

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Anterior microforaminotomy (AMF) has been developed as an alternative procedure to manage unilateral cervical lesions with preservation of segmental mobility and limited direct decompression around the neural foramen. In 1996, Jho7) described a transuncal approach to AMF, performed through the uncinate process (UP) to preserve the remaining disc. Since then, many authors have reported favorable clinical outcomes of AMF or similar procedures1,2,3,5,8,9,11,13,17,21). and only several authors have described about radiologic outcomes of AMF, including the appearance of instability, static deformity, and a decrease in disc height, although the follow-up period have been relatively short1,5). The presence of radiologic degenerative changes after AMF may affect the surgical outcome in long-term follow-up. To clarify the exact extent and detail of these degenerative processes, we analyzed the radiological outcomes in patients who underwent single-level AMF with a follow-up of more than 6 years.
MATERIALS AND METHODS
Patient population
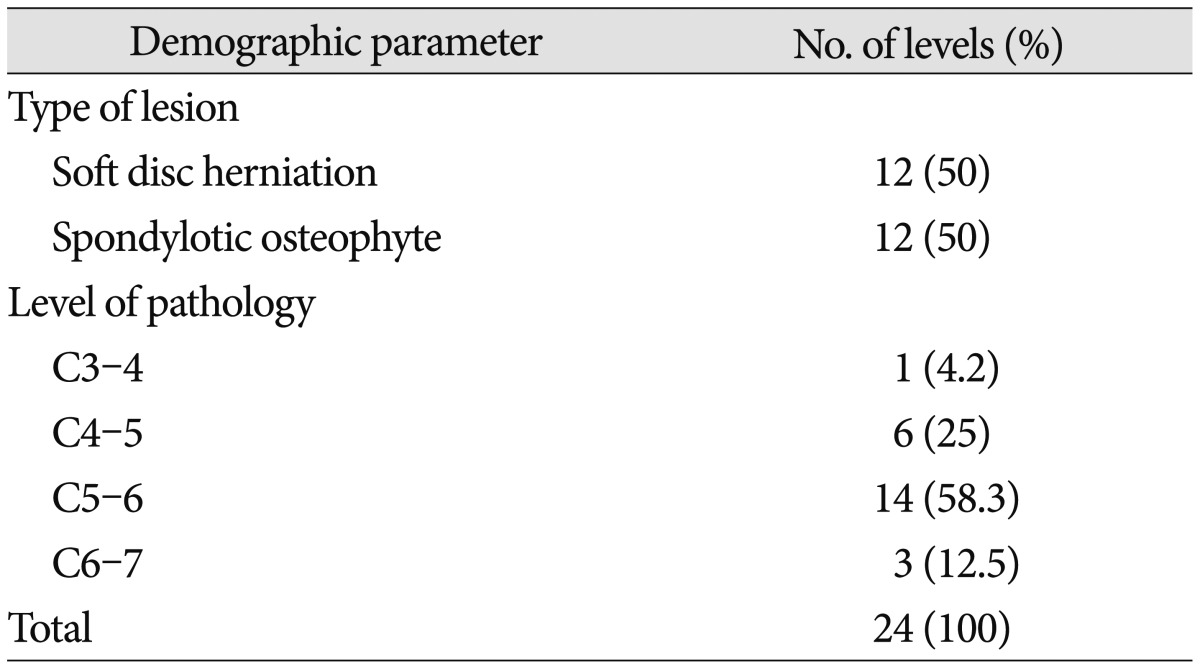
Twenty-four patients were included in this study. The inclusion criteria for this retrospective study were as follows : unilateral cervical radiculopathy that had not responded to conservative treatment in >6 weeks, imaging studies confirming pathologic features corresponding to the clinical symptoms, no previous cervical spine surgery, no evidence of spondylotic myelopathy, no combined cervical procedures, and a follow-up of >6 years. Table 1 provides the preoperative clinical summaries including the type and level of lesions.
Clinical evaluation
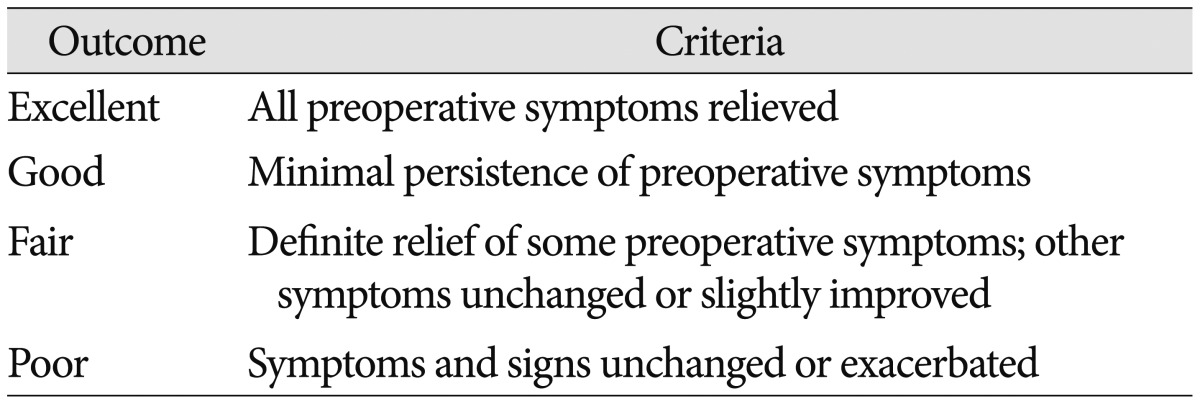
Medical records and our picture achieving and communication system (PACS) data were reviewed to collect clinical and radiological data. Preoperative symptoms and signs were assessed at admission, including the visual analogue scale (VAS) score and the neck disability index (NDI). Postoperative evaluations were carried out at the time of discharge and at systemic follow-up every 2 weeks during the first 3 months and then 1 year after the operation. Final follow-up data were obtained at the time of this study. These data were also graded according to Odom's criteria, according to which, patients were rated from excellent to poor depending on resolution, improvement, or persistence of preoperative symptoms (Table 2).
Radiological evaluation
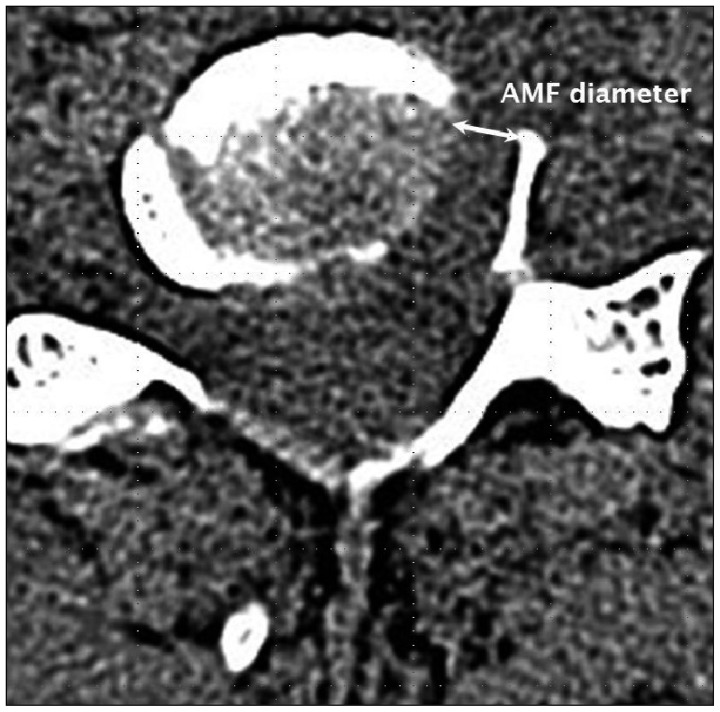
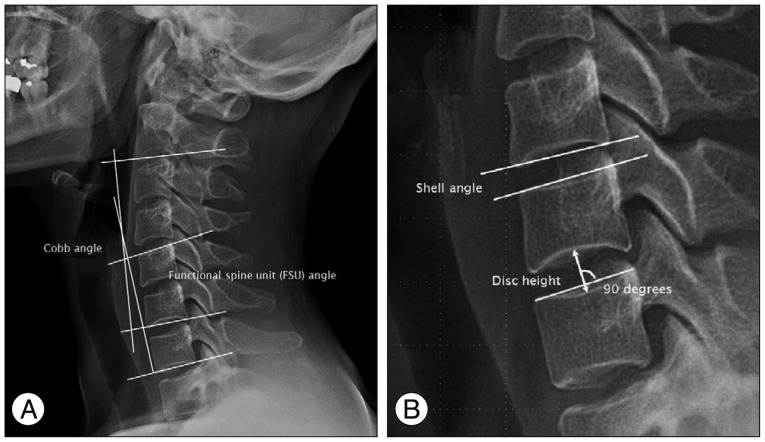
All patients underwent preoperative static and dynamic radiographs, high-resolution CT, and MRI. Postoperative static and dynamic radiographs and high-resolution CT were performed immediately to assess the extent of bone drilling. Follow-up roentgenograms were obtained. Final radiographs of the cervical spine were obtained at the time of this study. The AMF diameter and presence of disc invasion (Dinv) during the AMF procedures were determined using postoperative CT images and operative findings (Fig. 1). Using preoperative and postoperative static neutral lateral radiographs, disc height (DH) of the operated segment were assessed. To evaluate the change of segmental angles after surgery, functional spine unit (FSU) angle and shell angle (SA) of the operated segment were assessed. Also, Cobb angel (the angle formed between a line drawn parallel to the inferior endplate of C2 and a line drawn parallel to the inferior endplate of C7) was assessed to evaluate the changes of overall cervical curvature (Fig. 2). The range of motion (ROM) of each angle was also assessed using dynamic cervical spine radiographs. We measured the angles with quantitative measurement analysis software in a PACS workstation (Starpacs 5.0.8.1; Infinite, Seoul, Korea). Standard statistical analysis was performed with SPSS software for Windows (version 15.0; SPSS Inc., Chicago, IL, USA).
Surgical technique
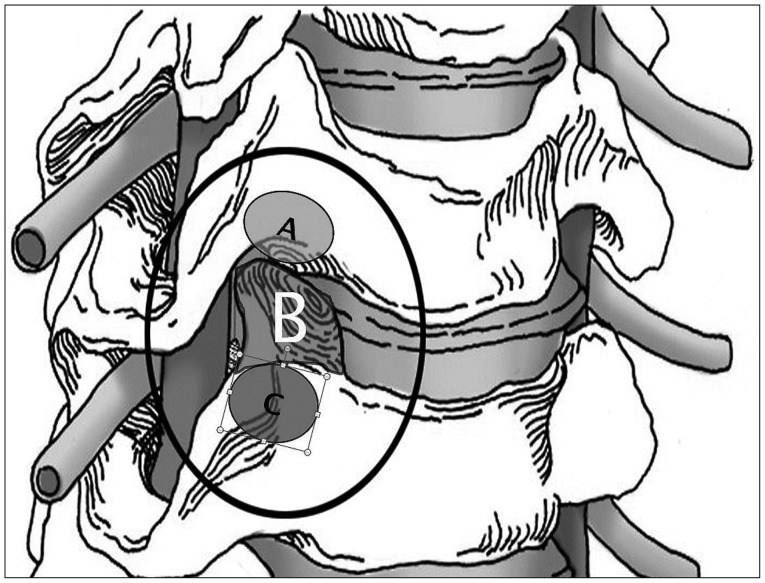
Description of AMF was published previously7). The transuncal approach for AMF was used (Fig. 3). The operation is performed with the patient under general anesthesia. The head is positioned with the midline upright. Both shoulders are gently pulled caudally and fixed with tape. A 3-cm-long transverse incision is made in a skin crease ipsilateral to the radiculopathy. The subcutaneous tissue and platysma muscle are incised along the line of the skin incision. A combination of sharp and blunt dissection is used to access the anterior column of the cervical spine. The prevertebral fascia is opened, and the anterior column of the cervical spine is exposed. The correct level is then confirmed radiographically. An anterior cervical discectomy retractor system is applied. Only smooth-tipped retractor blades are used, thus avoiding injury to the trachea and esophagus medially and the carotid artery and vagus nerve laterally. Retraction naturally exposes the ipsilateral longus colli muscle rather than the midline anterior disc surface. Use of an operating microscope begins at this stage. The medial portion of the longus colli muscle is excised to expose the medial parts of the transverse processes of the upper and lower vertebrae. Once the medial parts of the transverse processes of the upper and lower vertebrae have been identified, the ipsilateral uncovertebral (UV) joint between them can be seen. The interface of the UV joint is angled cephalad from the horizontal line of the intervertebral disc. The UV joint is drilled between the transverse processes using a high-speed microdrill attached to an angled handpiece. To prevent injury to the vertebral artery, the thin cortical bone is left attached to the ligamentous tissue covering the medial portion of this artery; drilling continues down to the posterior longitudinal ligament. As drilling advances posteriorly, the drilling direction is gently inclined medially. When the posterior longitudinal ligament is exposed, a piece of the thin cortical bone remains attached lateral to the ligamentous tissue covering the vertebral artery. This lateral remnant of the UP is dissected from the ligamentous tissue and fractured at the base of the UP. Drilling at the base of the UP must proceed cautiously because the nerve root lies just behind it. When the remaining piece of the UP is removed, the compressed nerve root will be distended forward by bone decompression. If there is no ruptured herniated disc fragment behind the posterior longitudinal ligament, the nerve root decompression is ended. At this point, the posterior longitudinal ligament still covers the nerve root and lateral margin of the spinal cord. If the disc fragment has ruptured though the posterior longitudinal ligament, the tail of the disc material will be visible at this stage, and this disc fragment can be removed. To avoid overlooking a hidden disc fragment, the ligament is incised with an arachnoid knife or microscissors and removed with a 1-mm foot-plated bone punch. Finally, the platysma is closed with interrupted 3-0 absorbable stitches, and the skin is approximated with subcuticular sutures. A cervical collar is not used.
RESULTS
Clinical outcome
Patient population
The studied patients included 14 men and 10 women with a mean age of 49.1 (34-63) years at the time of surgery. The main pathology was spondylosis in 12 patients (50%) and soft disc herniation in 12 cases (50%). The operated segment was C5-6 in 14 patients (58.3%), C4-5 in 6 (25%), C6-7 in 3 (12.5%), and C3-4 in 1 (4.2%) patient (Table 1). There were no surgery-related complications. The mean follow-up was 7.9 (6.4-9.8) years.
Odom's criteria
Of the 24 patients, 17 (70.8%) demonstrated excellent results, 5 (20.8%) demonstrated good results, and 2 (8.4%) experienced a fair outcome.
VAS and NDI scores
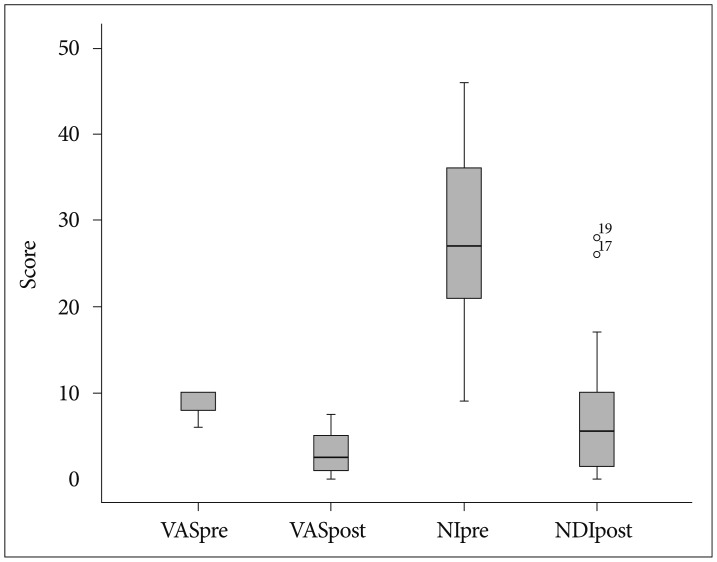
The mean preoperative VAS score was 8.6 (6-10), the postoperative VAS score was 3.0 (0-7.5), and the difference in the VAS scores was 5.5 (0-10). The mean preoperative NDI was 27.9 (9-46), the postoperative NDI was 7.3 (0-28), and the difference in the NDI was 20.6 (1-40). Both the VAS score and NDI were significantly improved (p<0.01) (Fig. 4). The VAS scores and NDI were well correlated with each other (p<0.01). The postoperative VAS scores, NDI, and their changes showed no correlation with any other clinical or radiological parameters.
Radiologic outcomes
Disc invasion and DH change
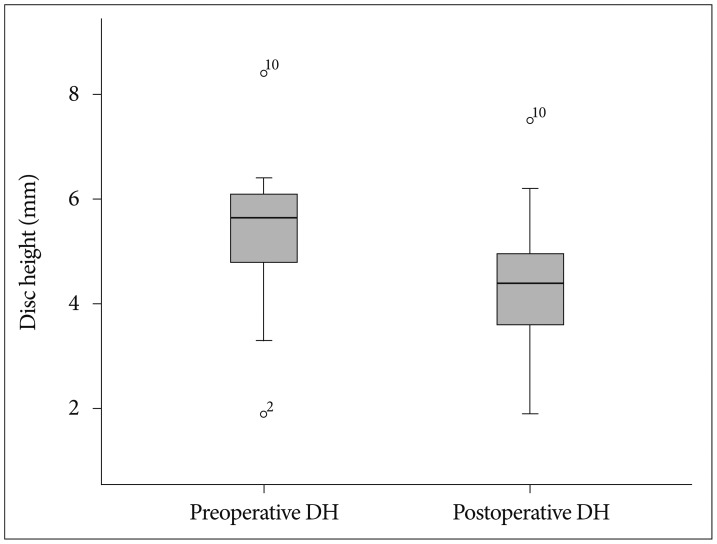
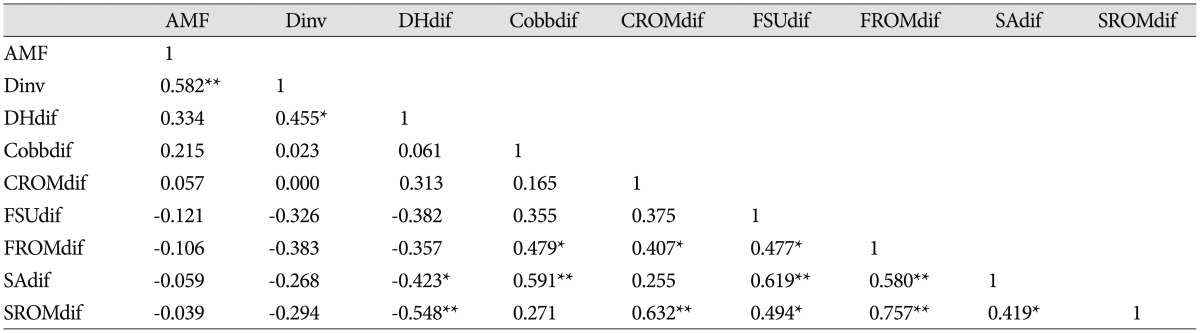
The presence of disc invasion (Dinv) was found in 16 of 24 (66.7%) cases. It was positively correlated with postoperative DH change (p<0.05). The preoperative DH was 5.4 mm (1.9-8.4), whereas the postoperative DH was 4.4 mm (1.9-7.5). The difference between the preoperative and postoperative DH was 1 mm (0-2.4) and was statistically significant (p<0.01) (Fig. 5). Four cases (16.7%) showed no change in DH postoperatively. The DH decrease was negatively correlated with the difference of SA, the postoperative ROM of the Cobb angle, FSU angle, SA, and the postoperative anterior spur (p<0.05) (Table 3).
AMF diameter and DH change
The mean AMF diameter was 5.2 mm (3.2-7.8). The AMF diameter was not correlated with DH decrease or any other change of static angles or their ROM (Table 4).
Static angles (Cobb angle, FSU angle, and SA) and kyphoscoliosis
In the operated segment, the mean preoperative Cobb angle was 12.5 (0.1-26.1) degrees, the mean FSU angle was -1.5 (-9-7.6) degrees, and the mean SA was 4.4 (-2.4-9.6) degrees. The mean postoperative Cobb angle was 11.3 (-15.7-29.7) degrees, the mean FSU angle was -1.3 (-13.5-8) degrees, and the mean SA was -1.3 (-13.5-8) degrees. Only the pre- and postoperative SA showed a significant difference (p<0.05). The postoperative change in the SA was correlated with the changes in DH, FSU angle, and Cobb angle (p<0.05) (Table 4). Kyphotic change in the postoperative Cobb angle, FSU angle, and SA was found in 3 patients (12.5%), 4 cases (16.7%), and 15 cases (62.5%), respectively. There was no visible postoperative scoliosis.
ROM (Cobb angle, FSU angle, and SA)
The mean preoperative ROM of the Cobb angle, FSU angle, and SA were 51.7 (16.6-73.8), 10.7 (1.1-21.2), and 8.5 (0.3-19.5) degrees, respectively. The postoperative ROM of the above-mentioned angles were 47.3 (26.6-78.5), 7.9 (0-16), and 6.4 (0-11.4), respectively. Only the pre- and postoperative ROM of the SA (SROM) showed a significant difference (p<0.05). The pre- and postoperative ROM of the Cobb angle, FSU angle, and SA were well correlated with one another (p<0.01).
Postoperative spur formation at last follow-up
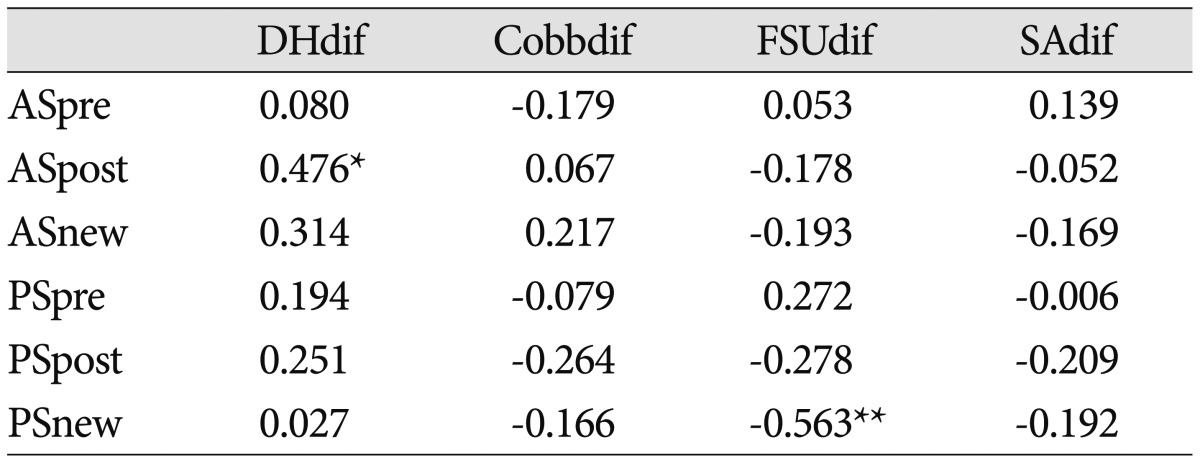
The preoperative anterior spur (AS) was visible in 7 (29.2%) patients, whereas the postoperative AS was visible in 19 (79.2%). Thus, new AS formation was visible in 12 (50%) patients. In addition, the pre-existing AS was aggravated postoperatively. The postoperative AS was correlated only with the DH change (p<0.01).
The preoperative posterior spur (PS) was visible in 11 (45.8%) patients, whereas the postoperative PS was visible in 18 (75%). Thus, new PS formation was visible in seven (29.2%) patients. The postoperative PS was not correlated with the DH change, but was negatively correlated with the postoperative DH. New PS formation negatively correlated with the FSU change (p<0.05) (Table 5).
DISCUSSION
Clinical outcome
The AMF procedure can largely be classified as AMF and 'modified AMF'. Although various surgical techniques may be used, the main concept is formation of a direct path to the pathology around the posterior UP. With the classic transuncal AMF procedure, most authors have reported favorable outcomes in 91-99% of patients1,5,7,8,11). Various modified AMF procedures have shown favorable outcomes in 91-100% of patients2,3,9,13,17,21). In the present series, improvement was found in 91.7% of patients. All patients showed postoperative improvement in VAS and NDI scores. The reported complication rate for this procedure varies between 7% and 22%; however, there were no complications in our series.
Disc degeneration
Minor disc injury may result in acceleration of disc degeneration. Osti et al.16) studied the progression of disc degeneration induced by experimental tearing of the outer annulus in 21 adult sheep with a follow-up of 18 months. They found that inner annulus failure and nuclear degeneration occurred early at 1 and 2 months, narrowing of the disc space followed during the subsequent 18 months, and osteophytes appeared after 4 months. Nassr et al.15) reported a three-fold increase in the risk of developing adjacent-level disc degeneration in incorrectly marked discs in a short-term follow-up. Cuellar et al.4) studied the efficacy of nucleoplasty in 12 patients with cervical pathology; 42% of their patients showed progressive degeneration at the treated level. Several authors2,5) reported that postoperative narrowing of involved disc space occurred until 3 to 6 months after AMF, after then it was unchanged. In our study, disc injury (Dinv) was well correlated with the decrease in DH, which was correlated with decreased SA, postoperative spur formation, and decreased SROM. This indicates that Dinv during AMF may be the trigger of disc degeneration. In our long-term follow-up study, the decrease in DH progressed with time, even after several years.
Changes in static angles
The derangement of normal cervical sagittal angle may induce kinematic changes and accelerate degeneration of the motion unit. Miyazaki et al.14) studied the relationship between changes in the sagittal alignment of the cervical spine and disc degeneration using kinematic MRI in 201 patients. In the present study, kyphotic changes in the postoperative Cobb angle, FSU angle, and SA were found in 3 (12.5%), 4 (16.7%), and 15 (62.5%) patients, respectively. The Cobb angle, FSU angle, and SA were well correlated with one another; thus, a postoperative decrease in SA at the involved segment may lead to segmental and overall kyphotic changes in the cervical spine in some patients. But, in most patients, the postoperative changes of segmental angles may be compensated for by intact facet joints, ligaments, adjacent discs, and cervical musculature6,18,20).
Changes in dynamic angles
Several authors have reported a correlation between disc degeneration and segmental instability10,19). Kirkaldy-Willis and Farfan10) postulated three stages of degeneration : temporary dysfunction, instability, and stabilization. Later, Tanaka et al.19) confirmed this theory. In our series, 75% of patients showed a decrease in postoperative SROM, whereas 25% of patients showed an increased SROM after long-term follow-up. This means that two stages of the degenerative process after AMF are present in our series. The former group demonstrated a restabilized stage of degeneration. The latter could be explained as follows : either the disc degeneration was still progressing or the limited preoperative ROM due to pain was released by successful surgical treatment.
Spur formation of operated level
Segmental mobility may change from a hypermobile to a stable state with a osteoligamentary repair mechanism producing anterior (AS) or posterior osteophytes (PS) according to the progress of disc degeneration10,12). Kumaresan et al.12) performed a biomechanical investigation with a finite element model of the C4-6 cervical spine. They reported that the overall and degenerated segmental stiffness increased with the severity of degeneration. Specifically, the anterior region of the cortex showed a more pronounced increase in these responses. In our study, AS formation was visible in 50% of patients, whereas PS formation was visible in 29.2%. Postoperative AS and PS were correlated only with changes in DH. As disc degeneration progressed, osteophyte formation occurred and/or pre-existing spurs were augmented.
Limitations of this study
The present study has some limitations. Our study was retrospective, and the follow-up interval was relatively variable (6.4-9.8 years). The number of patients was small. In some patients, the surgical, and especially the radiologic, outcomes may not have been the end result. A more uniform long-term follow-up is needed. The types of pathology were heterogeneous. The AMF diameter likely changed with the type and extent of the lesions. The radiologic measurements depended only on the software of our PACS system. The range of error may be not negligible.
CONCLUSION
AMF is an effective technique for treating unilateral cervical radiculopathy in spite of the presence of postoperative disc degeneration. It showed excellent surgical outcomes even in long-term follow-ups. However, a decrease in DH occurred in a considerable number of patients, especially in the presence of disc invasion. Disc invasion during surgery may be the trigger of sequential degeneration.

 XML Download
XML Download