

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Spinal subdural hematomas (SDH) are rare and are known to lead to cauda equina and/or spinal cord compression. In the literature, previous studies have linked spinal SDH to hemorrhagic disorders, trauma, spinal surgery, lumbar puncture or spinal anesthesia, spinal vascular malformations and spinal tumors1,3,5,16). Although the incidence of spinal SDH is quite low, it can occur in the absence of any of the known risk factors. Equally as rare, spinal SDH has been reported to arise as a complication in patients with intracranial SDH2,6,8,10-14,16). Unfortunately, the pathogenesis of simultaneous intracranial and SDH remains unclear. Here, we report a case of intracranial SDH with subsequent spinal SDH, and propose a potential mechanism for the cause of concomitant hematomas.
CASE REPORT
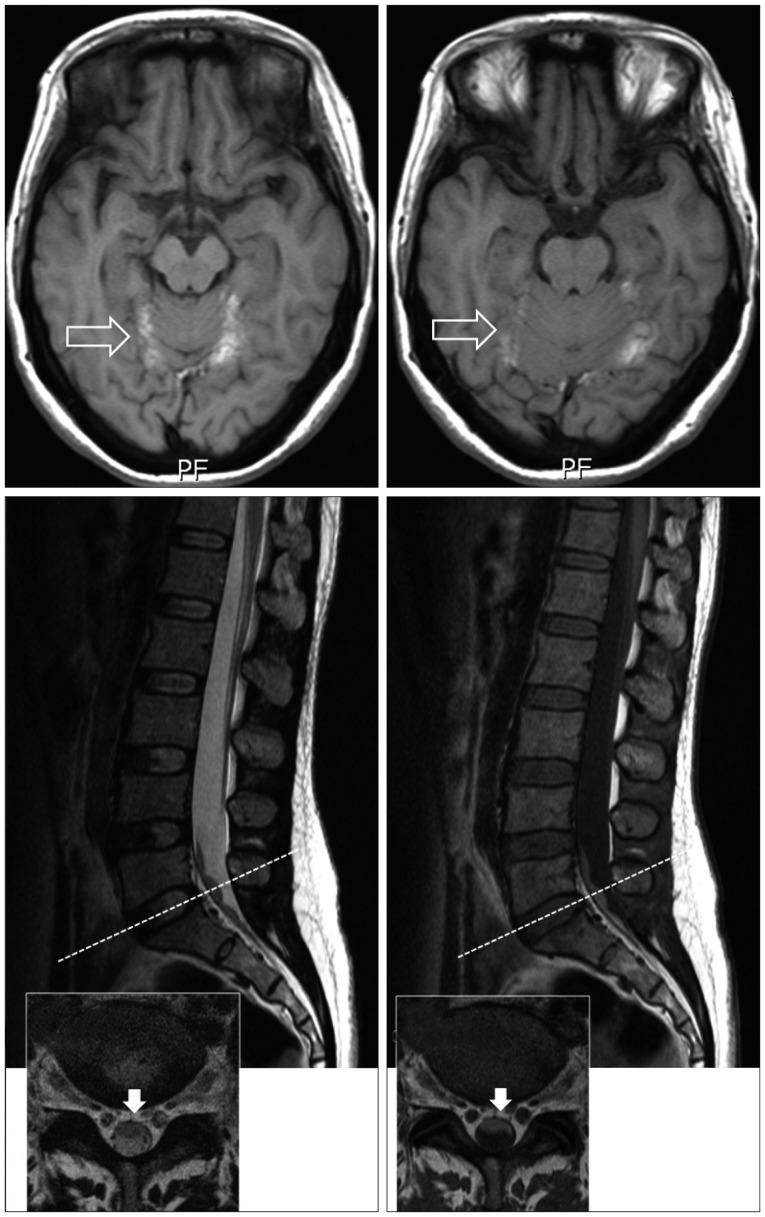
A 47-year-old female patient was referred to our hospital due to sudden onset of headache (visual analog scale; VAS 8) and backaches (VAS 6) following a slip and fall two weeks prior to admission, resulting in periorbital swelling, bruising and a headache. The pain was aggravated by standing and walking and partially relieved by sitting. The patient showed no sensory and motor deficits in lower limbs and there were neither bladder nor bowel dysfunction. She was alert and well oriented, and her spine was aligned normally in the coronal plane with mild loss of lumbar lordosis. Lumbar spine movements in the sagittal plane were restricted by pain. Upon straight leg-raise testing, the patient's leg was able to be raised 60° while lying down, with no neurological deficits noted in the limbs. The cervical spine was normal. There was no evidence of cranial nerve palsy or lateralizing neurological deficits. She had no previous history of anticoagulant therapy and hematological coagulopathy. Her coagulation profiles including platelet count, prothrombin time, and activated partial thromboplastin time were all within the normal ranges. Cranial imaging studies revealed a small amount of acute SDH along the tentorium (Fig. 1). Magnetic resonance imaging of the patient's lumbosacral spine revealed spinal SDH at the anterior portion of the caudal thecal sac at the levels of L5-S2 with marked neural compression (Fig. 1). No definite contrast enhancement at the lesion site was observed. The remaining intracranial structures and cervicothoracic spine were normal. Based on radiologic findings, traumatic intracranial SDH at the tentorium with subsequent spinal SDH was diagnosed. Seven-day course of conservative management was uneventful, and the patient experienced no neurological deficits, without notable event. Her complaints of headache and back pain were nearly resolved, and the patient returned to normal daily activities. At one-year follow-up, the patient was free of leg pain, but complained of a sustained mild headache. Follow-up imaging studies showed no definite abnormalities in the cranium or spine.
DISCUSSION
SDH following cranial subdural hematoma is extremely rare, with only a few cases having been reported previously2,6,8,10-14,16). The pathogenesis of traumatic SDH following intracranial subdural hematoma is difficult to explain in the absence of any violation of the dural layer. Unlike the intracranial subdural space, there are no bridging veins running in the spinal subdural space10). Therefore, the true pathogenesis of SDH remains obscure.
Spinal hematomas may migrate from a cranial lesion, a view that has been supported by many authors15). Lecouvet et al.11) explained that the propagation of blood from cranial to spinal subdural space is possible due to the presence of anatomic continuity between them. The authors of several reports also have described the spontaneous resolution of acute intracranial subdural hematoma. When this occurs, redistribution of subdural blood is often observed with layering along dependent areas such as the tentorium. In view of the presented patient's history of a dramatic resolution of an acute intracranial subdural hematoma with redistribution of blood, we hypothesize that the development of SDH might have been related to a progressive migration of subdural blood to the most dependent areas of the lumbosacral region under the influence of gravity. In other words, the hematoma may have attained a liquefied form and migrated through the subdural space14,16). This theory is supported by previous electron microscopic observation of an anatomical continuity between the intracranial and spinal subdural space7). The continuity between the intracranial subdural space and that of the spine has thusly been proven. In a previous study, Haines et al.4) examined the dura-arachnoid junction at an electron microscopic level and demonstrated that although the external dural layer is strong, the inner dural or meningeal dural layer is structurally weak and vulnerable to injury. Under normal conditions, there is no space at the dura-arachnoid junction. When pathologic or traumatic processes occur, the space is identifiable. For this reason, this space has been deemed "potential space". Shrunken brain due to trauma may open this "potential space" and allow fluid to collect in this space. If fluid collection continues, it may be gravitationally pulled downward along the potential space of the spine9). This process may also damage the small anastomosing network of extremely delicate spinal dural vessels, so that a symptomatic hematoma may then be formed. The spinal subdural space comprises a small anastomosing network of extremely delicate vessels, which are directed longitudinally along the lateral margins of the dura mater. However, their extremely small sizes hinder them being a source of hemorrhage.
It is generally agreed that prompt laminectomy with evacuation of the hematoma should be performed before irreversible damage to the spinal cord occurs. However, including our patient, ten of the twenty cases reported in the literature demonstrated a benign course along with spontaneous resolution of thoracic or lumbar subdural hematoma with conservative treatment. Accordingly, an operation should only be considered for cases involving progressive neurologic deficits or persistent symptoms.
CONCLUSION
SDH may be concomitant with or may occur after intracranial subdural hematoma. Although the exact pathogenetic mechanism and prevalence is not certain, we hypothesize that the occurrence of SDHs might be related to a progressive migration of subdural blood to the most dependent areas of the lumbosacral region under the influence of gravity. In other words, the hematoma may attain a liquefied form and migrate through the subdural space. Accordingly, in patients with intracranial subdural hematoma complaining of lower back pain and weakness in both legs, lumbosacral MR examination should be performed to exclude the coexistence of SDH.
 XML Download
XML Download