

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Unlike adults, traumatic cervical spine injuries are common in the upper cervical spine in children because of the following factors : large size of the head, immature cervical musculature, and horizontal orientation of the facet joints13,16). In addition, the fulcrum of motion is located at the C2-3 region in the pediatric spine unlike in adults where it is located in the lower cervical spine13,16). The cartilaginous end plate between the dens and the body of C2 does not ossify until the child is 5 to 7 years old5,15). Therefore, odontoid synchondrosis fractures are common in young children less than 7 years of age3,5,6,10,11,14,15). Conventionally, the first line of treatment for odontoid synchondrosis fractures in children is immobilization in a halo vest3,6). How-ever, internal fixation is necessary in certain situations7). We report a 10-year-old child with odontoid synchondrosis fracture that was treated by C1 lateral mass-C2 pars screw fixation with a good outcome and discuss the causes for the synchondrosis fracture in this age group and the indications for surgery in this condition.
CASE REPORT
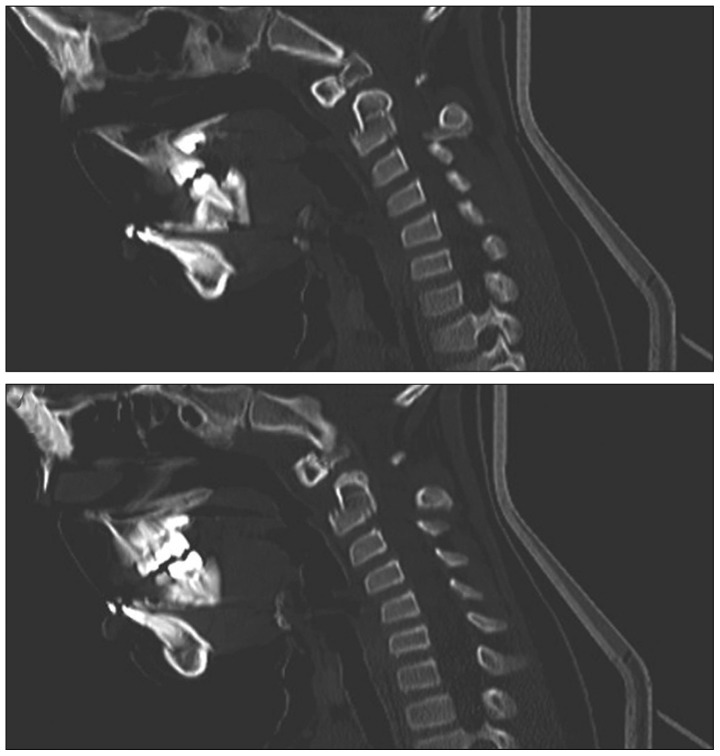
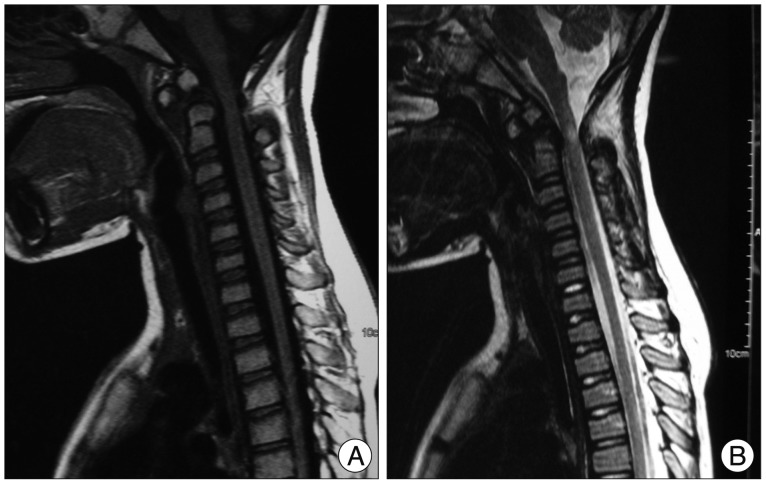
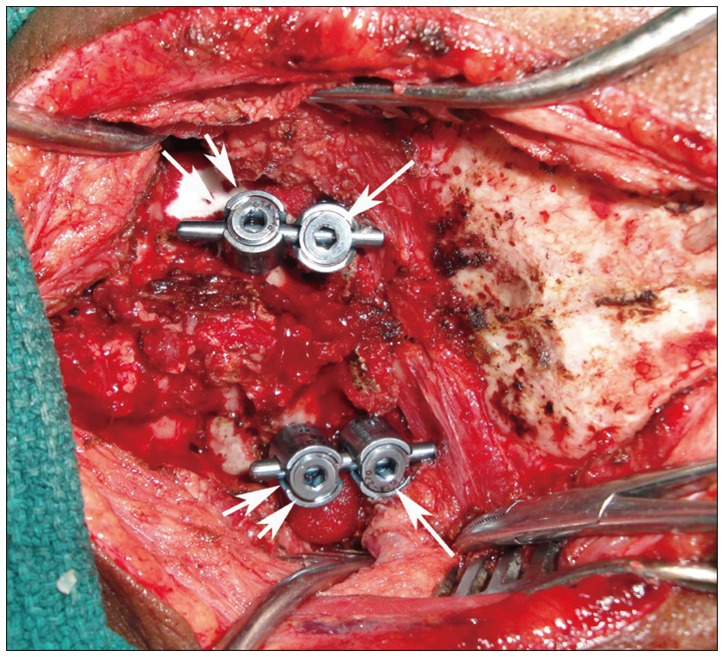
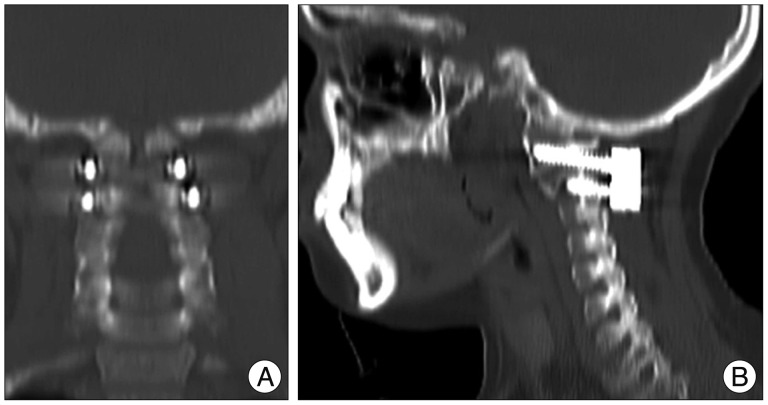
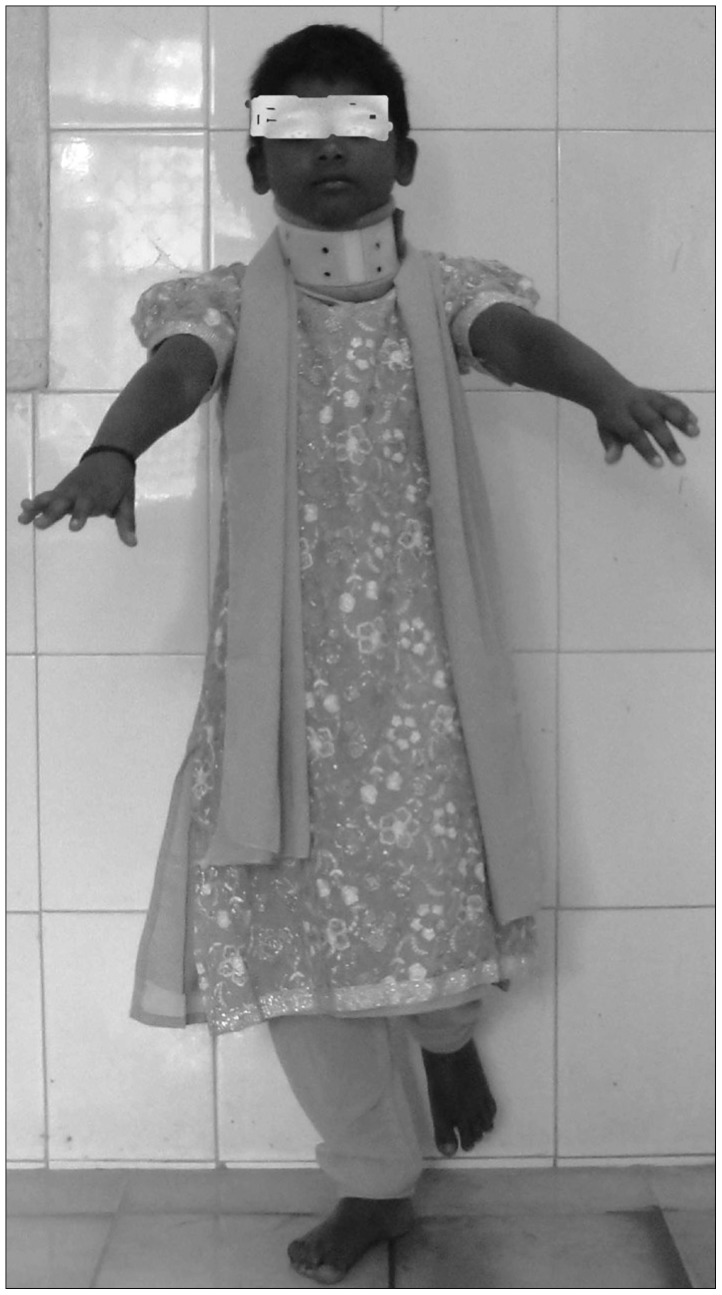
A 10-year-old female child was brought with history of fall from the cot followed by immediate quadriplegia and retention of urine. Examination revealed a conscious child with a GCS score of 15/15. The tone was diminished in all four extremities with grade 0/5 power in both upper and lower extremities. Sensations were diminished below C2 bilaterally. Bladder had been catheterized at an outside institution. Plain radiographs (not shown) revealed a suspicious fracture of the odontoid. CT of the cervical spine showed fracture of the base of the odontoid with posterior displacement (Fig. 1). MRI revealed cord compression at C2 level with intramedullary signal changes (Fig. 2). Patient was immobilized with a Philadelphia collar. In view of the presence of significant neurological deficits and the posterior displacement of the odontoid fragment, it was felt conservative treatment with external immobilization might not be helpful. Hence, C1 lateral mass-C2 pars screw fixation was planned. During surgery, a conventional midline exposure was made. The C2 nerve roots and ganglia were sectioned bilaterally and this revealed a wide open atlantoaxial joint on either side. The joint cartilage was curetted on either side and packed with bone chips obtained from the lower spinous processes. Subsequently, C1 lateral mass and C2 pars screws were placed using standard techniques. After confirming good reduction, rods were contoured and fixed (Fig. 3). Postoperative radiographs revealed good reduction with proper screw placement (Fig. 4). Postoperative CT scan showed proper placement of screws in atlas and axis (Fig. 5). Postoperative MRI was not done. Postoperative period was uneventful. Two months after surgery, patient showed motor power of 4+/5 in all extremities with preserved sensations and intact sphincter control. Six months later she had no neurological deficit and had started attending school (Fig. 6).
DISCUSSION
In children, the axis is divided by the paired neurocentral synchondrosis between the neural arches and the body of axis and the subdental synchondrosis between the dens and the body of axis8). Even though fusion of this synchondrosis usually takes place by 7 years of age4,5,12), it has been documented that this process can be delayed into adoloscence1,2,9). Most cases of odontoid synchondrosis fractures reported till date have been in children less than 7 years of age3,5,8,10,11,14,15). However, the index case reported by us is 10 years old and is the oldest child with synchondrosis fracture reported till date. The reasons for the occurrence of synchondrosis fracture in a child older than 7 years of age are manifold. As mentioned earlier, the fusion of the synchondrosis between dens and body of axis might be delayed into adoloscence2). Amling et al.1) have shown that the thickness of the cortex at the base of the dens is only 35% of the rest of axis and furthermore, there is decreased trabecular bone mass and trabecular interconnection within the base of the dens. Both these factors along with the delayed union of synchondrosis might have contributed to the occurrence of this fracture in this 10-year-old child. Gebauer et al.9) in a histomorphometric study found that the subdental synchondrosis persists in 87% of adult cervical spines. The same authors noted the poor bone integration of the synchondroses in all ages as well as the presence of a residual disc blastema with an average size of 25% of the sagittal depth of the dens9). These studies provide explanations for the occurrence of odontoid synchondrosis fractures in older children.
Role of surgery for odontoid synchondrosis fractures
The first line treatment for most odontoid synchondrosis fractures is often external immobilization6,11,15). Approximately 96% fusion rate is expected with external immobilization alone6). However, surgery does have a role in selected patients with odontoid synchondrosis fractures7). Generally, surgery is an option in patients who fail conservative treatment. Recent literature shows that certain characteristics of odontoid synchondrosis fractures are associated with high failure rate with external immobilization alone7). Fulkerson et al.7) reported that a significant displacement of the odontoid of 11% to 100%, angulation of greater than 30 degrees, clinical evidence of upper cervical spinal cord injury were indications for surgical intervention. In our patient, there was posterior displacement of the odontoid of more than 11% with clinical as well as radiological evidence of upper cervical cord injury and hence our patient had the necessary indications for surgical fixation. The fact that our patient showed significant improvement with surgical treatment indicates that in selected patients with odontoid synchondrotic fractures surgical fixation with C1 lateral mass screws and C2 pars screws is a viable option. In our patient, motion-preserving anterior odontoid screw fixation was not chosen because the fracture fragments were displaced and there was radiological suspicion of transverse ligament injury both of which are indications for posterior C1-2 fixation. Hence, posterior instrumentation of C1-2 was chosen with good results clinically and radiologically.

 XML Download
XML Download