

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tapia's syndrome, first described in 1904 by the Spanish otorhinolaryngologist G. A. Tapia, includes two distinct conditions, differing in clinical manifestation and pathophysiological mechanism. The central Tapia's syndrome is a typical crossed brainstem syndrome caused by a lesion of the nucleus ambiguus, the nucleus of hypoglossal nerve and the pyramidal tract5). The peripheral Tapia's syndrome is due to the extracranial lesion of the recurrent laryngeal branch of the vagus nerve and the hypoglossal nerve9). But in most publications about this syndrome, the peripheral Tapia's syndrome was described. Peripheral Tapia's syndrome is a rare complication of anesthetic airway management. Main symptoms are hoarseness of voice and difficulty in tongue movement. Upon neurological examination, the patient typically shows an ipsilateral paralysis of the vocal cord and tongue. But Sotiriou et al.8) reported a case of postoperative airway obstruction after coronary bypass grafting surgery due to bilateral Tapia' syndrome. To our knowledge, no report has been published or given an explanation for Tapia's syndrome after posterior cervical spine surgery.
We report two cases of peripheral Tapia's syndrome after posterior cervical spine surgery in general anesthesia.
CASE REPORT
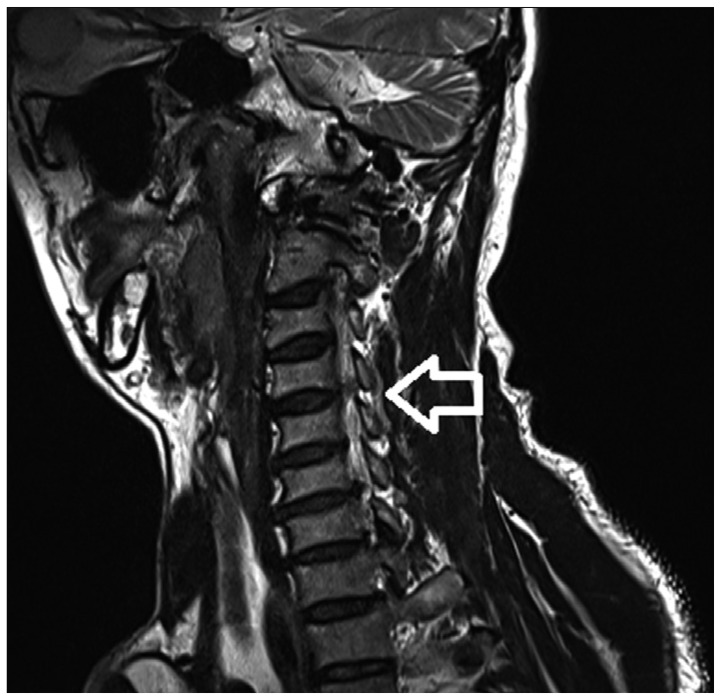
The patient of first case is a 53-year-old man who presented right shoulder drop and right shoulder pain. On motor examination, weakness of 0/5 right in shoulder abduction was found. Magnetic resonance imaging revealed C4/5 foraminal herniated nucleus pulposus (Fig. 1). The patient was placed in the concord position under general endotracheal anesthesia and the head was secured in the Mayfield head clamp. The patient underwent a posterior foraminotomy with discectomy. Immediate postoperatively, weakness of right shoulder abduction was improved from 0/5 to 3/5. On postoperative day 1, he complained of hoarseness, hypesthesia of left side tongue, buccal cavity and deviation of the tongue to the left during protrusion. There was no definitive lesion in postoperative brain magnetic resonance imaging. In laryngeal electromyography with 37 mm monopolar needle, there was no motor unit action potential on left thyroarytenoid muscle which is innervated by the recurrent laryngeal branch of the vagus nerve. Six months after surgery, symptoms were resolved.
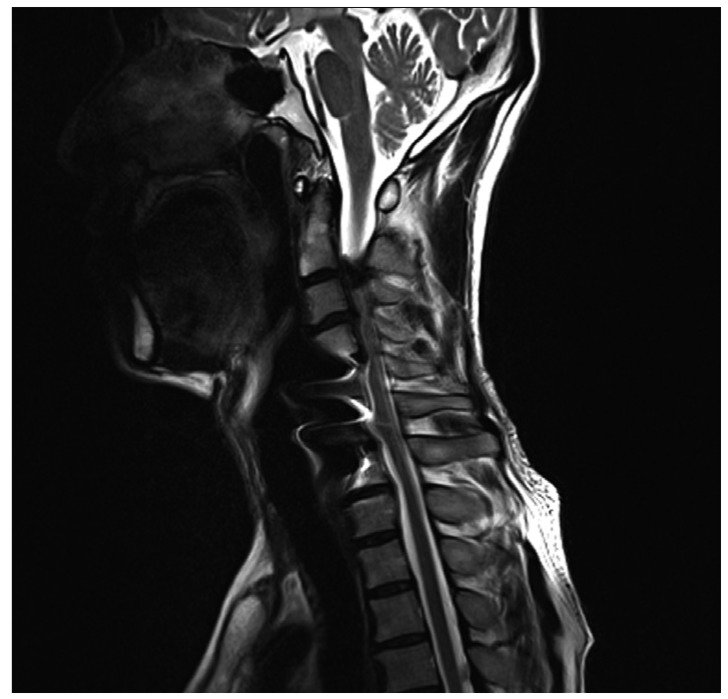
The patient of second case is a 56-year-old man who presented gait disturbance. Fifteen years prior to admission, he had a cervical injury from a traffic accident and underwent C5/6 anterior cervical discectomy and fusion. On neurologic examination, ankle clonus was found. Magnetic resonance imaging and computed tomography revealed spinal stenosis on C2/3/4/5 and ossified yellow ligament in right C2/3 (Fig. 2). The patient was placed in the concord position under general endotracheal anesthesia and the head was secured in the Mayfield head clamp. He underwent right C2 hemilaminectomy and C3/4/5 laminoplasty under general anesthesia. Surgery was uneventful. Postoperatively, he complained of hoarseness, hypesthesia of left side tongue, and deviation of the tongue to the left during protrusion. On postoperative day 4, all symptoms except hoarseness were resolved. Two months later, hoarseness was also completely resolved.
DISCUSSION
Concomitant paralysis of the hypoglossal and recurrent laryngeal nerves can be caused by lesions affecting the lateral wall of the lower part of the oropharynx and the upper part of the hypopharynx where the hypoglossal and vagus nerves are in close proximity6). There are many causes of Tapia's syndrome, including general anesthesia (septorhinoplasty10), coronary bypass8), shoulder surgery2)), metastatic hemangiosarcoma5), carotid artery aneurysm7), fungal infection4), neurofibroma of vagal and hypoglossal nerves1). However, most of them are due to general anesthesia. Yavuzer et al.11) described a case of Tapia's syndrome after septorhinoplasty as a consequence of nerve compression after inflation of the cuff within the larynx. Boisseau et al.2) reported a case of Tapia's syndrome after general anesthesia following shoulder surgery. The syndrome, in their case, was believed to be due to a compression by the endotracheal tube, caused by the displacement of the head2). Lykoudic et al.6) reported a case of Tapia's syndrome after general anesthesia following rhinoplasty. They believed that throat packing, which is applied in hypopharynx and lower oropharynx, facilitated compression of the nerves upon the tracheal tube and the pharyngeal wall3).
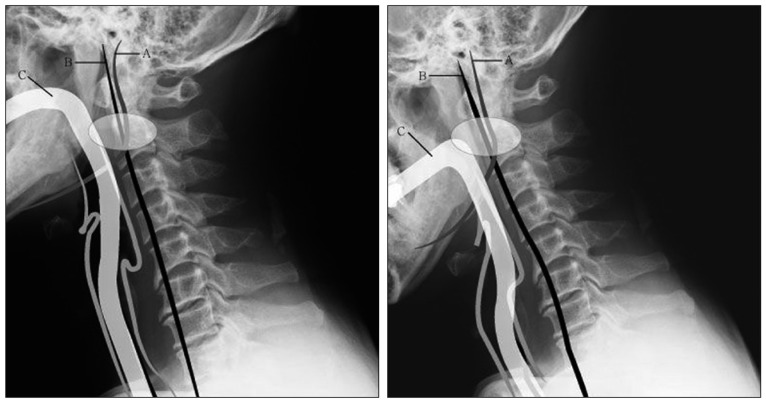
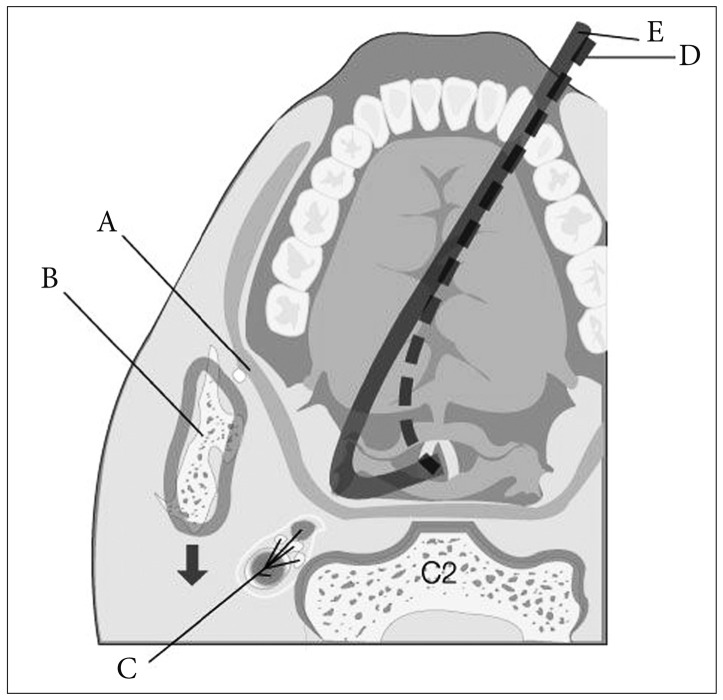
To our knowledge, our cases are first reports of Tapia's syndrome after posterior cervical spine surgery. The causes for our cases have not been confirmed. There was no direct anatomical relation between the operation, the vagus nerves and the hypoglossal nerves, and there was no record of displacement or malposition of the endotracheal tube. Considering the causes of aforementioned cases in the literatures, we hypothesize that additional neck flexion for surgical exposure may have caused the endotracheal tube to offend the lateral wall of oropharynx and hypopharynx where the two nerves are in close proximity. The more the neck is flexed, the more the endotracheal tube is bent within pharynx. So, when the neck is flexed excessively, convexity of the bent endotracheal tube within the pharynx may compress the pharyngeal wall. Because the endotracheal tube is fixed on only two terminal points in general anesthesia, mouth with taping and trachea with ballooning, the middle convexity of the bent endotracheal tube may move freely in the pharynx. The middle convexity of the bent endotracheal tube may deviate from midline and offend the lateral wall of the oropharynx and hypopharynx where the two nerves are in close proximity. Besides, when the neck is flexed excessively, ramus of mandible moves closer to the cervical spine and the two nerves (Fig. 3). In this situation, the two nerves may be entrapped amid the offending endotracheal tube, the ramus of mandible and transverse process of cervical vertebra (Fig. 4). Therefore, excessive neck flexion may facilitate compression of the nerves upon the endotracheal tube and the pharyngeal wall like the throat packing did in case of Tapia's syndrome after rhinoplasty6).
Fortunately, the mechanism of nerve injuries in cases of Tapia's syndrome following anesthesia and surgery is known as neuropraxia. Most cases in literatures heal within 4 to 6 months3). For treatment of Tapia's syndrome, Boga and Aktas3) recommended corticosteroid as the key drug. However, this should be used with discretion. They recommended only follow-ups for mild cases3).
CONCLUSION
Tapia's syndrome is a rare complication which every surgeon must nonetheless be aware of. To avoid this problem in posterior cervical spine surgery, we suggest paying special attention to the position of the endotracheal tube to avoid excessive neck flexion before and during the positioning of the patient.
 XML Download
XML Download