

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Decompressive craniectomy is widely used in the neurosurgical field to relieve intractable intracranial hypertension in patients with traumatic brain injury (TBI), cerebral infarction, subarachnoid hemorrhage (SAH), intracerebral hemorrhage (ICH), or for other reasons1,3,7,17,18,21,22). Once craniectomy has been performed, surviving patients are obligated to undergo a second procedure for cranial reconstruction. The indications for cranioplasty (CP) are usually protective and cosmetic23). Besides these, CP has been reported to facilitate neurological recovery and to improve cerebral blood flow, cerebrospinal fluid (CSF) hydrodynamics, and metabolic activity23). Although CP is a relatively simple procedure, it has a high complication rate4,8). In addition to the risks inherent in any cranial operation, there are also specific risks to which the procedure is predisposed, such as postoperative infection due to foreign body implantation, hematoma, bone graft resorption, subdural or epidural fluid collection, seizure, and fixed neurological deficits4). Epidural fluid collection (EFC) is a relatively rare complication, and since a substantial number of EFC disappears or regress spontaneously over time, the true incidence of EFC may have been underestimated. There are a few small clinical series describing EFC as complication of CP4,9). The aim of this study was to provide a complete review of all perioperative EFC, defined as EFC within 10 days of surgery, as well as to identify any risk factors that may be associated with EFC following CP. The fate influencing the outcome of EFC were also analyzed retrospectively.
MATERIALS AND METHODS
From January 2004 to December 2012, a total of 117 patients who underwent CP were enrolled in this study. Among these, 49 patients with EFC and 57 without EFC were analyzed. The available hospital charts and clinical records were reviewed retrospectively. CP was performed if the presence of a slack brain and medical recovery permitted reconstruction. Immediately after decompressive craniectomy, the removed bone flaps were frozen and stored under sterile condition at -78℃.
These flaps were later identified and thawed prior to reimplantation for subsequent cranial repair. Non-autologous bone flaps were reconstructed with polymethylmethacrylate (PMMA). During cranioplasty, the layer for replacement of the bone fragment was dissected between the myocutaneous flap and the dura-like layer covering the brain. The bone margin encasing the craniectomy defect was exposed. After achieving meticulous hemostasis in the epidural spaces with bipolar coagulation and hemostatic agents, circumferential and bone flap dural tack-up sutures were placed to reduce epidural dead space. The autologous bone flap or PMMA was fixed in place with microscrews and plates. The temporalis muscle was dissected as a separate layer and fixed at the bone flap. Then, a closed-suction drain was placed in the epidural and subgaleal space for 3 to 7 days.
The variables included gender, age at CP, initial diagnosis at the time of craniectomy, interval from craniectomy to CP, material used for the bone graft, size of bone flap, operating time, postoperative air bubbles in the epidural space, existence of a preoperative ventriculoperitoneal (V-P) shunt, dural calcification, extensive cerebromalacia and severe depression in craniectomy site. Patients were subdivided into 3 age groups : young (<30 years of age), middle-aged (30-60 years of age), and old (>60 years of age). The interval from craniectomy to CP was stratified into early (within 2 months) and later (more than 2 months). The size of the skull defect was calculated by a formula, 3.14×long axis×short axis. It was classified as small (< 75 cm2), moderate (75-125 cm2), or large (>125 cm2). Eleven patients had hydrocephalus after craniectomy; a V-P shunt was performed at the same time as CP in 6 of these patients, and the CP followed the V-P shunt in 5 other patients. Programmable valves were used for the V-P shunts.
Of the enrolled patients, 106 were classified according to whether they had or did not have EFC. A brain computed tomographic (CT) scan was taken in order to determine EFC. We defined EFC as low density fluid in the epidural space on brain CT scan within 10 days after CP. Serial brain CT scans were obtained to detect changes of EFC. The two groups were compared to identify risk factors for EFC.
According to the degree of EFC, EFC was divided into minimal (brain compression without midline shift), moderate (brain compression with a little midline shift) and extensive (brain compression with definite midline shift). The full course of follow up was evaluated for each patient so that EFC after discharge from the CP procedure would be included.
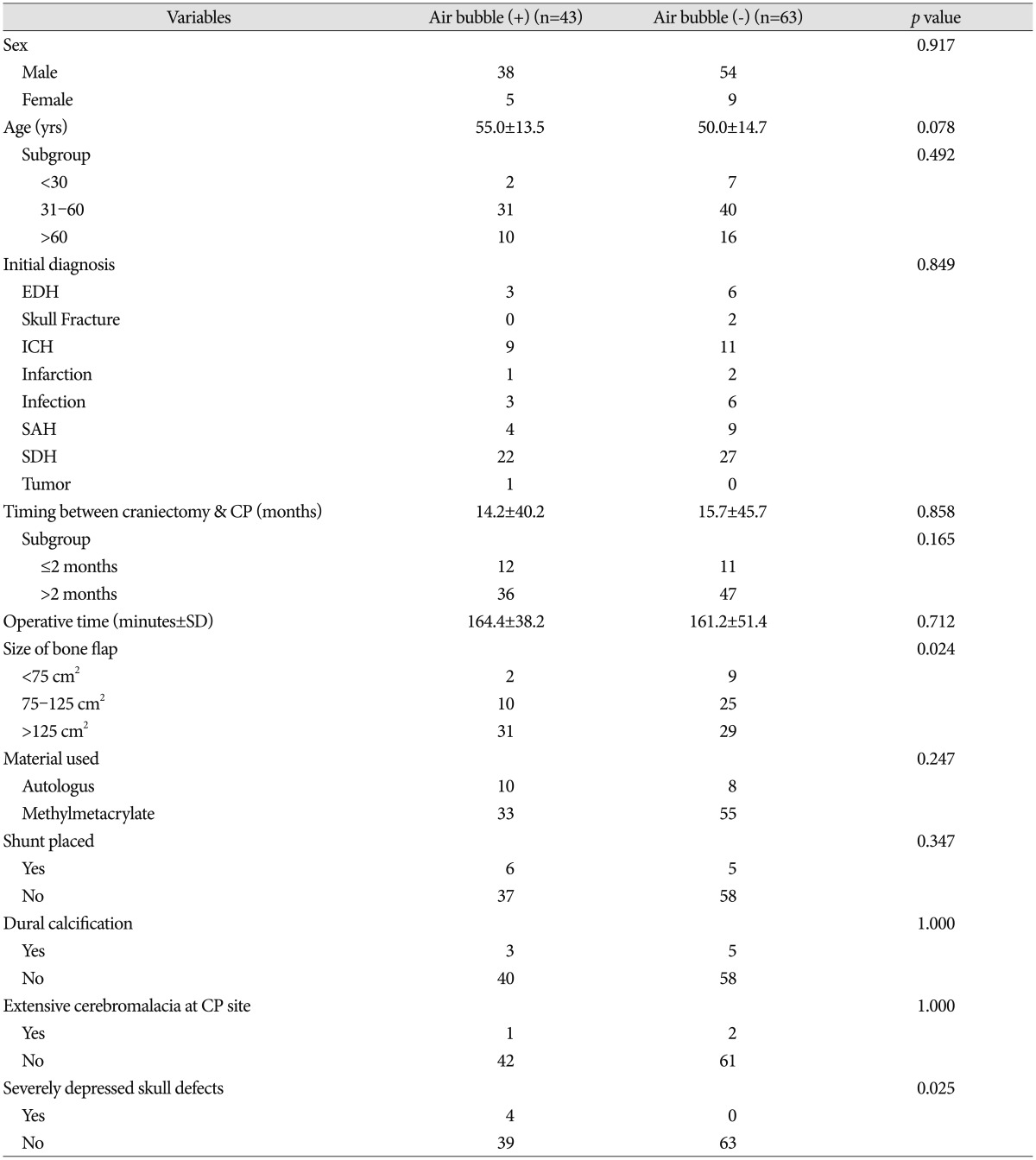
43 of 106 patients suffered from postoperative air bubbles in the epidural space following CP. The factors associated with epidural air bubbles were also investigated. The including factors were gender, age at CP, initial diagnosis at the time of craniectomy, interval from craniectomy to CP, material used for the bone graft, size of bone flap, operating time, existence of a preoperative V-P shunt, dural calcification, extensive cerebromalacia and severe depression in craniectomy site.
Statistical analysis
Data were analyzed with the R language ver. 3.01 (R Foundation for Statistical Computing, Vienna, Austria) and p-value <0.05 of the test was considered statistically significant. Statistical significance for comparisons between two groups was tested using the independent t-test for continuous variables. Categorical variables were compared using Pearson's chi-square test or Fisher's exact test. Multivariate logistic regression models with the inclusion criterion of a p values <0.05 were used to identify the determinants related to EFC following CP.
RESULTS
Complications of cranioplasty
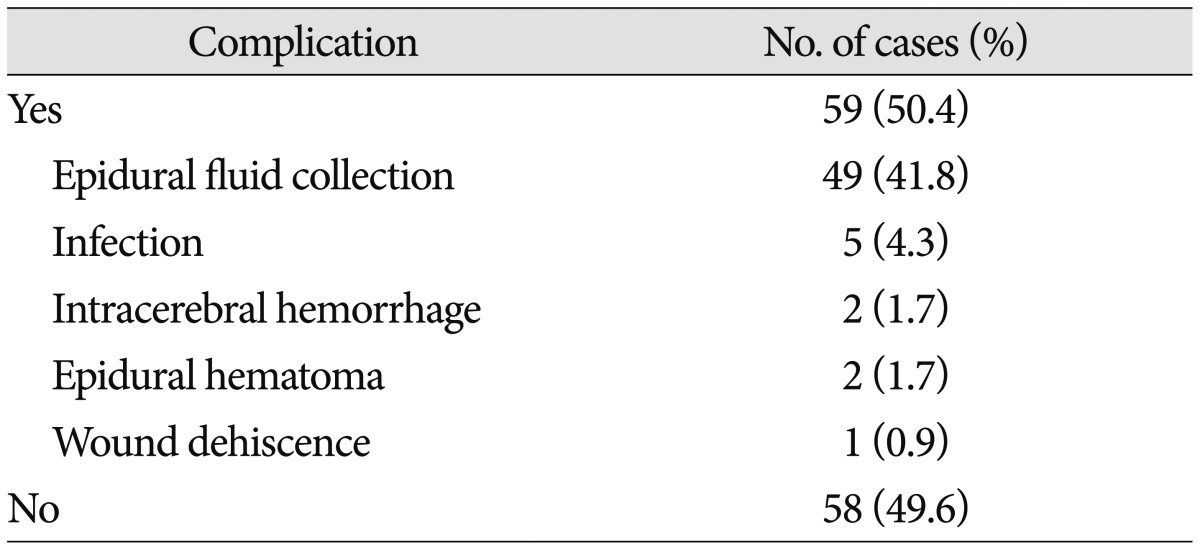
Overall 59 (50.4%) of the 117 patients suffered CP-related complications. These consisted of EFC in 49 patients (41.8%), infection in 5 (4.3%), ICH in 2 (1.7%), EDH in 2 (1.7%) and wound dehiscence 1 (0.9%) (Table 1). The 49 patients with EFC and 57 patients without EFC were included in this study.
Assessed variables for the development of EFC
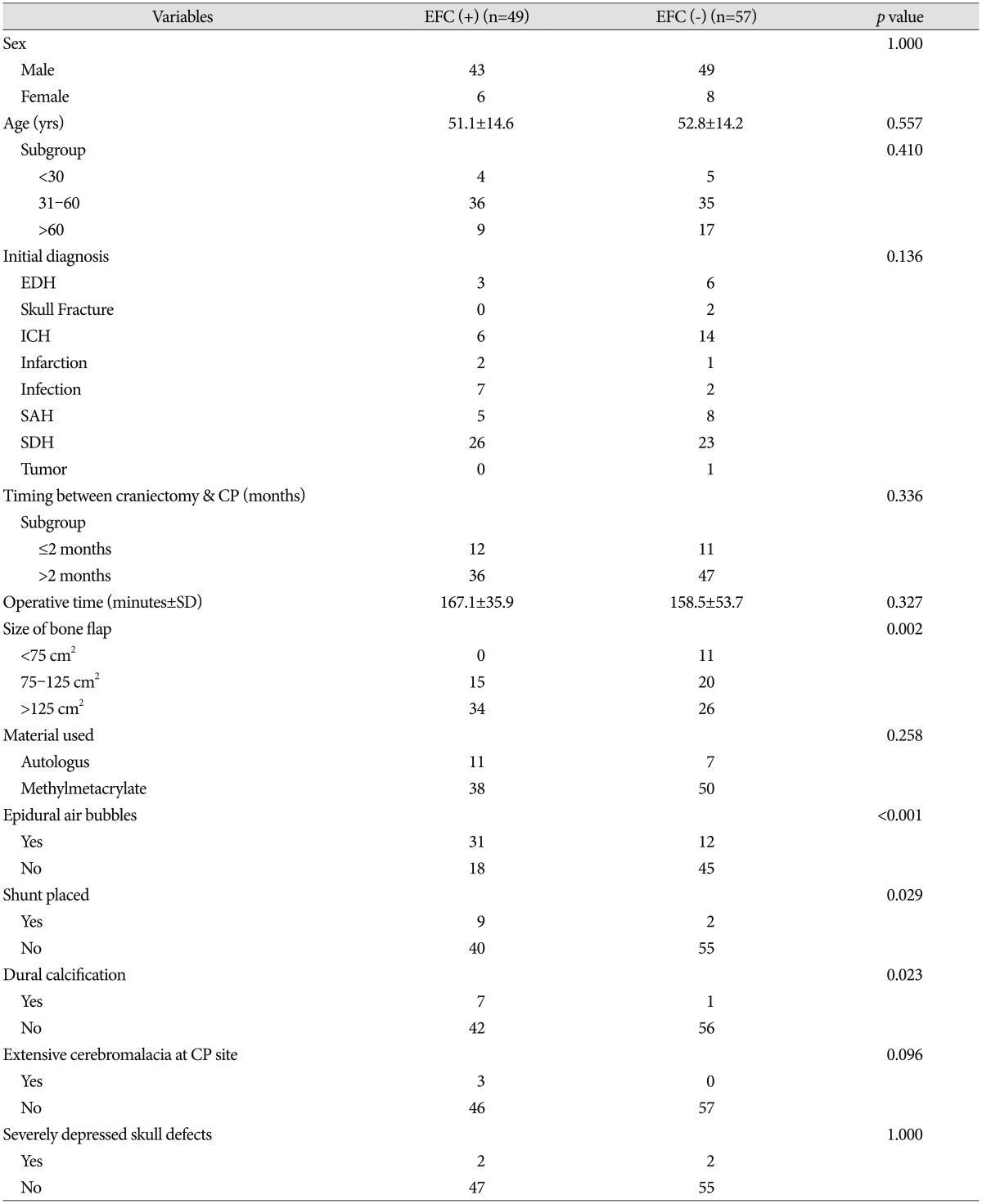
Baseline patient characteristics and the results of EFC stratified by categorical variables are summarized inTable 2.
Gender and age
Of the 106 patients, 92 were men (86.8%) and 14, women (13.2%). Number of EFC cases among the males and females were 43 (46.7%) and 6 (42.9%), respectively (p=1.000). The mean age of the study population was 52.0±14.3 years; that of the 49 patients with EFC was 51.1±14.6 years, and that of the 57 patients without EFC was 52.8±14.2 years (p=0.557). The frequencies among the young, middle-aged and older patients with EFC were 44.4% (4/9), 50.7% (36/71) and 34.6% (9/26), respectively (p=0.410).
Initial diagnosis
The initial diagnosis for craniectomy were divided into 6 general categories; 1) traumatic injuries such as EDH or SDH and skull fracture, 2) SAH due to ruptured aneurysm, 3) cerebral infarction, 4) brain tumor, 5) ICH, 6) infectious processes such as cerebral abscess, subdural empyema, bone plate infection. Differences in rates of EFC between the initial diagnosis were statistically not significant (p=0.136).
Interval between craniectomy and cranioplasty
Patients who underwent replacement early (within 2 months) had an EFC rate of 52.2% (12/23), and those who underwent replacement later (more than 2 months) had a rate of 43.4% (36/83) (p=0.336).
Operative times
The mean operative times for those with EFC and those not having EFC were 167±35.9, 158.9±53.7 minutes respectively (p=0.327).
Size of the skull defect
The development of EFC was more common when the skull defect was large. It occurred in 0 of 11 cases (0.0%) with defects <75 cm2, 15 of 35 cases (42.9%) with defects 75-125 cm2 and 34 of 60 cases (56.7%) with defects >125 cm2. These differences were statistically significant (p=0.002).
Material used for cranioplasty
The defect was reconstructed using saved autologous bone in 17.0% (18/106) of the patients, and using PMMA in 83.0% (88/106) of the patients. Patients receiving autologous bone had an EFC rate of 61.1% (11/18) compared to 43.2% (38/88) among the patients receiving PMMA (p=0.258).
Epidural air bubbles and V-P shunt placed
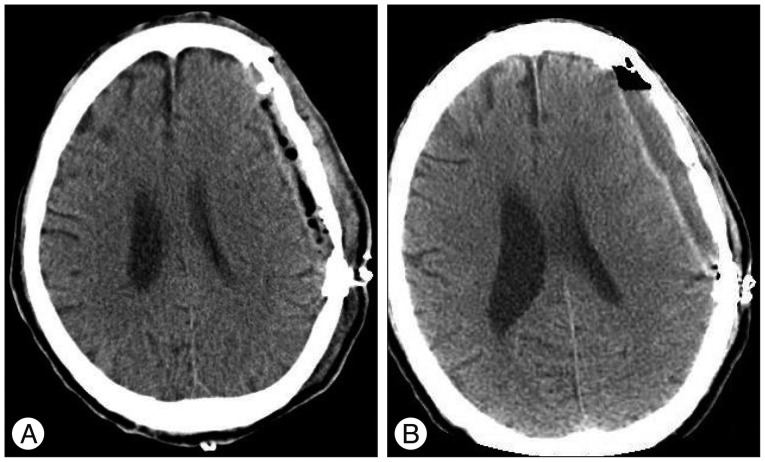
The rate of EFC was a 72.1% (31/43) in patients with postoperative epidural air bubbles in brain CT scan, and 28.6% (18/63) in those without bubbles (Fig. 1). The difference in the rate of EFC with and without epidural air bubbles showed a trend toward significance (p<0.001).
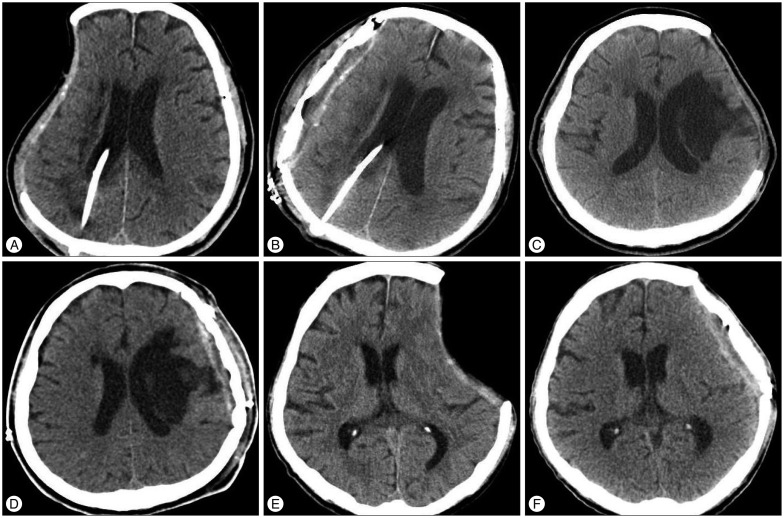
When overt hydrocephalus is present during evaluation for cranioplasty, consideration should be given to permanent CSF diversion either before or at the time of cranioplasty. We performed a V-P shunt along with CP in 6 patients, and CP followed the V-P shunt in 5 patients. Patients receiving a V-P shunt operation had an apparently higher rate of EFC (81.8%) than those without shunt operation (42.1%) (Fig. 2A, B). This finding also reached statistical significance (p=0.029).
Dural calcification, extensive cerebromalacia and severe depression at the craniectomy site
The rate of EFC was a 87.5% (7/8) in patients with preoperative dural calcification, and 42.9% (42/98) in those without dural calcification (p=0.023). Other variables such as extensive cerebromalacia (p=0.096) and severe depression at craniectomy site (p=1.000) did not affect the rate EFC (Fig. 2C-F).
Fate of EFC
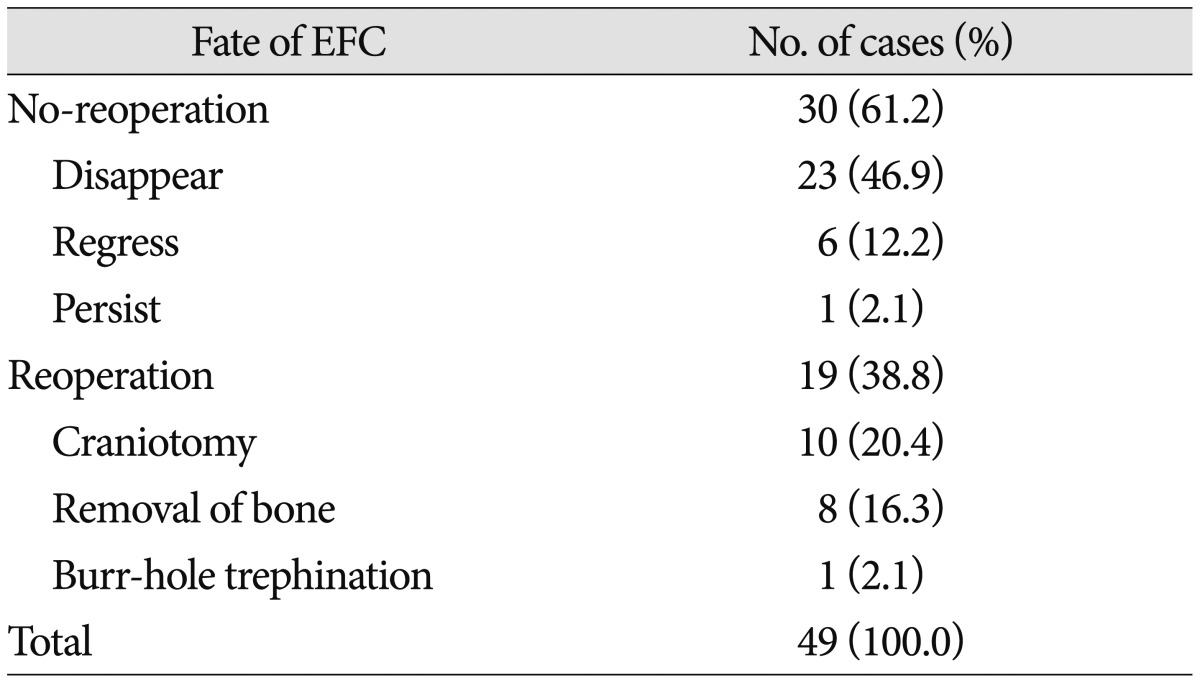
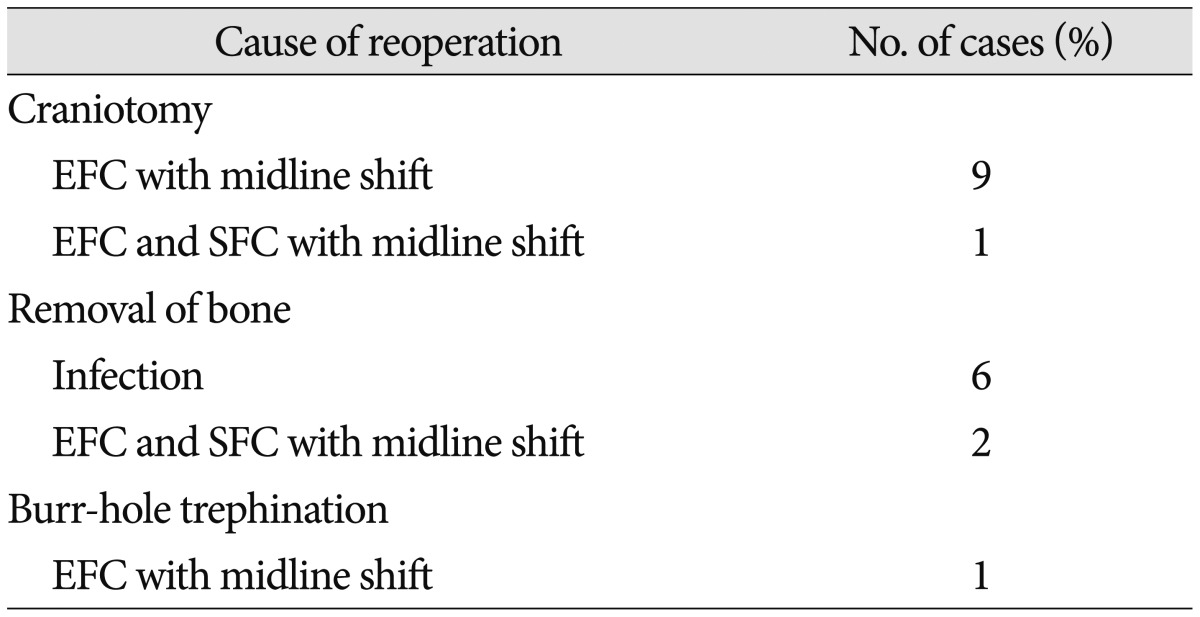
The mean length of brain CT scan follow-up periods in the EFC group was 12.5±16.9 months (range, 0.5-60.7 months). Most of the EFC disappeared (46.9%) or regressed (12.2%) over time during follow up. However, 19 patients (38.8%) required reoperation. Reoperation included 10 craniotomies, 8 for removal of bone, and one for burr-hole trephination (Table 3). The cause of reoperation was due to symptomatic EFC, infection following EFC and persisted EFC with subgaleal fluid collection (Table 4).
Correlation between amount of EFC and reoperation
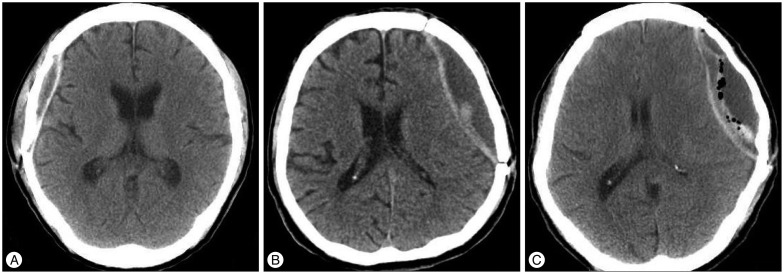
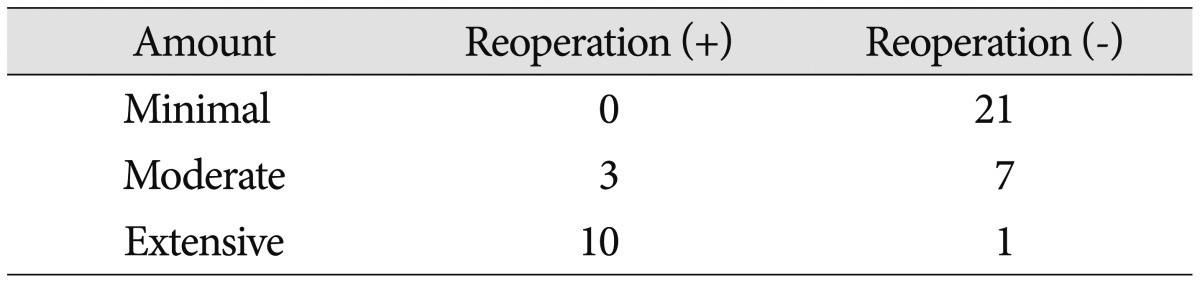
Excluding the patients (n=6) who underwent reoperation due to infection following EFC, reoperation (n=13) after CP was more common when the amount of the EFC increased (p<0.001). It occurred in 0 of 21 cases with minimal EFC (0.0%), 3 in 10 cases with moderate EFC (30.0%) and 10 of 11 cases with extensive EFC (90.1%) (Table 5,Fig. 3).
Statistical analysis
In the t-test and chi-square test, size of bone flap (p=0.002), presence of postoperative air bubbles in the epidural space (p<0.001), shunt placed (p=0.029) and dural calcification (p=0.023) were significant risk factors for EFC. However, in the multivariate logistic regression analysis, postoperative air bubbles in the epidural space (OR, 7.33; 95% CI, 2.81-20.87) and dural calcification (OR, 10.94; 95% CI, 1.50-228.27) were significant risk factors (Table 6). Overall, 43 of 106 patients (40.6%) suffered from postoperative air bubbles in the epidural space following CP. Size of bone flap (p=0.024) and severe depression at craniectomy site (p=0.025) were statistically significant factors for postoperative epidural air bubbles (Table 7). But, in the multivariate logistic regression analysis, there was no statistically significant factor for air bubbles in the epidural space.
DISCUSSION
Data from recent studies have indicated that CP following decompressive craniectomy is associated with high complication rates ranging from 16.4% to 34%2,4,8,12,20). However, these studies mainly analyzed major complications such as infection, hematoma formation, and bone flap resorption. Sobani et al.19) analyzed 96 patients who had undergone CP. The overall complication rate was noted in 36.5% (n=35), of which 10 were major complications such as hydrocephalus, osteomyelitis, SDH, and EDH, and 25, minor complications including breakthrough seizures, CSF leak, postoperative subgaleal fluid collection, superficial wound infections, and new-onset transient neurological deficits. Among minor complications, reports of EFC after CP are uncommon and limited to small series. In a series of 213 patients, Chang et al.4) reported that 13 patients (6.1%) experienced fluid collection complications. Recently, Lee et al.9) analyzed detailed incidence, predictive factors and fate of EFC after CP. Of 59 patients, EFC was occurred in 22 patients (37.3%). In our series, 59 (50.4%) of 117 patients had CP-related major and minor complications. Our overall complication rate was higher than that in other studies4,8,12,19) because in our case minor complication such as EFC was markedly higher (41.8%) than reported previously. The higher EFC in our study could be explained as follows. First, all patients demonstrating EFC on follow-up brain CT scans within 10 days were included, regardless of the amount of EFC. Second, previous studies may have not included small amount of EFC as a complication of CP because it seldom had a detectable effect on neurological status and a substantial number of EFC disappeared or regressed over time. Accordingly, the true incidence of EFC may have been underestimated.
Although the cause of EFC is unknown, we suppose that CSF may leak through dural defects that created during CP; alternatively, postoperative exudate from the dissected subgaleal region and muscle may accumulate due to failure of brain expansion.
It is generally recommended that CP be performed at least 3 to 6 months after the initial craniectomy. If the patient has a history of intracranial infection or an open craniocerebral injury, the procedure can be delayed for at least 6 months after the first surgery5). However, some authors have advanced the idea of early CP after decompressive craniectomy to alleviate complications from craniectomy2,10,14,15).
Cho et al.5) suggest that early cranioplasty was effective in improving ADL of patients. The Barthel index of ADL was found to be significantly higher in the early cranioplasty group. In addition, early cranioplasty does not increase relative risk of complications, such as infection or fluid collection.
Chun and Yi6) detected subdural fluid collection in follow-up brain CT scans in 7% (2/30) in an early CP group (within 1 month after craniectomy), whereas in a control group in which CP was performed over 3 month after craniectomy, 46.7% (7/15) of patients had subdural fluid collection (p=0.003). The authors explained this observation by suggesting that the potential dead space between the skull and the brain encountered during CP was reduced if CP was performed when brain swelling remained.
In our study, patients were classified into two groups according to the time from craniectomy to CP (early, ≤2 months, and late, >2 months), but there was no difference in the rate of EFC between the early and late CP groups (p=0.336).
PMMA is the most common alloplastic material used in CP12). There are some reports researching fixation materials and infection after CP. Cho et al.5) reported fixation materials and usage of bone cement (PMMA) had no effect on the rate of cranioplasty infection. But, there are a few reports analyzing the occurrence of EFC and fixation materials. Lee et al.9) demonstrated that the type of graft material (autologous vs. PMMA) was not associated with EFC after CP. In our study, the EFC rate was 61.1% using autologous bone and 43.2% using PMMA (p=0.258).
Some authors reported that patients with a V-P shunt at the time of cranioplasty were at higher risk for complications including subdural fluid collection because of the relative intracerebral hypotension that a shunt introduced15,16). It is very important how to expand the concave space. Oh et al.13) proposed a simple technique to occlude the shunt tube before cranioplasty and to be the head-down position on operation. Their study was done on 23 patients undergoing CP and V-P shunt operations after the decompressive craniectomy. They claimed that the outcomes of shunt operation performed after CP tended to be better than when CP was performed after shunt operations, and the implantation of patient's own skull bone as early as possible may be better than later CP (3-6 months). But, Chang et al.4) supported that the presence of a ventricular shunt did not seem to influence the complication rate after cranioplasty. We performed CP followed by V-P shunts continuously in 6 patients and CP followed by V-P shunt at the intervals of several months in 5 patients. Programmable valves were used for the V-P shunts. The EFC rate among patients with shunts was higher (81.8%) than among the patients without shunts (42.1%). The effect reached statistical significance (p=0.029).
Lee et al.9) reported that dural calcification were founded to be the predictive factor in the formation of EFC after CP. Dural stiffness due to dural calcification may prevent the expansion of brain, resulting in creation of epidural dead space. In our study, patients who had preoperative dural calcification was 8 patients, 7 with EFC and 1 without EFC. It was statistically significant in EFC group (p=0.023). We performed 3 cases of CP for extensive cerebromalacia at cranioplasty site. All 3 cases involved EFC (p=0.096).
A CP for severe depression under the craniectomy site may result in dysfunction of the underlying brain, risk of fluid collection and hematoma formation in the epidural and subdural space due to the large dead space. If CP is not contraindicated in patients with large, concave flaccid skull defects, implanting the patient's own skull bone as early as possible prior to the appearance of delayed neurological impairment may be better than later CP11,13). We encountered 4 cases of severely depressed skull defects without V-P shunts. We used a simple technique to be the head-down position on operation. Two of cases involved EFC after CP and the other two cases did not have EFC (p=1.000). Park et al.14) reported that infection was more common when the skull defect was large, occurring in 6.9%, 11.1%, and 37.5% of patients with small, moderate and large defects, respectively (p=0.003). However, we are not aware of any study of the relationship between size of the skull defect and the occurrence of EFC after CP. In our study, the EFC rate increased with the size of defects (p=0.002). We suggest the following explanations for the increased probability of EFC formation in large skull defect : first, the chance of dural damage is higher in large skull defect than small ones, and CSF leaks through a dural damaged during CP; second, more postoperative exudate may accumulate from large dissected scalp flap than from small ones due to insufficient blood supply to the end of the flap.
Lee et al.9) reported that the most reliable factors for EFC were an air bubbles in epidural space and dural calcification, because 90.9% of the patients in the EFC group had air bubbles after CP compared 9.1% who did not. That is also the case with us. The corresponding rates were 72.1% and 28.6% (p<0.001), and air bubbles in epidural space and dural calcification were the reliable risk factors for EFC.
We analyzed several factors that might be associated with epidural air bubbles following CP. Size of bone flap (p=0.024) and severe depression under the craniectomy site were statistically significant in forming epidural epidural air bubbles after CP (p=0.025). We suggest the following explanations for the increased probability of air bubbles in epidural space. First, large bone flap have an increase in the possibility of the dead space that cause formation of air bubbles and resulting in EFC. Second, severe depression under the craniectomy site result in creation of epidural dead space that cause formation of air bubbles, but it was not associated with EFC in our cases.
Lee et al.9) reported that 22 (37.3%) of 59 patients suffered from EFC following CP and the EFC disappeared or regressed over time in 12 (54.5%) of these patients, while 5 (22.7%) required reoperation. In our cases, 29 (59.1%) of our 49 patients disappeared or regressed over time and 19 (38.8%) required reoperation. The cause of reoperation was due to symptomatic EFC and infection due to persisted EFC and subgaleal fluid collection.
As far as we know, only a few authors6,9) have analyzed the occurrence of EFC after CP and the predictive factors for its development. Most reports analyzing the outcome of CP appear to have ignored or underestimated the frequency of EFC because it is often asymptomatic and has a good prognosis. But, our data reveals that incidence of EFC was high and 38.8% of EFC cause reoperation due to existence of definite midline shift in brain CT and infection. However, our data are too limited to make definitive conclusions as to this point. It is retrospective in nature, the sample size is small and there is a lack of long-term follow-up data. Nevertheless, the result of our study imply that EFC is frequently occurred complication after CP and provides significant information such as risk factor and the fate of EFC after CP.
CONCLUSION
In the current study, EFC is predicted by postoperative air bubbles in the epidural space and preoperative dural calcification. When the skull defect is large, surgeon should be aware that the patient runs a risk of EFC. Large numbers of EFC can be treated conservatively, but reoperation is necessary to resolve 38.8% of cases due to symptomatic EFC and infection. Since EFC occurs frequent after CP, it should be emphasized with complication after CP.

 XML Download
XML Download