

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Stent-assisted coiling is a safe and effective method for treating wide-necked aneurysms1), but ischemic stroke related to stent thrombosis is a major potential drawback. All thromboses occur within one year after the initial procedure, very late stent thrombosis (VLST), which is defined as stent thrombosis occurring one year after implantation2), following sole stent-assisted coiling has not been previously reported. Here, we report the first case of VLST, which occurred 14 months after a typical sole stent-assisted coiling procedure.
This case highlights the possible mechanism of VLST after single stent-assisted coiling and raises concerns about the duration of prophylactic antiplatelet therapy (APT).
CASE REPORT
History and procedure
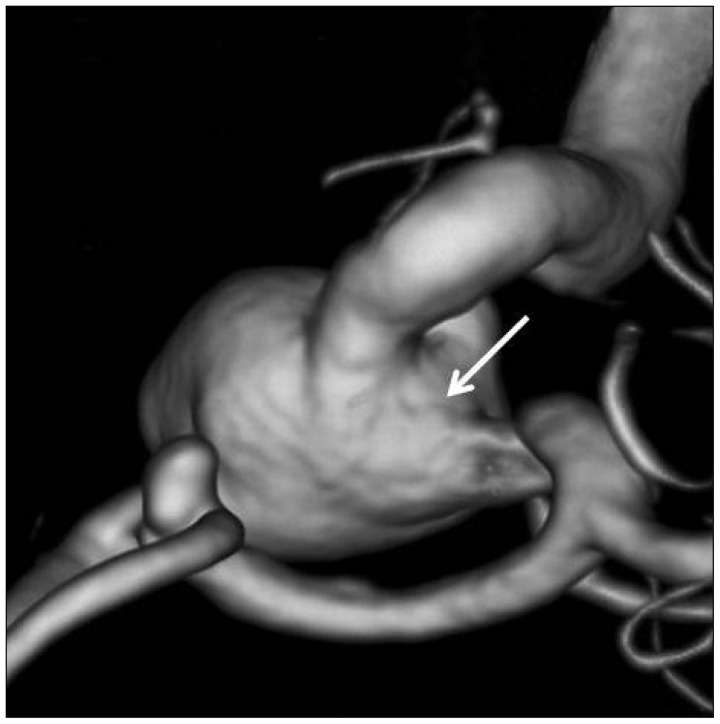
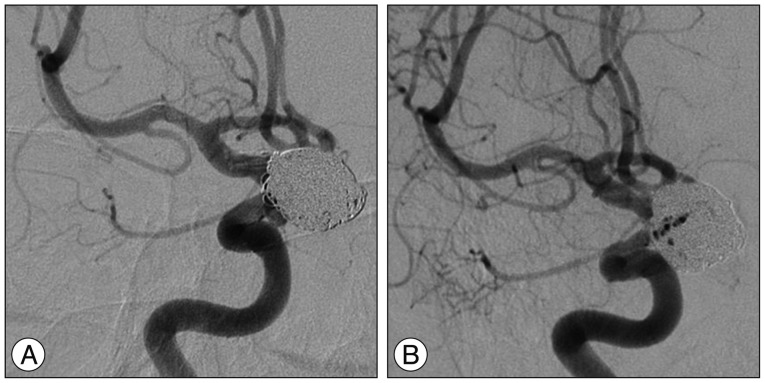
A 56-year-old woman presented with subarachnoid hemorrhage from a ruptured aneurysm in the anterior communicating artery (AcoA) and an unruptured large aneurysm with an ultrawide neck involving the parent artery circumferentially at the right paraclinoid internal carotid artery (ICA) (Fig. 1). The ruptured AcoA aneurysm was treated successfully by clipping. Endovascular coil embolization was performed for the paraclinoid aneurysm 4 weeks after clipping. Coiling was performed using a stent-assisted technique for wide neck remodeling. The patient received oral aspirin (300 mg/d) and clopidogrel (75 mg/d) for 7 days before the coiling procedure, which was performed using a transfemoral approach under full anticoagulation with intravenous heparin (activated clotting time >250 s). First, a closed-cell Enterprise stent (4.5×37 mm; Cordis, Miami Lakes, FL, USA) was navigated in the ICA and implanted across the wide neck of the aneurysm, and coiling then was performed using 19 bare platinum coils (Orbit; Cordis, Miami Lakes, FL, USA) via a SL-10 microcatheter (Boston Scientific, Natick, MA, USA), which was jailed outside the stent. The final angiogram showed near complete obliteration of the aneurysm with minimal neck remnant (Fig. 2A).
The patient had an uneventful postoperative course and was neurologically normal at the out-patient department follow-up. Furthermore, follow-up angiography performed at 12 months after the coiling procedure depicted no change in the small amount of residual filling of the aneurysmal neck and a well-preserved parent artery without any thrombosis or stenosis (Fig. 2B).
Antiplatelet therapy
The patient was maintained on dual antiplatelet therapy (APT) for 12 months after the initial treatment. We used 300 mg aspirin and 75 mg clopidogrel as the dual antiplatelet regimen for 4 weeks followed by 200 mg aspirin and 75 mg clopidogrel for 5 months and 100 mg aspirin and 75 mg clopidogrel for the remaining 6 months. After the 1-year follow-up angiographic evaluation, dual APT was switched to aspirin monotherapy.
Very late thrombosis
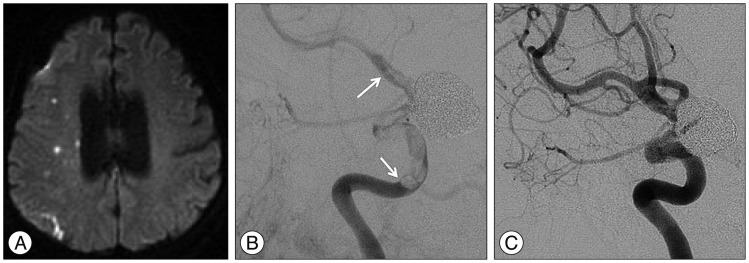
Two months after switching to aspirin monotherapy, the patient experienced transient ischemic attack symptoms. Computed tomography angiography revealed occlusion of the right ICA at the level of stent implantation. Diffusion weighted imaging taken for evaluating ischemic symptoms demonstrated multiple embolic infarctions in the right hemisphere (Fig. 3A). Digital subtraction angiography (DSA) revealed in-stent thrombosis extending from the cavernous ICA to the distal ICA (Fig. 3B). The patient admitted stopping her aspirin medication prior to a dental procedure conducted 3 days before the ischemic event.
Management of thrombosis
The patient was managed conservatively, because the potential risk of thrombus distal migration was considered to be high for interventional therapy. Clopidogrel 75 mg was added to aspirin 200 mg and low molecular heparin was administrated for 10 days. A follow-up angiography showed completely resolution of the thrombosis with good flow through the parent artery (Fig. 3C). The patient was discharged neurologically intact on 200 mg aspirin and 75 mg clopidogrel.
DISCUSSION
Stent-assisted coiling is increasingly being used to treat aneurysms6,11), but, although this is an effective and relatively safe technique1), it has inherent problems such as thromboembolic complications and in-stent stenosis10,18). The timing of stent thrombosis can be classified as acute (<24 h post procedure), early or subacute (24 h to 30 days post procedure), late (31 days to 1 year post procedure), or very late (>1 year post procedure)2). In-stent thrombosis within 1 year after stenting has been reported to occur at a rate of around 3% after stent-assisted coiling10,14,15,19). However, no report has previously described VLST following implantation of a sole stent, which is self-expanding intracranial stent designed for coiling assistance. The mechanisms of VLST previously proposed are; progressive in-stent stenosis, premature discontinuation of dual APT, delayed atypical response to adjacent polyglycolic acid-loaded "bioactive" coils, spontaneous occlusion of the parent artery, stenting across major arterial side branches, stent mal-apposition, stent fracture, stent strut penetration of the necrotic core, disruption of vulnerable plaque near the stent, radiation therapy, and hypersensitivity vasculitis4,7). In our case, no in-stent stenosis or stenosis around the stented vessel was noted by 1-year follow-up angiography. Furthermore, we used only bare-metal coils. Thus, premature discontinuation of antiplatelet medication was the likely cause of VLST in our case. The prevention of thromboembolic complications after stenting is currently achieved with prophylactic dual APT12), but the regimens and durations of prophylactic APT are controversial9,21). It is recognized intracranial stents are thrombogenic until stent endothelialization occurs, and that the duration of APT should be based on the completion of endothelialization. It has been reported by some that endothelialization is complete within 6 months after BMS implantation5,8,16), but no human data is available regarding the rate of stent endothelialization after stent-assisted coiling. In the interventional cardiology field, current guidelines recommend dual APT for at least 1 month for BMSs, but up to 1 year for drug-eluting stents, which cause delayed endothelialization22). However, in the neuroendovascular field, the optimal duration of prophylactic APT following stent-assisted coiling remains undefined, and clinical practices are highly discrepant; some authors have recommended only 3 or 6 months of antiplatelet therapy after stent placement for coiling17,20). These recommendations seem to be based on the facts that the target vessel for stent placement is usually nonatherosclerotic and that stents being used for coiling assistance are of bare-metal and have self-expandable properties, and thus, do not delay endothelialization over stent struts or cause endothelial injury16).
However, a much longer duration of APT may be required when stent endothelialization is only partially achieved. The occurrence of VLST may mean that formation of a complete neointimal layer incorporating stent struts has failed despite the passage of considerable time after stent implantation. Furthermore, it has been established that exposed stent struts are prone to thrombosis. Our patient had a large aneurysm with a circumferential wide neck, which suggests a large portion of the stent might have unopposed the parent vessel. In addition, it is likely that stent struts facing a circumferential wide aneurysmal neck are endothelialized at a far slower rate than that of a similar sized stents placed across a smaller aneurysmal neck. Another possible pathophysiology of incomplete endothelialization involves mechanical factors of closed-cell stents. These stents can be kinked or flattened in tortuous curves, which can result in incomplete stent apposition, causing incomplete endothelialization3,13). Thus, the ultra-wide neck involving the parent artery circumferentially and the closed-cell stent deployed in the tortuous carotid siphon probably contributed to the incomplete stent endothelialization in our case. Although we present only a single case of VLST after sole stent-assisted coiling, our observation suggest that APT is needed for much longer period after sole stent-assisted coiling for a large aneurysm with an ultra-large circumferential wide neck. A study is required to determine optimal APT regimens according to stent type, number, and aneurysm size, shape after stent-assisted coiling.
CONCLUSION
We present a case of a VLST after sole stent-assisted coiling. Although VLST is extremely rare, it is a serious event with potentially devastating consequences. This case demonstrates that long-term APT and patient strict adherence are required to possibly prevent this complication when a large portion of the stent is anticipated to be unopposed to the vessel wall.
 XML Download
XML Download