

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Upper cervical spine instrumentation is always challenging for spine surgeons due to the highly variable pedicle anatomy and vertebral artery anomalies. Particularly, C1-2 fixation techniques have been developed in order to overcome those problems, and C1 lateral mass-C2 pedicle screw fixation has been increasingly used since it was introduced in 1994 by Goel and Laheri3) and modified in 2001 by Harms and Melcher5). Many published reports describe the technique's superiority to transarticular C1-2 fixation and several posterior fusion methods in biomechanics and feasibility when vascular and bony anomalies exist, although the procedure is still challenging and its accuracy does not provide any certainty to surgeons. Because it is a free-hand technique, Abumi's method and the fluoroscopy-guided technique have their own limitations in terms of reliability9), so navigation systems have been recently introduced to aid in these procedures. Among them, the computed tomographic (CT)-based navigation system was recently revealed to have excellent results : over 89% accuracy reported, even in the thoracolumbar spine2) and an 85% to 97% accuracy rate in lower cervical spine instrumentation, as reported in previous articles12,13). However, the accuracy rate for the CT-based navigation system at the upper cervical spine level, especially in C1 and C2 instrumentation, has not been reported yet. We have used the CT-based navigation system in several cervical instrumentation surgeries, and report its safety and efficiency through the comparison of previous reports.
MATERIALS AND METHODS
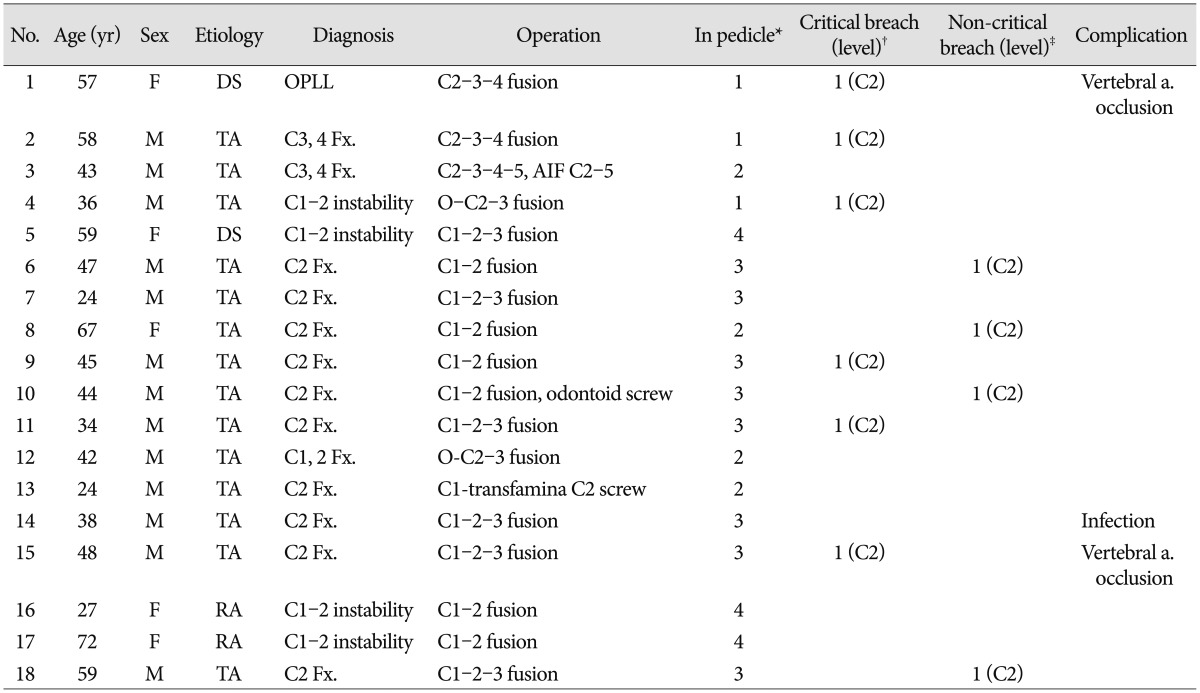
This retrospective study included 25 patients who underwent upper cervical instrumentation, including C1 lateral mass-C2 pedicle screw fixation, between May 2005 and March 2014. The patients underwent the usual posterior approach and instrumentation using CT-based navigation systems (Steal-Station; Sofamor-Danek, Memphis, TN, USA in cases 1 to 4; and Navigation cart II; Stryker, Kalamazoo, MI, USA in the remaining cases) by one surgeon. Among them, 18 patients who has postoperative CT scans participated in this study and the accuracy of the screw positions at C1 and C2 only was analyzed by a third observer. The usual posterior approaches were used and ultimately, two occipito-cervical fusions, 13 C1 lateral mass-C2 pedicle screw fixations, and three C2-3-4 posterior instrumentation were performed (Table 1). The laminectomies were performed in neurologically compromised patients, and a CT-based navigation system and fluoroscopy were used during the pedicle screw instrumentation procedure (Vertex™; Sofamor-Danek, Memphis, TN, USA in cases 1 to 11 and Synapse system; Synthes, West Chester, PA, USA in the remaining cases). The precise position of the screw was evaluated by a postoperative computed tomographic scan and categorized into one of three groups : absolute in-pedicle, non-critical breach (pedicle violation <2 mm), and critical breach (pedicle violation >2 mm).
Surgical procedure
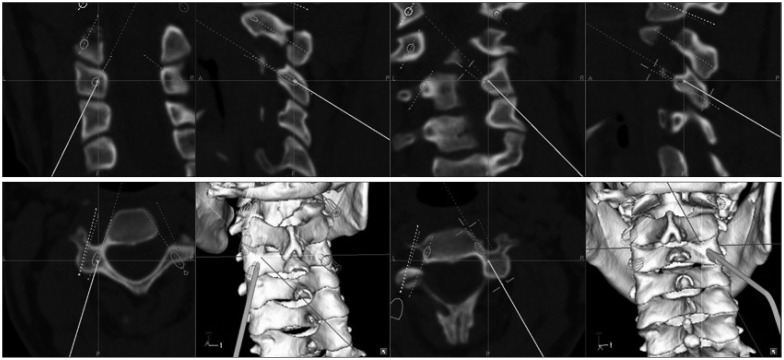
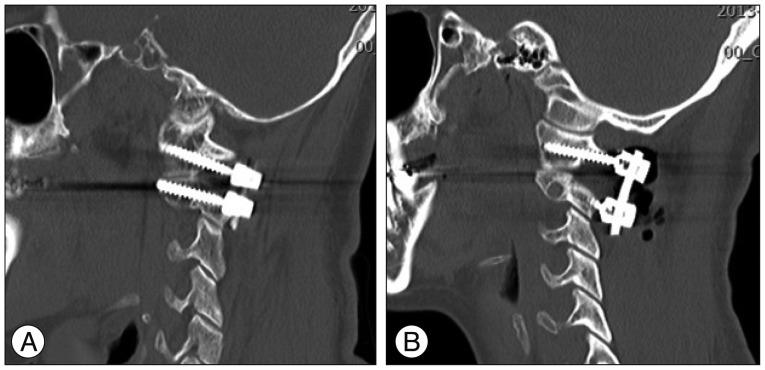
In the prone position, a usual mid-line incision was performed and the reference device was secured at the C2 spinous process after exposure. Navigation procedures included acquiring a preoperative CT image, activating a patient tracker, adjusting the camera angle, registration, tool calibration, and simulation of screw placement. During the registration process, both a point-to-point registration and surface-matching process were used to reduce the mean deviation, and simulation of the screw trajectories was acquired on the navigation monitor (Fig. 1). The C1 trajectory was changed from a lateral mass under the C1 posterior arch (cases 1 to 11) to modification of the pedicle screw with a partial removal of the lower C1 arch (remaining cases) (Fig. 2). During C1-2 screw insertion, additional lateral fluoroscopy was used to confirm the best direction.
RESULTS
A total of 58 screws, including 26 C1 screws and 32 C2 screws were analyzed. Postoperatively, the precise positions of the C1 lateral mass-C2 pedicle screws were 81.1% (47/58); 8.6% (5/58) of the screws were in a non-critical breach position and 10.3% (6/58) of the screws were critical breaches. Most (5/6) of the critical breaches and all of non-critical breaches were observed at the C2 pedicle screws, and only one case of a C1 lateral mass screw showed a critical breach (p=0.033, Kruskal-Wallis test). All cases of breach occurred in traumatic instances, except for one case of degenerative spine disease, which resulted in a C2 critical breach (p=0.091, Mann-Whitney U test). There were three complications (two vertebral artery occlusions and a deep wound infection), but no postoperative instrument-related neurological deteriorations were seen, even in the critical breach cases.
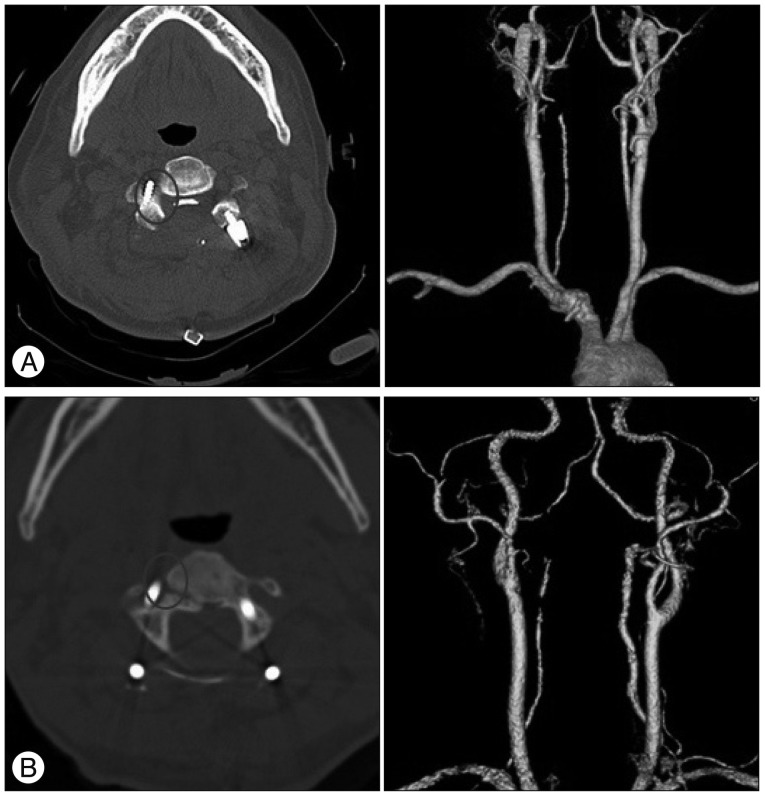
In case 1 and case 15, the right C2 pedicle screw protruded over 50% into the vertebral foramen, even though correct navigation procedures were performed. The postoperative CT angiograms showed that retrograde flow from the opposite vertebral artery covered the distal area (Fig. 3) and no cerebellar infarction and/or symptoms occurred. One patient (case 14) had a deep wound infection postoperatively and wound revision with massive irrigation was performed in response. The patient was discharged without any further complications and/or screw removal procedures.
DISCUSSION
According to the 2000 cadaveric study of Ludwig et al.10), the accuracy rates of C3-7 pedicle screws using the CT-based navigation system are 76% (in pedicle) and 13.4% (non-critical breach). A 2005 clinical study by Rampersaud et al.12) reported an 85% accuracy rate in pedicles; and a 13.1% rate of non-critical breaches and 2.2% occurrence of critical breaches in the thoracolumbar spine. In 2012, Gelalis et al.2) published a systemic review comparing the free-hand technique, and found that the percentage of the screws fully contained in the pedicle ranged from 69 to 94% overall; those that used fluoroscopy ranged from 28 to 85%, while those using CT navigation ranged from 89 to 100% and those using fluoroscopy-based navigation ranged from 81 to 92%. However, those studies were conducted in the thoracic and lumbar spine only. The authors believe that the present study is the first article regarding C1-2 fixation using a CT-based navigation system. In the present study, an 81.1% accurate placement in the pedicle was seen, in addition to an 8.6% rate of non-critical breaches and a 10.3% rate of critical breaches. Those results were not highly satisfactory to the authors, but the C1-2 junction has high mobility, which makes precise stabilization inherently problematic as compared with the lower cervical or thoracolumbar spines. Additionally, seven cases were excluded because their screw positions were correct on the postoperative X-ray so CT scans were not taken. The accuracy rate would be higher than reported here if they were involved in the study. Another clinical study by Richter et al.13) reported a 97% accuracy rate using a navigation system versus a 91.4% accurate rate using the conventional method for C3-6 pedicle screw fixation. A recent article regarding C1 lateral mass-C2 pedicle screw fixation reported a 95.8% correct screw placement14), but the researchers used isocentric C-arm 3-dimensional navigation, which is a more upgraded system than ours.
The possible reasons of the relatively higher rate of breach at C2 than C1 in the present study are described below. One reason is that most of the cases were C2 fractures, so relative instability occurred, and it could cause error and change between the preoperative CT scan and intraoperative position of the patient. Another reason may be that the reference device, which was secured to C2 spinous process, could have been touched and therefore moved, unintentionally during the procedure.
Finally, the authors recommend that more precision be used, both during the point-to-point registration and the surface-merging during the navigation procedure. A modified C1 trajectory could be helpful to reduce intraoperative bleeding, postoperative occipital neuralgia, and operation time.
CONCLUSION
Although a CT-based navigation system can allow surgeons to perform more precise procedures at the lower cervical and thoracolumbar spine, it still has some problems in the upper cervical spine, due to the region's highly variable anatomy. Even though there were no catastrophic complications, more experiences are needed in order to safely conduct upper cervical spine instrumentation surgery.
 XML Download
XML Download