

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Infantile fibrosarcoma is a rare soft tissue sarcoma diagnosed in fetuses, neonates, or infants11). The areas most commonly involved are the extremities, followed by the spine, head and neck3,12). While considered a non-aggressive form of sarcoma, complete surgical resection is rarely feasible at diagnosis. Nearly half of the patients require chemotherapy to reduce tumor size before surgery, and/or to prevent recurrence after surgery3,12). The role of radiotherapy is debated and is mostly reserved as salvage therapy or to preserve the organ function. Metastases have reported in the lung, bones, central nervous system, kidneys, and the eyes15). Unfortunately, surgery is not an option for infantile fibrosarcoma developing in the head and spine due to the high risks of nerve damage. Their chances of survival are considerably lower because they rely on non-invasive therapies.
Spinal metastasis is a common problem among cancer patients, and is generally treated by radiotherapy10). However, application in children and infants is restricted because of the possible late effect of radiotherapy in children including second malignancies, growth disturbance, and other skeletal abnormalities2,14). These problems are due to unwanted irradiation of normal organs remote from the irradiated area. To decrease these undesirable adverse radiation effects, an optimal radiotherapeutic modality which focuses the delivered dose onto the lesions while sparing the peripheral normal tissue is necessary.
Cyberknife® (Accuray Incorporated, Sunnyvale, CA, USA), a stereotactic, linear-accelerator-mounted, image-based system, is capable of delivering radiation with millimetric precision. The high precision of the Cyberknife® allows clinicians to practice hypofractionated radiotherapy, whereby larger doses of radiation are delivered in fewer sessions, and over a shorter period of time, than standard radiation therapy, with minimal risk of peripheral tissues. It is now widely used for the treatment of adult spinal tumors including primary or metastatic lesions of various origins, and the efficacy and safety of Cyberknife® have been widely demonstrated for patients with limited spinal lesions1,5,10). Here, we present a case of infantile fibrosarcoma with spinal metastasis. Cyberknife® stereotactic hypofractionated radiotherapy was used to treat the intraspinal lesion under general anesthesia, and a favorable outcome was achieved without undesirable side effects.
CASE REPORT
A previously healthy 8-month-old boy presented with a 3×3 cm mass in the right lower leg, which was surgically excised. Pathological analysis confirmed the diagnosis of infantile fibrosarcoma and the surgical margin was not clear. His parents refused reexcision but accepted monitoring by regular imaging. However, a mass was detected again in the same area two years after surgery. Therefore, the patient then underwent complete excision, and recurrent sarcoma was confirmed histologically. After the second resection, the patient had monthly follow-up and no evidence of disease was observed on an ongoing one year.
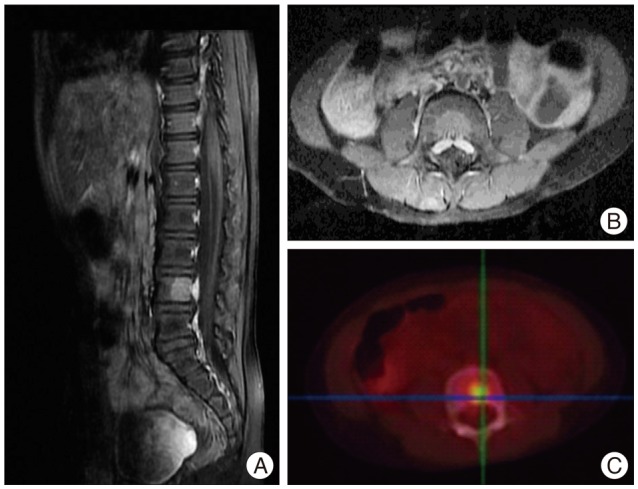
A surveillance whole-body fludeoxyglucose positron emission tomography scan conducted 3 years after the initial presentation demonstrated a recurrent mass in the right lower leg, one micrometastatic lesions at the left proximal fibula and another macrometastasis in the 4th lumbar vertebral column, respectively. Lumbar spine magnetic resonance imaging (MRI) revealed a contrast-enhancing lesion of 1.6 cm in the posterior aspect of the 4th lumbar vertebral column without spinal canal compression (Fig. 1). To preserve right lower leg, debulking surgery of the recurrent lesion was performed, and the histological features were found to be consistent with recurrent sarcoma with rhabomyosarcomatous differentiation. Two weeks after the surgery, the patient started to receive chemotherapy with a VAC regimen composed of vincristine (1.5 mg/m2), dactinomycin (0.045 mg/kg), and cyclophosphamide (2.2 g/m2) for a total of 44 weeks treatment course.
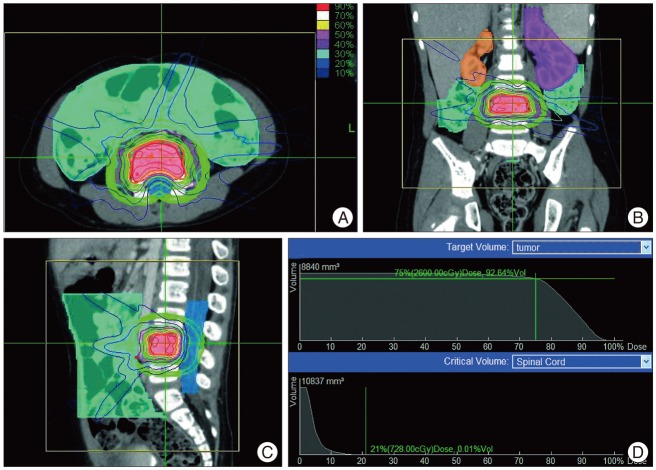
Given the potential risk of spinal pathologic fracture and myelopathy, radiotherapy was chosen to treat the 4th lumbar vertebral metastatic lesion. Cyberknife® hypofractionated radiotherapy was decided due to the solitary nature of the metastasis and fewer sessions are needed, which would decrease the frequency of general anesthesia for radiotherapy. The patient was immobilized in a vacuum mattress. Fused enhanced computed tomography (CT) (Accuray) and MRI scans were used in the treatment planning. The delineation of the gross tumor volume (GTV) and the organs at risk was carried out on the planning CT. Given the potential risk of kyphosis and scoliosis by asymmetric irradiation of the spine, the whole involved vertebra was contoured as the GTV. Clinical target volume was equal to the GTV and no margin was added to obtain the planning target volume (PTV), which was 8.84 mL. No fiducial or other markers were implanted to localize the irradiated area. A total of 26 Gy was prescribed to the 75% isodose line, covering 92.64% of the PTV with a maximal spinal cord dose of 744.26 cGy (Fig. 2). Cyberknife® stereotactic body radiotherapy was performed on the 15th, 16th, 19th, and 20th of October 2009 with a mean procedure time of 83 min (range 56 min to 128 min). The radiotherapy course was conducted in a manner concomitant with the first cycle of chemotherapy. During the radiotherapy, immobilization was aided by general anesthesia, and X-sight spine tracking (Accuray Inc.) was used to minimize setup error.
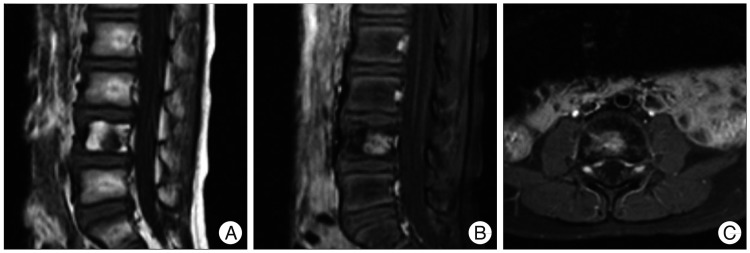
The patient tolerated the anesthesia and immobilization well and remained still during the radiotherapy. Up to the date of this report, i.e., 33 months after radiotherapy, the patient remains neurologically stable and 23% reduction in tumor volume was achieved on the surveillance MRI scans (Fig. 3). No acute radiation toxicity was found.
DISCUSSION
In contrast with adult patients, there is no established consensus about the best management of spinal metastasis in children. Sinha et al.16) presented a retrospective study of 20 children with metastatic spinal disease receiving various treatments including surgery, chemotherapy, radiotherapy and multi-modality combination therapy, and concluded that a standard treatment could not be established for metastatic tumor. Conventional radiotherapy is established as an effective modality for spinal tumors10,15). However, for durable tumor control and in cases of more radio-resistant malignancies, higher-dose radiotherapy may be needed and the radiotherapy is usually precluded by the radiosensitivity of the spinal cord or previous radiation4). Peugniez et al.13) reported the application of conventionally fractionated Cyberknife® radiotherapy (1.8 Gy/fraction) with 25.2 Gy and 19.8 Gy, respectively, in 2 children with recurrent spinal tumor after prior radiotherapy. However, the disease progressed despite the re-irradiation which indicates that conventional radiotherapy may not be efficient for children spinal metastatic tumor. The present case report describes a successful treatment protocol for spinal metastasis combining chemotherapy and high-precision Cyberknife® stereotactic hypofractionated radiotherapy for children diagnosed with infantile fibrosarcoma.
The appropriate dose regimen for spinal radiotherapy for spinal metastasis depends on the primary cancer biology and other factors including tumor location, previous radiotherapy and surrounding critical organs, especially the spinal cord. However, the notable increase in the overall duration of treatment in conventional fractionated radiotherapy hinders the usefulness of radiotherapy in children due to the need for anesthesia during radiotherapy. In contrast to conventional radiotherapy schemes, hypofractionated radiotherapy is attractive because the dose is delivered over a few days and decreases the complexity of the treatment. A variety of fractionation schemes have been used in adult spinal stereotactic radiotherapy with fraction doses ranging from 6 to 30 Gy in 1 to 5 fractions, and rare severe radiation dose-related myelopathy was identified in this range1,5,6). Nevertheless, the tolerability and feasibility of hypofractionated radiotherapy in children is rarely reported and limited to pediatric CNS tumors7,8). To our knowledge, this is the first report of Cyberknife® stereotactic hypofractionated radiotherapy in childhood spinal metastasis.
Each radiation schedule can be converted to biologically effective doses (BEDs) using the following formula and are compared on the same scale, where n is the number of fractions; d, the dose per fraction; and α/β, the alpha beta ratio for irradiated tissue with the BED for spinal cord being 3 (BED3)9).
Gibbs et al.6) reported that limiting the volume of spinal cord treated above a BED3 of 29 Gy to less than 1 mL may decrease the occurrence of radiation-induced myelopathy. Higher radiation tolerance of lumbar spinal cord has been observed in some studies17). However, information from the literature about the tolerance dose for the spinal cord in children is sparse, motivating us to reduce the dose limit by about 50%, i.e., 14.5 Gy in our case. The dose we choose for this patient was 26 Gy in 4 fractions, with the maximal spinal cord BED3 around 12 Gy and a good coverage of 92.64%. With this dose fraction, no severe adverse events was noted during and after treatment over the ongoing period of 33 months.
CONCLUSION
This is the first report of Cyberknife® stereotactic hypofractionated radiotherapy for infantile fibrosarcoma with spinal metastasis. At 33-month follow-up, the patient was still neurologically stable and showed partial response with no acute radiation toxicity. This treatment may thus be a valid option for children with spinal metastasis. However, further clinical experiences and longer follow-up are needed to determine the efficiency and safety of Cyberknife® hypofractionated radiotherapy in childhood spinal metastatic disease.
 XML Download
XML Download