

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Posterior cervical screw fixation has been widely used for the correction of cervical spine instability and deformity. Compared to the conventional posterior wiring technique, the fixation method has several advantages such as higher fusion rate, no need of rigid external mobilization, and capability of connection between occipitocervical and cervicothoracic junction and fixation1,2,3,4,9). The fixation with lateral mass screw is relatively safe and easy to insert, but it has small and thin size causing less bony purchase and thus its lower pullout strength can be problematic when applied to C73,6). C7 pedicle screw fixation is known to be the biomechanically strongest method but the pedicle screw is technically difficult to apply due to its small size and critical neurovascular structure of the surrounding area6,15). Recently, C7 intralaminar screw technique has been used as an alternative or salvage technique to the pedicle screw fixation because the method is technically simple and not limited by the position of vertebral artery. And, compared to the pedicle screw, it is significantly superior in all aspects except biomechanically lateral bending range of motion5,6,7). Successful application of bilateral crossing laminar screw technique requires profound knowledge of anatomy for proper positioning of two screws in C7 laminar. To accommodate standard 3.5 mm cervical screw into the bilateral crossing intralaminar screw insertion technique at C7, the following two conditions are required. First, the minimum laminar thickness should be at least 5.5 mm when assuming a tolerance of 1 mm in each side of screw10,12). Second, bilateral two screws should not collide each other at the midline. Accurate screw start point should be selected to satisfy above mentioned conditions in narrow C7 laminar area.
The bilateral crossing laminar screw technique was initially performed in C2 level by Wright14). However, exact same application on C7 does not guarantee the same results because of anatomical differences. Thus, this study aims to determine optimal entry point of the bilateral crossing intralaminar screw insertion by measuring thickness and surface area of various vertical cross-sections of screw entry point (spino-laminar junction). Computed tomography (CT)-based anatomical study has been performed to test feasibility of the C7 intralaminar screws in previous reports, but, there is no cadaveric study focusing on the bilateral crossing C7 intralaminar screw8,11,16). The purpose of this cadaveric study is to provide and establish a guideline of selecting safe entry point of screws for preventing the possibility of screw collision and investigate the usefulness of bilateral crossing laminar screws.
MATERIALS AND METHODS
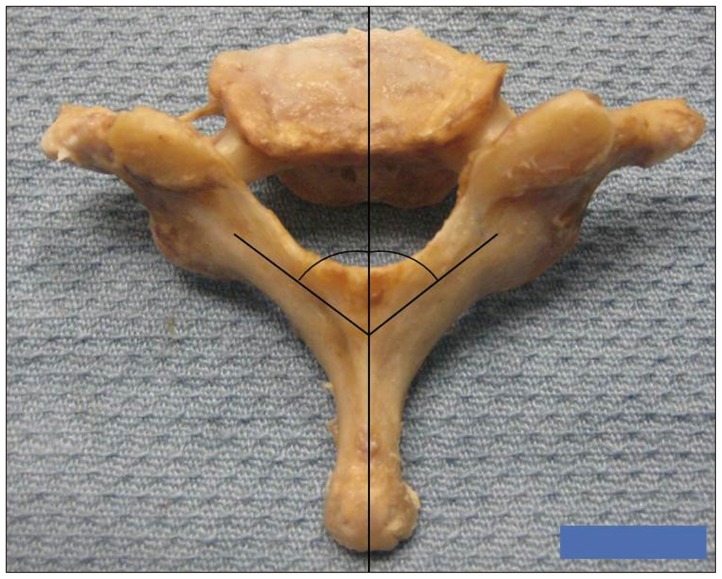
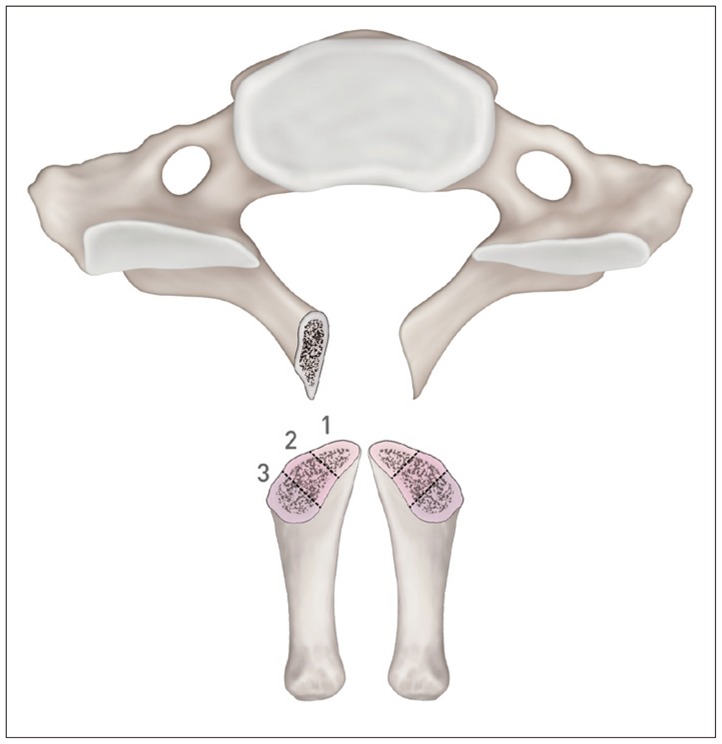
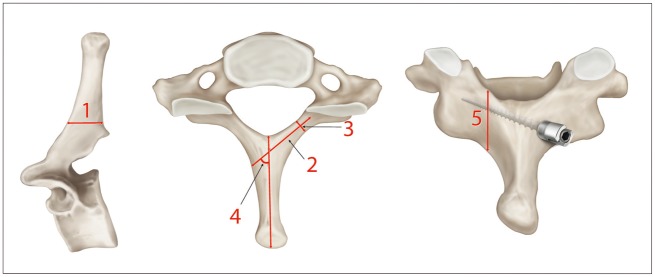
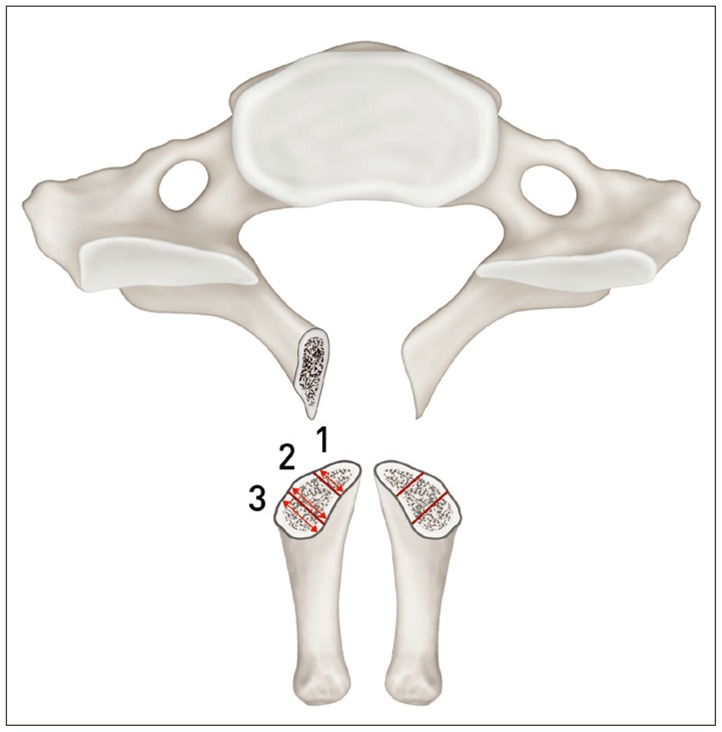
Eighteen fresh cadaver spines from human adult were used for this study. The anatomic specimens were obtained from University of Texas Health Science Center at Houston, Department of Neurosurgery. Demographic information including age and gender was available for each specimen. Donor criteria excluded the subjects with history of rheumatoid disease, spine trauma, infection, tumor or any other bony diseases. Linear measurements were made by an electronic digital caliper (Mitutoyo, Kanagawa, Japan, accuracy 0.1 mm) for all specimens in the following points; height of C7 mid-lamina and C7 lateral mass, minimum laminar thickness, and maximal screw length (the length from the spino-laminar junction to the contralateral lamina-lateral mass junction) (Fig. 1, 2, 3). Digital photographs of all specimens were taken in the axial plane with an appropriate metric scale. The specimens were cross-sectioned bilaterally and vertically at the screw entry point (spino-laminar junction) with electric saw. After then, laminar height was measured at the cross-sectioned plane of screw entry point and the height was equally divided into three parts; upper, middle, lower parts. The maximal laminar thickness of upper 1/3, middle 1/3, and lower 1/3 were measured separately. All measurements were obtained bilaterally and additional digital photographs of the cross-sectioned area were taken. Using Image J software (National Institutes of Health, Bethesda, MD, USA), lateral spino-laminar angle (the angle formed by the C7 spinous process and a line parallel to the longitudinal axis of the C7 lamina) and area of the cross-sectioned surface at the screw entry point were measured (Fig. 4, 5). Statistical analysis using the Student t-test was performed with SPSS software (version 12.0; SPSS Inc., Chicago, IL, USA). Data on sex and laterality (right and left) were compared with anatomic measurement. The values of p<0.05 were considered as statistically significant.
RESULTS
Gross anatomy
The average age of cadaver specimen was 61±10.5 years (47-83 years of range) and the ratio of male : female was 10 : 8. The mean maximal screw length on the right and left was 24.3±1.1 mm (range 22.8-26.5 mm) and 24.8±2.0 mm (range 23.0-29.0 mm), respectively. The mean bilateral maximal screw length was 24.6±1.6 mm (range 22.8-29.0 mm). The mean minimal laminar thickness on the right and left was 6.6±1.2 mm (range 4.0-7.4 mm) and 6.7±1.2 mm (range 5.3-7.9 mm), respectively. The mean bilateral minimal laminar thickness was 6.6±1.2 mm (range 4.0-7.9 mm). Assuming that 1 mm tolerance margin is needed on each side, 4 specimens (4/18, 22.2%) and 6 laminas (6/36, 16.7%) were found to be not applicable for 3.5 mm screw insertion (minimum laminar thickness is smaller than 5.5 mm). In the midline area where two of 3.5 mm screws might cross (3.5×2+2 mm=9 mm), the mid-laminar height was over 9 mm in all specimens and the mean mid-laminar height was 13.7±2.5 mm (range 11.05-18.22 mm). The mean spino-laminar angle on the right and left was 52.1±3.1° (range 47.4-57.2°) and 49.5±5.5° (range 43.2-60.6°), respectively. The mean bilateral spino-laminar angle was 50.8±4.7° (range 43.2-60.6°). At the screw entry point, the mean laminar height on the right and left was 16.6±1.6 mm (range 14.7-19.0 mm) and 16.9±1.5 mm (range 15.3-19.5 mm), respectively. The mean lateral laminar height at the screw entry point was 16.8±1.6 mm (range 14.7-19.5 mm) (Table 1, Fig. 6).
Cross sectional anatomy
After vertical cross-sectioning of spino-laminar junction, lamina height was equally divided into 3 parts (upper, middle, and lower) and maximal thickness and surface area of each portion were measured bilaterally. The mean maximal thickness of upper, middle, and lower parts at the spino-laminar juction on the right side was 4.7±1.2 mm (range 3.1-6.8 mm), 7.2±2.0 mm (range 4.3-11.0 mm), and 6.9±1.6 mm (range 4.2-9.9 mm), respectively. The mean maximal thickness of upper, middle, and lower parts at the spino-laminar juction on the left side was measured at 5.3±1.1 mm (range 3.6-7.6 mm), 7.9±2.0 mm (range 4.2-11.1 mm) and 7.7±2.0 mm (range 4.1-11.1 mm), respectively. The mean bilateral maximal thickness of upper, middle and lower parts at the spino-laminar juction was 5.0±1.2 mm (range 3.1-7.6 mm), 7.5±2.0 mm (range 4.2-11.0 mm) and 7.3±1.8 mm (range 4.1-11.1 mm), respectively (Table 2, Fig. 7). The mean surface area of upper, middle, and lower thirds at spino-laminar juction on the right side was 21.6±9.4 mm2 (range 7.8-33 mm2), 45.9±20.0 mm2 (range 22.3-84.8 mm2), and 31.5±10.6 mm2 (range 14.9-50.4 mm2), respectively. The mean surface area of upper, middle, and lower parts at the spino-laminar juction on the left side was 20.8±7.0 mm2 (range 9.6-33.6 mm2), 47.7±13.0 mm2 (range 26.3-67.6 mm2), and 38.0±13.1 mm2 (range 19.4-60.9 mm2), respectively. The mean bilateral surface area of upper, middle, and lower parts at the spino-laminar juction was 21.2±8.3 mm2 (range 7.8-33.6 mm2), 46.8±16.9 mm2 (range 22.3-84.8 mm2), and 34.7±12.4 mm2 (range 14.9-60.9 mm2), respectively (Table 3). In most cases, the screw entry point started at spino-lamina junction and vertical cross-section of the part showed various morphologies of C7 laminae. When upper thirds lamina was the start point, only 12 laminae out of 36 (33.3%) was thicker than 5.5 mm. For middle and lower thirds, 30 (83.3%) and 32 (88.9%) laminae were thicker than 5.5 mm, respectively. In surface area of the cross-sectional area, the area passing by 3.5 mm screw is 9.6 (1.75×1.75×3.14) mm2. Considering 1 mm tolerance margin on each side of screw, 23.7 (2.75×2.75×3.14) mm2 is thought to be enough surface area for placing screw. For screw entry point, 14 (38.9%), 32 (88.9%), and 28 (77.8%) sides laminae satisfied the condition in upper, middle and lower thirds lamina, respectively (Table 2, 3).
DISCUSSION
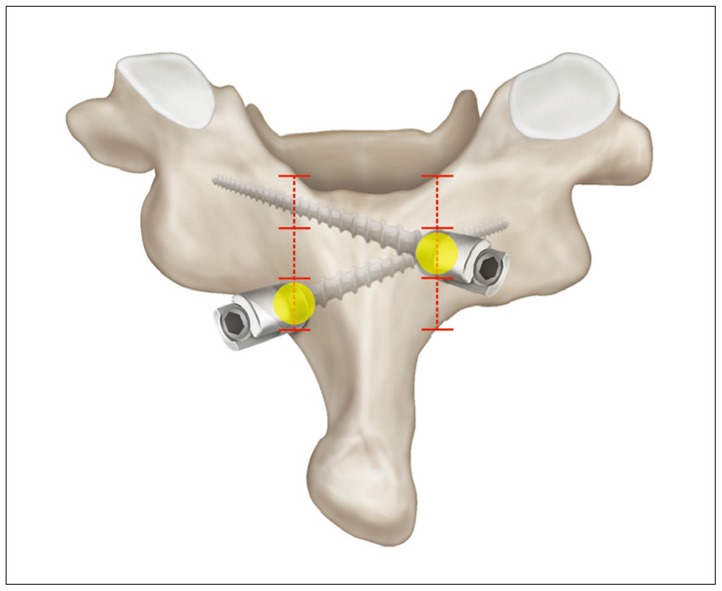
The C7 intralaminar screw technique reported by Hong et al.5) at 2008 has some advantages such as eliminating the risk of injury to neurovascular structures. When the vertebral artery courses into C7 transverse foramen, the C7 pedicle screw insertion can induce injury of adjacent vertebral artery or spinal cord. The use of intralaminar screws allows immobilization of the C7 without risk of the vertebral artery injury. Another important advantage of the intralaminar screw fixation is that the screw can be placed and directly seen at outer cortex of lamina and all relevant structures without use of fluoroscope or navigation system13). In biomechanical aspect, the strongest C7 fixation method is the application of pedicle screw. C7 intralaminar screw is not significantly different from the C7 pedicle screw fixation in flexion/extension, axial rotation and pull-out strength even though it is inferior in lateral bending6). Thus, the C7 intralaminar screw insertion has been used as an alternative or salvage technique recently when C7 pedicle screw insertion is not possible or failed because of small pedicle size of C7 or vertebral artery coursing through the C7 transverse foramen. The advantages of the C7 intralaminar screw insertion leaded several CT-based anatomic studies of C7 and resulted in the advances of the technique8,11,16). However, if the screw is too long, it can possibly induce facet joint or cervical nerve root injury. Especially if it penetrates ventral surface of lamina, spinal cord injury can occur. Also, two screws can collide each other in case of bilateral screw insertion. Identification of accurate screw entry start point can reduce possible complications. Therefore, our anatomic study focused on the intralaminar screw entry point and laminar anatomy for application of bilateral crossing intralaminar screw. In our test results, mean laminar thickness, maximal screw length, and spino-laminar angle of C7 were 6.6 mm, 24.6 mm, and 50.8°, respectively, which were comparable to other CT-based study11,12,13). The lamina cross-section results at spino-laminar junction showed that the junction between midlle and inferior thirds has the thickest laminar. This result suggests that the junction between middle and inferior thirds at the spino-laminar junction can be the screw entry point for unilateral intralamina screw5). But for bilateral crossing intralaminar screw, two screws can collide each other at the midline when both lamina takes the same screw start point. The bilateral crossing laminar screw at C2 level was reported initially by Wright14). In this study, one screw entry point was generated close to the rostal margin of lamina and another point was made at the caudal margin of lamina to prevent collision of two screws. The same application on C7 might not be successful due to the anatomical difference between C2 and C7. When the thickest part was measured, thickness and surface area of upper thirds of C7 lamina were 5.0 mm and 21.2 mm2, respectively, indicating that about 35% of spino-laminar junction was available for 3.5 mm screw insertion. Therefore, selection of the screw entry point for C7 should be different from the one for C2 level. The cross-sectional anatomy of C7 showed that the thickness of middle and lower thirds of spino-laminar junction was 7.5 mm, 7.3 mm, respectively. The surface area of middle and lower thirds of spino-laminar junction was 48.6 mm2, 34.7 mm2, respectively, suggesting that around 85% is available for 3.5 mm screw insertion. Thus, lower two thirds would be better choice for the screw start point to reduce the collision possibility of two screws for bilateral screw insertion (Fig. 8). This technique is not applicable on laminar fracture and lateral connector is required for the connection between upper/lower level and rod. Another important concern for the cervical laminar screw fixation is that decortication of the lamina for increasing fusion bed can expose the laminar screw and reduce bone purchase of the screw. But compared with C2, C7 has much larger bone graft surface and transverse process. Therefore, it is not necessary to decorticate the C7 lamina to enhance fusion7).
CONCLUSION
The intralaminar screw insertion in C7 level has been used as an alternative or salvage technique to the use of pedicle screw. This technique is relatively safe and easy, but precise anatomic knowledge is required for safe insertion of bilateral crossing C7 intralaminar screws into narrow laminar space. Selection of proper screw entry point is the best way to reduce complications such as collision of two screws and violation of laminar cortex. The level of laminar thickness was the highest in middle thirds of C7 screw entry point cross-section and around 77% was available for 3.5 mm screw insertion when lower thirds was chosen for the screw entry point. For bilateral crossing laminar screw insertion, middle and lower thirds of spino-laminar junction can be chosen for each side, respectively, as screw entry points to ensure safe application. The results of this cadaveric study are thought to be a good guideline for safe screw placement in clinical application.






 XML Download
XML Download