

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Aneurysms arising from the internal carotid artery (ICA) trunk have a higher risk of intraoperative rupture with a large defect in the wall due to their very fragile walls and poorly defined necks1,9). Therefore, these aneurysms require special attention.
We reviewed the aneurysm database of our hospital from 2007 to 2012, and found two cases in which we used an encircling clip to obliterate the ruptured ICA trunk aneurysm. We illustrate these two cases and review the repair methods for arterial tearing in the pertinent literature.
CASE REPORT
Case 1
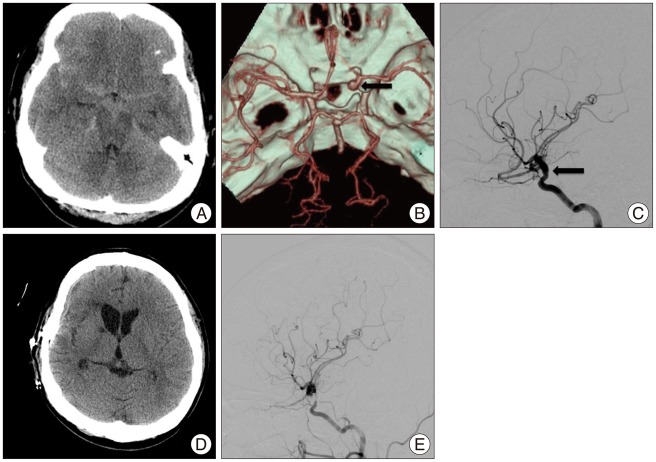
A 38-year-old woman presented with a Hunt-Hess grade 4 subarachnoid hemorrhage (SAH). A 3-dimensional computed tomographic (CT) scan showed no definite saccular aneurysm except for diffuse bulging of the right supraclinoid ICA (Fig. 1A, B). Subsequent digital subtraction angiography (DSA) revealed diffuse bulging of the right ICA (Fig. 1C). The fusiform lesion at the ICA was thought to be the source of SAH; thus, we decided to obliterate the lesion via the wrapping method.
After the removal of the anterior clinoid process and temporary clipping of the proximal ICA, we tried to wrap the aneurysm with a piece of cotton and a fenestrated clip. During clip placement, premature rupture occurred. Because the exact site of the rupture could not be found, we chose the Sundt clip-graft (Codman, Raynham, MA, USA) to stop the massive arterial bleeding. Although we performed sufficient dissection so that nearby perforators would not be involved, we could not avoid the sacrifice of the ICA perforators. Postoperative brain CT scan revealed hypodense lesion in the genu of the right internal capsule. The patient's left hemiparesis gradually recovered and showed a Glasgow Outcome Scale score of 4 by three months after surgery. After sixteen months, follow-up DSA showed stenosis of the right ICA and preservation of distal blood flow (Fig. 1E).
Case 2
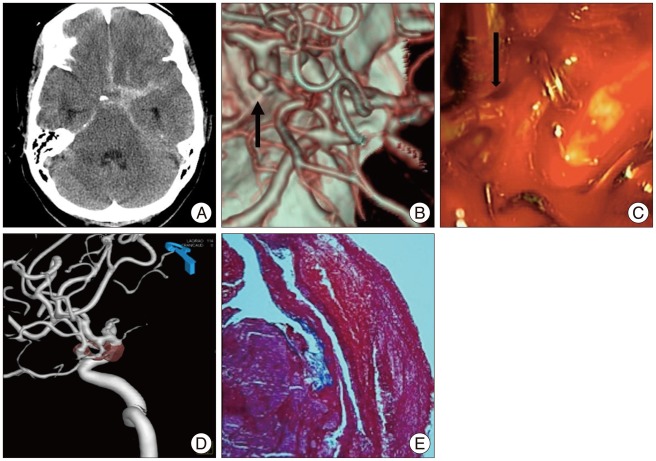
A 46-year-old female presented with a Hunt-Hess grade 3 SAH. Brain CT scan showed thick and diffuse SAH involving the basal cisterns and left Sylvian fissure (Fig. 2A). The subsequent 3-dimensional CT scan revealed a small aneurysm (2.5×2.2 mm) on the posterolateral wall of the left supraclinoid ICA (Fig. 2B).
We found the aneurysm located on non-branching portions of the ICA between the anterior choroidal artery and posterior communicating artery during the course of operation. After temporary clipping of the proximal ICA, we applied a straight clip parallel to the arterial wall. During microdissection of the distal part of the aneurysm, the aneurysm was separated from its base (Fig. 2C). We applied a temporary clip in the distal ICA and the placed the Sundt clip-graft. Intraoperative indocyanine green videoangiography and Doppler were performed; we confirmed the patency of perforators and the ICA. Follow-up DSA showed that the ICA was patent but mildly stenotic from the placement of the Sundt clip-graft (Fig. 2D). Histological examination of the detached aneurysm revealed a pseudoaneurysm with a thrombus and focal organization, indicating that the wall of the aneurysm consisted of neither elastic fibers nor muscular layers (Fig. 2E).
At the time of discharge, the patient showed a Glasgow Outcome Scale score of 5.
DISCUSSION
ICA trunk aneurysm arises from the non-branching site of the ICA. These aneurysms are characterized by a very fragile wall, lack of aneurysm neck, and tendency to avulse with minimal surgical manipulation1,9,10). Also, these are histologically different from saccular aneurysms and are difficult to discriminate from saccular aneurysms on preoperative angiography1,3). Several mechanisms have been proposed including atherosclerosis with hypertension, hemodynamic stress, and dissection9,10). However, the pathogenesis of this aneurysm is not clearly known.
Simple clipping of the ICA trunk aneurysm may be hazardous with a high rate of intraoperative or postoperative rupture. Various therapeutic strategies for the ICA trunk aneurysm have been attempted including surgical wrapping, encircling clip placement, clip placement with wrapping, endovascular coil embolization with or without stents, and surgical trapping with or without bypass1,4,5,7,8,13,15). However, we cannot predict to encounter a case in which unexpected tearing of aneurysm neck during microdissection or after the placement of permanent clip. Also, the bypass or endovascular treatment is not always possible because of limited facility and the patient's clinical condition (rebleeding or inaccessible route for endovascular treatment). Therefore, it is important for a novice neurosurgeon to know various repair methods.
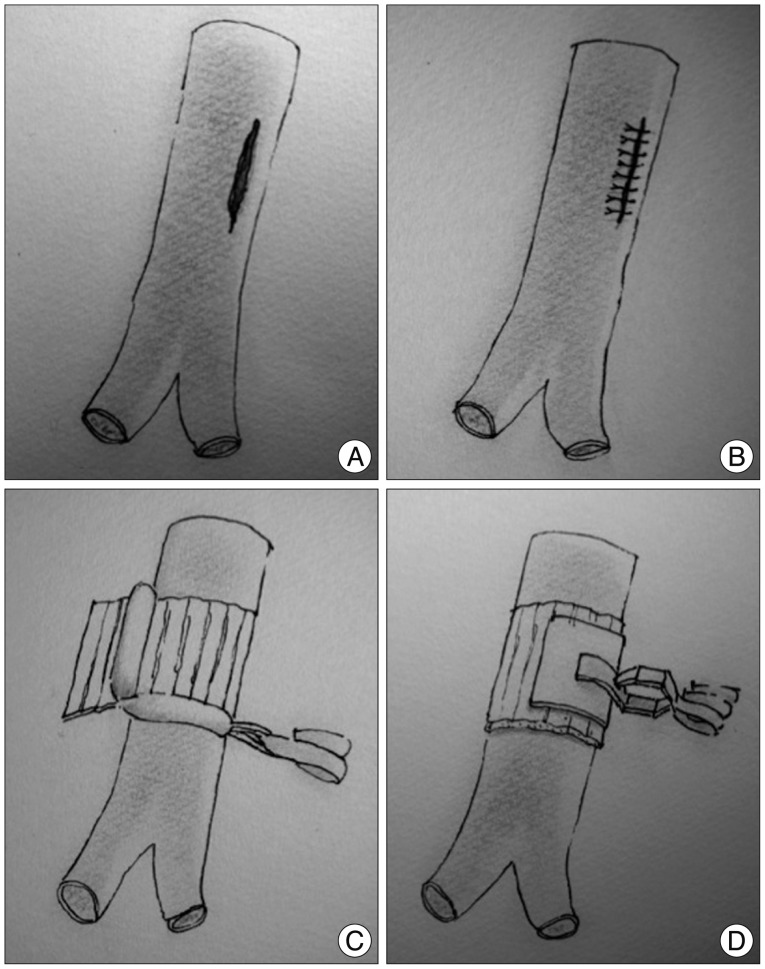
Several methods have been used to repair vessel defects. The suture technique is simple, but takes a long time to achieve occlusion of the parent vessel and is hindered by the position of the vessel and the irregular vessel wall, resulting in stenosis of the defected vessel. A simple method only using a strip of gauze and muscle was introduced, but there is a risk of rebleeding or regrowth of the aneurysm1,14). Other investigators have described a technique using a clip with encircling material such as cottonoid, muscle, fascia, or synthetics. Lanzino and diPierro8) reported a case of a partial avulsion between the junction of the aneurysm and the parent artery in which the tear of the arterial wall was repaired with a clip and a swathe of cotton. Some authors presented a silastic sheet combined with a fenestrated aneurysm clip for emergent hemostasis5). Since the introduction of repair with an encircling clip by Sundt12) in 1967, it provided the neurosurgeon with a rapid non-suture technique for the repair of diseased intracranial vessels. A silastic encircling clip was designed for rapid hemostasis, and there was a report on a technique using sutures covered with surgical and fibrin glue and an encircling clip for repair of a large defect of the ICA4,15). We present schematic illustrations of various repair methods for arterial tearing during aneurysm surgery (Fig. 3).
In our cases, we used the Sundt clip-graft. The advantage or disadvantages of the Sundt clip are explained in the pertinent literature2,6,7,11). There are some issues to take into consideration when applying Sundt clip. It is essential to select the appropriate clip. The barrel diameter 2-5 mm at 0.5 mm intervals and blade length 3, 5, and 7 mm are now commercially available. Therefore preoperative measurement of ICA size is helpful to select Sundt clip in a case of ICA trunk aneurysm. A shorter blade length is recommended to avoid perforator compromise. Also repetitive clipping may occur perforator injury because Sundt clip is bulky. It is needed to identify the patency of parent artery and perforators by Doppler or indocyanine green videoangiography after deployment of Sundt clip. When compromised, reposition of clip or larger barrel size is recommended. In our experience, it is helpful to select a smaller barrel size (till 2/3 of parent artery) for controlling continuous bleeding. And irrigation and waiting are recommended for minor bleeding from Sundt clip rather than clip manipulation. In a retrospective study of 17 patients, the authors reported two complications (50% vessel stenosis and occlusion) after use of Sundt clip and concluded that there was no evidence of increasing stenosis or vessel occlusion over time11). However, long-term follow-up will be needed to confirm this finding. A 3-dimensional CT angiogram or rotational angiogram is useful tool for radiologic follow-up to avoid metallic artifact by Sundt clip, as shown in Fig. 2D.
The standard treatment for unexpected tearing of the parent artery during aneurysm surgery in our hospital is to wrap with cotton threads and to apply a clip parallel to the parent artery including the normal arterial wall. However, this method was impossible due to a large defect and massive bleeding in our cases. The Sundt clip-graft may be a useful alternative for a rapid repair of vessel tearing during aneurysm surgery, especially the ICA trunk aneurysm.
 XML Download
XML Download