

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pseudoprogression (PsPD) and pseudoresponse (PsR) following anticancer therapy are major areas of controversy in the management of high-grade glioma. In the era of temozolomide, discrimination of PsPD and true progression of high-grade glioma after concurrent radiochemotherapy (CRT) with conventional magnetic resonance imaging (MRI) are extremely challenging. Novel imaging modalities such as MR spectroscopy, positron emission tomography (PET), and perfusion MRI are showing promising results but have yet to be validated in prospective studies. We previously reported the significance of overexpression of p53 for predicting development of PsPD10). In addition to the method of interpretation for early radiologic deterioration, when to determine this is also a critical issue because it affects the clinician's decision making regarding whether to switch to salvage therapy for recurrent disease or to continue planned adjuvant therapy. The timing of defining early progression varies from 4 weeks to 6 months1,4,16,21,24). As PsPD was termed "early necrosis" in early reports, many series determined PsPD at 4 weeks after treatment. Conversely, Wen et al.28) proposed new Response Assessment in Neuro-Oncology (RANO) Working Group criteria for high-grade glioma. An increasing non-enhancing component in T2-weighted and Fluid Attenuated Inversion Recovery (FLAIR) MR images was considered to be progression for patients receiving anti-angiogenic therapy with the new criteria. They also suggested that progression can be true progression only in the cases of recurrence outside the radiation field or in pathologically confirmed cases, if radiological progression is detected within 12 weeks when PsPD is most prevalent. However, further validation would be necessary because this suggestion is not based on a clinical study that demonstrates comparable survival outcome between early true progression (4 weeks after treatment; etPD) and late true progression (progression between 4 and 12 weeks after treatment; ltPD). If the survival difference between etPD and ltPD are significant, early progressive findings should be treated based on the assumption that the lesion would be the recurrent tumor.
PsR is the concept that represents temporary radiological improvement after using an antiangiogenic agent such as bevacizumab while having progression in effect. Phase II trials using bevacizumab and CPT-11 in recurrent malignant glioma have shown a high response rate of 63%, but this encouraging result did not lead to a significantly improved overall survival (OS)11,27). This phenomenon has been proposed to represent the effect of bevacizumab normalizing the permeability of leaky endothelium that causes edema, showing a steroid-like feature.
In the present study, we evaluated PsPD following radiation therapy combined with concurrent temozolomide (TMZ) and also assessed PsR following anti-angiogenic therapy for patients with recurrent disease using criteria of the RANO Working Group.
MATERIALS AND METHODS
Patients
All data from patients diagnosed with World Health Organization (WHO) grade 3 or 4 glioma from March 2005 to February 2011 were retrieved from the archives of the pathologic reports. The clinical and pathologic data of relevant patients were obtained in accordance with the protocol approved by the institutional review board. Fifty-five of sixty-two patients with high-grade glioma who received radiotherapy (RT) with concurrent and adjuvant TMZ were included in the present study.
Treatment
Gross total resection was performed in 16 (29%) patients, subtotal or near total resection was performed in 25 (45%) patients, and stereotactic biopsy was performed in 14 (26%) patients.
The median dose used for radiation therapy was 61.2 Gy (range, 59.4-61.2 Gy) with daily fractions of 1.8-2.0 Gy. Forty-five patients received a total dose of 61.2 Gy in 34 fractions, nine patients received 60 Gy in 30 fractions, and one patient received 59.4 Gy in 33 fractions. The median time from surgery to the initiation of CRT was 26 days (range of 11-77 days).
TMZ concomitant with postoperative RT was administered at 75 mg/m2 a day. For adjuvant TMZ, 150-200 mg/m2 was administered daily for 5 days, every 28 days.
In terms of salvage therapy following recurrence, the surgical resection was performed for the patients who had a small progressive lesion involving non-eloquent area, and gamma knife surgery was reserved for the cases with small lesions and medically inoperable condition. Bevacizumab with or without CPT-11 was considered as a primary option for salvage therapy in all inoperable cases showing true progression. Bevacizumab was used at a dose of 10 mg/kg. The patients who had previous episode of intracranial hemorrhage or who were not be able to afford bevacizumab received nimustine (ACNU)/cisplatin (CDDP) or procarbazine, lomustine, and vincristine (PCV) chemotherapy, or metronomic TMZ.
Assessment of response and statistical analysis
MRI with gadolinium enhancement and T2/FLAIR was performed 1 month after CRT and every 3 months thereafter. When a progressive finding was present, MRI was performed at 2-month intervals. Progression was defined as a more than 25% increase in the sum of the products of perpendicular diameters as in the Macdonald criteria, an increase in the non-enhancing lesion in recurrent cancer with bevacizumab15). Each MRI scan was thoroughly reviewed with a neuroradiologist.
EtPD and ltPD were defined as true progression found at first and second post-treatment MRI with the exception of PsPD, respectively. PsR was scored when progressive enhancement or a non-enhancing T2-weighted lesion was shown right after response to bevacizumab, or after discontinuation of the drug due to toxicity. In some cases, cerebral blood flow (CBF), cerebral blood volume (CBV) values using perfusion MRI, and apparent diffusion coefficient (ADC) maps were used to discriminate PsPD or PsR versus true progression. The Kaplan-Meier method was used for the survival analysis to compare OS between etPD and ltPD.
RESULTS
Patient characteristics
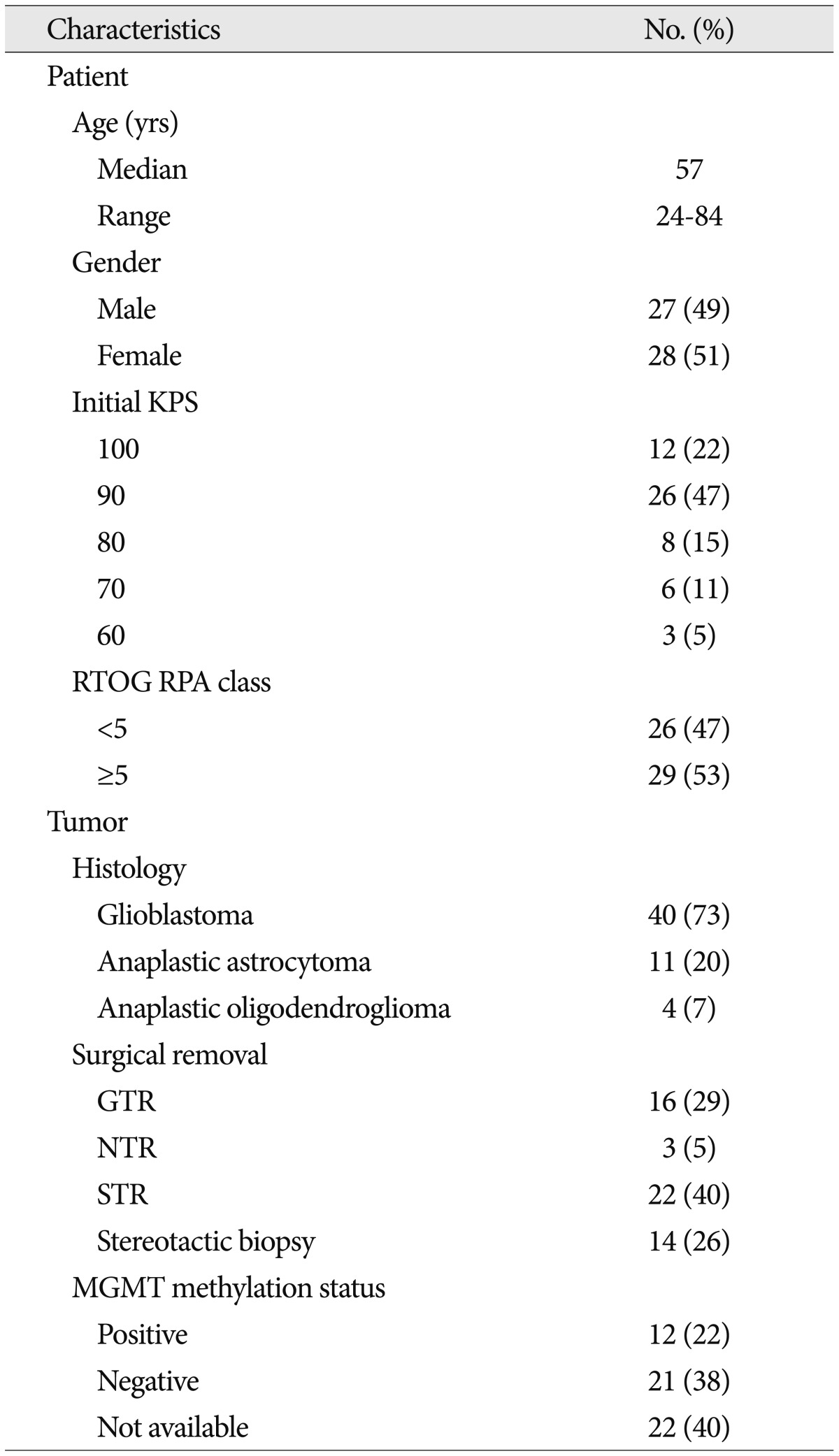
Patient and tumor characteristics are shown in Table 1. Forty (73%) patients were diagnosed with glioblastoma multiforme. All patients were treated with RT combined with concurrent and adjuvant TMZ after surgical resection or stereotactic biopsy. Four patients could not continue adjuvant TMZ due to poor general condition.
Nine (24%) of thirty-seven patients with disease progression during all treatment period and 1 case of PsPD were treated with bevacizumab with or without CPT-11. Surgical resection, gamma knife surgery, ACNU/CDDP, PCV chemotherapy, or metronomic TMZ were also used as an option for the salvage therapy.
In 13 of 55 patients CBV, ADC, or PET were undertaken, and it was insufficient number to analyze the efficiency of the techniques. The exams only provided additional information and were not absolute means of diagnosis.
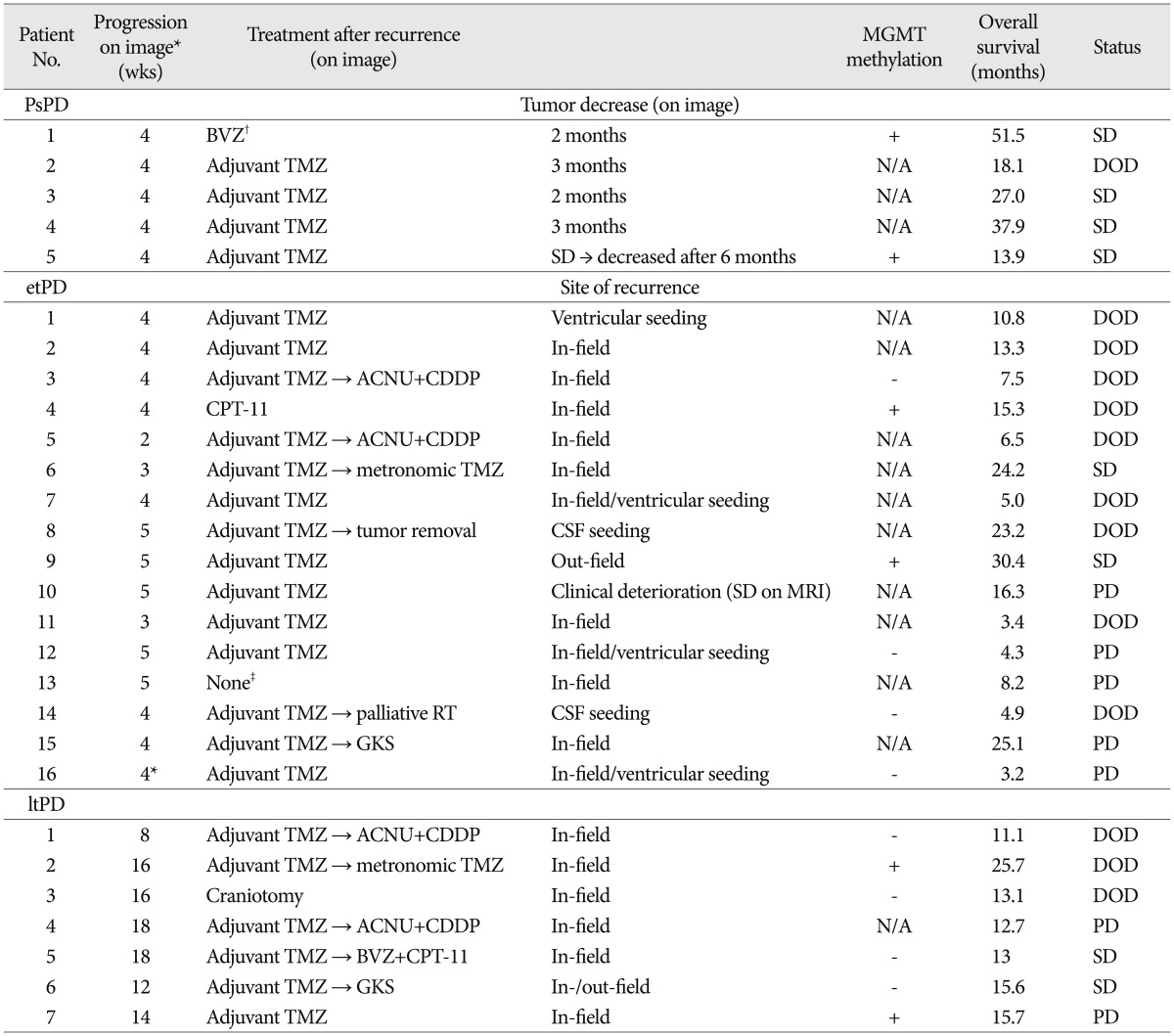
Incidence of etPD, ltPD, and PsPD
At the first follow-up after CRT, 21 patients (38%) showed radiologic progression. And at second post-CRT MRI, 16 (29%) of them persistently showed progression and considered as etPD. Five (9%) of those patients showed progression after the first MRI taken at post-treatment 4 weeks and showed improvement afterwards without specific salvage treatment with a decreasing or stable dose of dexamethasone. These groups of patients were finally categorized as PsPD. And at second post-CRT MRI, 7 showed new progression that was not seen in previous MRI (ltPD). The details of each category are shown in Table 2.
Survival outcomes
The follow-up time was defined as the period between surgery (including stereotactic biopsy) and the last follow-up day or death. The estimated median survival was 25.6 months (range of 3.3-89.7 months). The OS rates at 1 and 2 years were 84.8% and 59.2%, respectively. When divided into WHO grade III and IV gliomas, OS at 2 years were 71.4% and 53.3%, respectively (p=0.125).
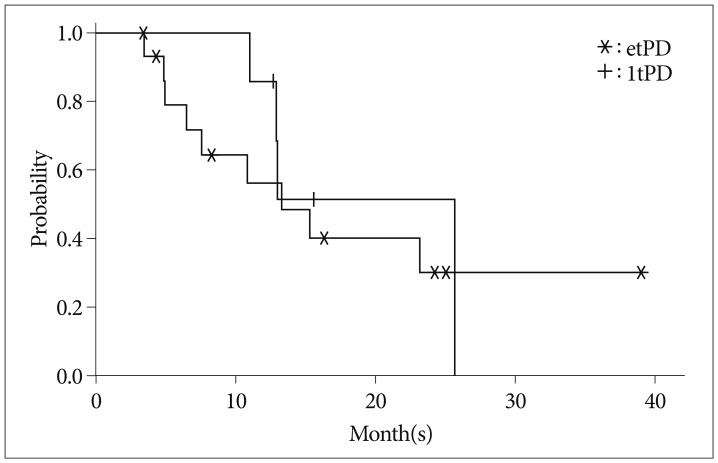
As shown in Fig. 1, the OS of the etPD group vs. ltPD group was 57% vs. 86% at 1 year, and OSs were 30% and 51% at 2 years, respectively. No statistically significant difference was found between etPD and ltPD groups (p=0.595).
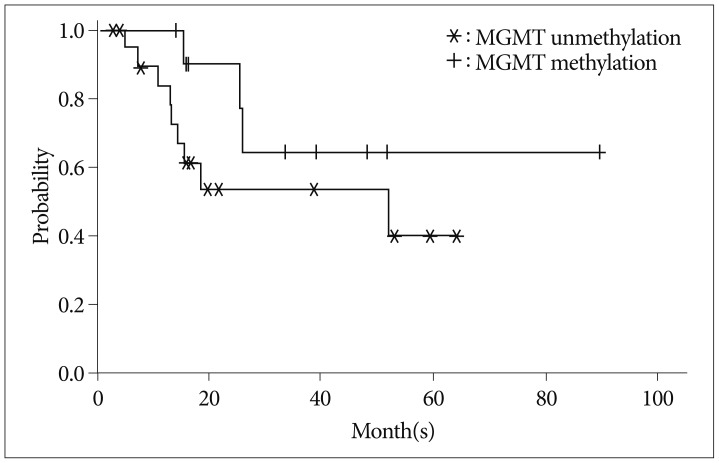
We also performed subgroup analysis in 33 patients having available data for O-6 methylguanine-DNA methyltransferase (MGMT) methylation status. Although there was no statistically significant OS difference between the patients with methylated MGMT and those with unmethylated MGMT (p=0.178), it showed trend toward better survival with MGMT methylation (Fig. 2).
In multivariate analysis using covariates (recursive partitioning analysis, WHO grade, p53 status, MGMT methylation status and extent of resection), none of the factors including etPD and ltPD was related to OS.
The median survivals of treatment with or without bevacizumab, were 10 and 6 months, respectively (p=0.835).
Pseudoresponse
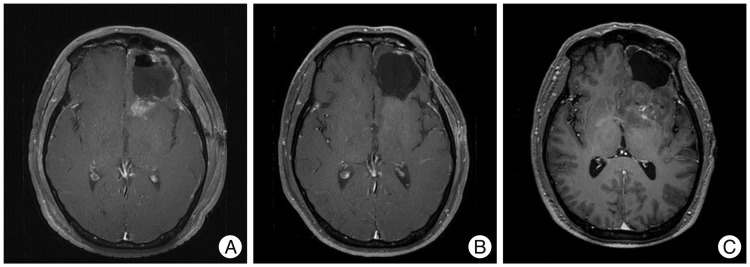
Although 5 (50%) of 10 patients showed a radiological response following salvage treatment with bevacizumab, the response was durable in one case and the stable state persisted for 11 months. The others experienced rapid progression after improvement (Table 3). For one case, the MRI scan showed decreased high T2 signal intensity 1 month after bevacizumab and CPT-11, the lesion showed progression at the subsequent follow-up, and we considered this case to be PsPD. For three other cases, radiologic improvements were shown within 3 months and bevacizumab was continued until thromboembolic events in two cases and cerebral infarction in one case. All showed rapid regrowth of the tumor immediately after discontinuation of bevacizumab on MRI (Fig. 3).
DISCUSSION
The primary goal of this study was to evaluate the survival difference between etPD and ltPD. Thus, we could not identify a statistically significant survival difference between the two groups, indicating that it would be safe to continue planned adjuvant TMZ rather than treatment for recurrence when radiologic progression appears in the first post-treatment MRI. This unique treatment strategy dealing with radiologic progression for high-grade glioma comes from the absence of a diagnostic modality providing high accuracy and resemblance between in-field recurrence and treatment response as PsPD or radiation necrosis. The mechanism of PsPD which is exclusive phenomenon in high-grade glioma, is not clarified, but might be related to the nature of tumor itself. Blood tumor barrier of glioma has high expression of P-glycoprotein, a 170-kDa drug efflux pump protein, which is the main component of blood brain barrier (BBB) and inhibits penetration23). Generally, glioblastoma has compromised barrier that gadolinium can penetrate and shows enhancement. But if the BBB is not altered the lesion presents as nonenhancing tumor. BBB breakage after RT has been well documented but the mechanism is unclear. In vitro study showed that RT induces early transient increase in paracellular permeability while maintaining the tight junction of capillary endothelial cells6). An experimental study revealed that higher exposures of TMZ in brain tumor can also attribute to breakdown of the BBB20). Increased permeability of blood tumor barrier caused by RT and TMZ would result in contrast enhancement due to leakage, which presents as PsPD. PsPD therefore should be defined retrospectively because it mimics tumor progression.
RANO criteria were suggested to overcome the limitation of Macdonald criteria and drew considerable attentions. Although it provides innovative assessment in the treatment of malignant glioma, yet several limitations were pointed out as discriminating true or false lesions in non-enhancing lesions, too simple tumor size measurement, and not reflecting any of new imaging techniques14). Despite current criteria as Macdonald or RANO, purely objective judgement of treatment response only with imaging is difficult in practice. Increased CBV/CBF and a decreased ADC value do not imply progressive disease at all times, however, the decisions are made from these novel imaging modalities for most of the confusing cases. Also, interpreting non-enhanced lesions has raised another dilemma in clinical practices. Latest imaging techniques as dynamic susceptibility contrast MRI perfusion, diffusion-weighted MRI, MRI/PET scans using biomarker, and thallium single photon emission CT are introduced but no comparison under prospective studies have been performed2,13,29). Thus, disparity sometimes in clinical judgment between oncologists and radiologists makes further treatment planning more complex and often needs to be discussed by a multidisciplinary tumor board. Nevertheless, without pathologic confirmation, the possibility of misdiagnosis always exists. For example, one patient who was considered to show PsPD in our last study was confirmed to show true progression by surgery. In this case, CBV was not increased and the tumor demonstrated stabilization after 4 weeks at the second post-treatment MRI, which could be considered to be PsPD. Recently, Vogelbaum et al.26) suggested that retrospective assessments of serial images to distinguish PsPD form true progression and when the finding is ambiguous, the response should be called indeterminate even with RANO criteria. This shows despite the latest techniques and reorganization of the criteria they do not guarantee more reliable diagnosis or appropriate further treatment plan therefore validation should be needed. Retrospective comparative analysis among various criteria has been performed placing emphasis on the nonenhancing tumor8). The major component that we adopted from RANO was the timing of decision making as well as imaging criteria. Appropriate timing is crucial in avoiding the misdiagnosis that would lead to discontinuation or initiation of the effective therapy. Also in Canadian recommendations PsPD cannot be diagnosed until 12 weeks after the end of RT unless new lesion shows out-of-field5). In the review of Sanghera et al.22), timing of defining PsPD varied from 2 weeks to 6 months among 8 studies. Considering that most of the decisions are made at 4 weeks or 6 months in performed studies, it should be confirmed that observation until 12 weeks is not related to decreased OS as in the present study. As our data showed no difference between etPD and ltPD, confirmation after serial observations would be reasonable rather than deciding early from a little information.
Correlation between MGMT methylation and PsPD, and association with improved OS has been reported by Brandes et al.1). In our study, the survival graph comparing MGMT methylated/unmethylated group showed difference but not statistically significant. It might be due to a small size of the available data.
Another crucial debate concerning PsPD is its combined presentation with PsR. As PsPD may reflect increased BBB permeability, administration of bevacizumab under misdiagnosis of true progression normalizes a leaky vasculature and therefore may show a "response"25). It is highly persuasive but only a hypothesis and needs further examination in the future study. In the present study, we observed one case of partial response from bevacizumab. The regression of in-field recurrence occurred 1 month after administration of the drug, and remained stable disease for 11 months. However, as we had impression of both possibilities, true progression vs. treatment related change, we still cannot rule out late PsPD in this case. Others have also reported 2 cases of bevacizumab treatment of symptomatic PsPD17). Counting such cases as the treatment effect may result in a falsely high response rate to an anti-angiogenic agent. As we cannot perform pathologic confirmation in every suspected recurrence, PsPD and PsR should not be considered separately.
Regarding PsR, conflicting views exist concerning interpretation of the response to bevacizumab in recurrent high-grade glioma. As mentioned earlier, a strikingly high response rate and progression-free survival (PFS) does not result in increased OS; thus, doubt exists regarding whether bevacizumab has an antitumor effect. In a pooled analysis by Norden et al.18), a statistically significant increase was found in PFS of patients receiving bevacizumab; however, OS demonstrated no statistically significant difference. In the same context, an argument exists for using PFS as a surrogate for survival12,18).
Bevacizumab causes adverse effects such as intracranial hemorrhage, thromboembolic events, and proteinuria7). In a phase II study of bevacizumab and CPT-11 in recurrent malignant glioma, 4 of 32 (13%) patients had a thromboembolic event and two of them died of toxicity/neurologic deterioration27). We observed three (30%) thromboembolic toxicities that caused discontinuation of the drug. Those cases were all bevacizumab responsive and underwent re-progression shortly after cessation. One possible advantage of bevacizumab is considered to be reduction of corticosteroid use3), but paradoxically it can cause dependency on bevacizumab, which is one of the most expensive drugs. Additionally, bevacizumab can cause VEGF-independent mechanisms of progression in the heavily treated patients18). Furthermore, as glioblastoma is known to be associated with a high risk of thromboembolism, anti-coagulation would be needed to prevent severe complication19). However, not every patient planning to be administered bevacizumab can receive prophylaxis, and thus a positive effect for survival may be countervailed. This life-threatening toxicity cannot be overlooked, and costs and benefits must be considered.
One of the limitations of the current study is showing high OS than other reported data, and this may be due to censored data, as 9 of the patients were unavailable for follow-up9). When recurrence was suspected, salvage treatment varied among patients because until now there is no standard chemotherapy regimen in the management of high-grade glioma.
Although small-sized and retrospective in nature, the present study suggests methodology and evidence for the safety of postponed treatment of recurrent high-grade glioma until 12 weeks after termination of CRT and shows clinical features of PsR, raising a question about the true effect of bevacizumab.
CONCLUSION
Initiating a further treatment plan after 12 weeks as recommended by RANO does not lead to loss of overall survival. Additionally, in recurrent high-grade glioma, bevacizumab must be administered with caution in consideration of PsPD and PsR. However, MRI with gadolinium enhancement alone is not sufficient to characterize tumor response or growth. In addition to clinical correlation with adequate duration of follow-up and histopathologic validation, further studies regarding additional physiologic imaging modalities are required for accurate evaluation of tumor response.

 XML Download
XML Download