaustion, weakness of grip strength, slow walking speed, and low physical activity. Recent consensus for frailty definition is "a medical syndrome with multiple causes and contributors that is characterized by diminished strength, endurance and reduced physiologic function that increases an individual's vulnerability for developing increased dependency and/or death", which means sarcopenia combined with fatigue caused by many pathologic conditions68,91).
Cachexia
In 2008, Evans et al.29) introduced new definition of the cachexia, according to the agreement at the cachexia consensus conference, as a complex metabolic syndrome associated with underlying illness and characterized by loss of muscle with or without loss of fat mass. They proposed a multidimensional diagnostic assessment for cachexia including weight loss >5% for one year or BMI <20 with any three components of the followings : fatigue, anorexia, decreased muscle strength, anemia (hemoglobin <12 g/dL), hypoalbuminemia (<3.2 g/dL), or elevated inflammatory markers like IL-6 and C-reactive protein29). The major characteristics of cachexia comparing to sarcopenia are comorbid pathologic conditions (cancer, chronic heart failure, chronic obstructive pulmonary disease, etc.), decreased fat mass, systemic inflammation, increased protein wasting, increased resting energy expenditure, and anorexia89).
MANAGEMENT
Exercise
Most of studies for exercise therapy focused on progressive resistance training (PRT) to improve muscle strength and function rather than aerobic exercise. Yarasheski et al.101) recommended PRT for elderly population (76-92 years), 3 days/week for 3 months. They reported increase of whole body muscle mass about 2.2 kg for men and 1.0 kg for women. Gate speed and muscle strength were also known to be improved with PRT31,59).
Nutrition
Sarcopenic elderly individuals are recommended to intake protein of 1.0-1.5 g/kg/day which is about 15-20% of daily caloric intake5,66). Supplementary Vitamin D (700 IU/day) is recommended for the patients with vitamin D level <100 nmol/L5,66). Creatine monohydrate is also known to helpful for energy storage by increasing availability of phosphocreatine10). Chrusch et al.16) reported creatine supplement with PRT increased muscle mass as well as improved muscle strength.
SARCOPENIA AND NEUROSURGICAL CONDITIONS
Cerebrovascular disease
Motor paralysis induces early changes in muscle tissue by decreased motor nerve signals and reduction of number of motor units1). During chronic phase after stroke, disuse and spasticity can result in muscle atrophy and muscle type shift11). The distribution of muscle fiber types also changes after stroke from type 1 slow twitch muscle fibers to type 2 fast twitch muscle fibers, which is an inverse direction of age related muscle fiber type shift21). The muscle type shift after stroke was reported to affect clinical result negatively by aggravating gait disturbance with decreased walking speed of paralyzed leg21). Malnutrition is a common problem affecting clinical outcome of stroke patients, and it also affect the development of sarcopenia66,102).
Despite the negative influences of sarcopenia on the prognosis of stroke, guidelines for treatment, prevention, and rehabilitation of stroke patients do not indicate any consideration about stroke related sarcopenia32,77). Sarcopenia seems to be overlooked during management of patients after stroke.
Spine
Muscles consist of major portion of spine, but spine surgeons seem to not well understand the nature of muscles around spine comparing to that of bone, joint, or spinal nerves. Osteoporosis is one of the leading problems of spine in the elderly population, and is known to be closely related with sarcopenia through muscle-bone cross-talk17,39). There are strong evidences that muscular atrophy and fat infiltration are the representative age related degenerative changes of muscles54,57,93). Both the atrophy and fatty change of paraspinal muscles are also known to be associated with functional disorders and chronic back pain44,60,64,65). Degenerative lumbar spinal deformities including flat back syndrome and degenerative lumbar kyphosis are also reported to associate with paraspinal muscular atrophy and fatty change43,54).
In spite of many evidences for the relationship between paraspinal muscular atrophy and spinal disorders, there is still lack of concept to link the spinal problems with sarcopenia. The main reason of this mismatch may come from the definition of sarcopenia as a systemic disorder.
CONCLUSIONS
Muscles seem to have been underestimated in relation to the neurosurgical disorders. Even though sarcopenia is not yet listed in the 2014 release of international classification of disease, it must be an essential part of clinical practice and research by neurosurgeons in the near future.
 XML Download
XML Download