

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Split cord malformations (SCMs) are rare congenital anomalies in which the cord is split over a portion of its length to form a double neural tube in a single dural sac2,5,16,20).
SCMs associated with a split of the spinal column, spinal bony spurs, myeloceles, myelomeningoceles, lipomas, and dermal sinuses have been reported in the literature10,12,13,22).
SCMs and other associated anomalies are rare within the general population. It is more uncommon for the initial clinical presentations to occur in adulthood4).
We report a rare case of cervicothoracic SCM with spina bifida and tethered cord syndrome due to the thickened filum terminale in adult and discuss the anatomical and embryological relationship of the level of the fibrous septum and duplicated level of the spinal cord.
CASE REPORT
History and examination
A 34-year-old woman was admitted with neck pain, back pain, and recurrent bilateral leg weakness of 2 months duration. On physical examination, there was a paresis with 4/5 muscle strength and deep tendon hyperreflexia in both legs. There were no pathologic reflexes. The initial neurologic evaluation revealed sensory numbness below the level of the C-7 dermatome. An urodynamic study, somatosensory evoked potentials, and electromyograhic evaluation showed no abnormalities.
Neuroimaging findings and treatment
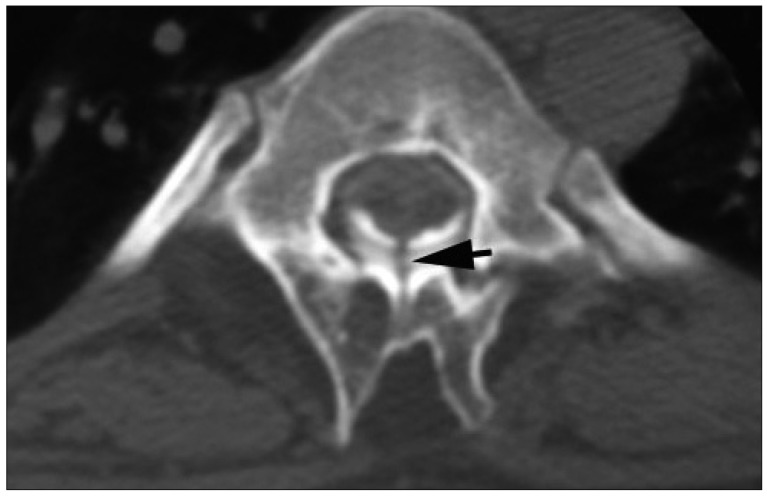
The radiologic examination revealed mild scoliosis of the thoracic spine, hemi-vertebrae at T6 level, and butterfly vertebral bodies at T11 level. Spina bifida was also present. The admission cervicothoracic MRI showed that the spinal cord was divided into two segments from the level of C-7 to T-11, and there was development the subcutaneous fat within the bifid spine. No fibrous septum was demonstrated on MR imaging. On lumbosacral MRI, the conus was shown to be low-lying, ending at the L5 level (Fig. 1). CT myelography showed that dye was leaked incidentally into the epidural and intradural spaces. A fibrous septum divided the spinal cord and extended to the epidural space and attached to the ventral cortex of the lamina at T9 level (Fig. 2).
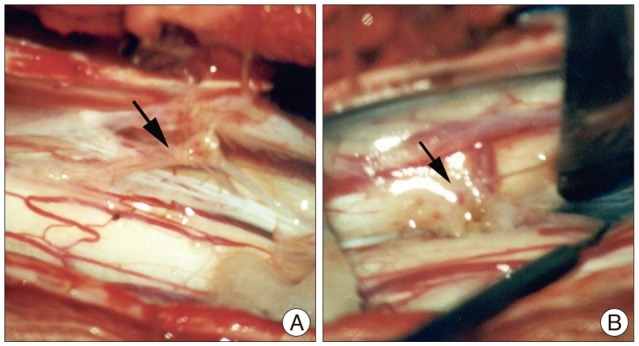
The patient underwent surgery to prevent progression of the neurologic damage resulting from tethering of the spinal cord. A laminectomy was performed from the level of T-8 to T-11. The T-9 and T-10 spines were bifid and abnormal fat tissue was infiltrated between the bisected spinous process. Surgery revealed a symmetric duplication of the spinal cord above the level of T-10, which was encompassed by a single dural sac, and the fibrous septum was recognized between the divided hemi-cord at the T-9 level, 10 mm above the cord reunion site (T-10). The fibrous septum splits and tethers spinal cord. The tethered spinal cord was released by resection of the fibrous septum (Fig. 3).
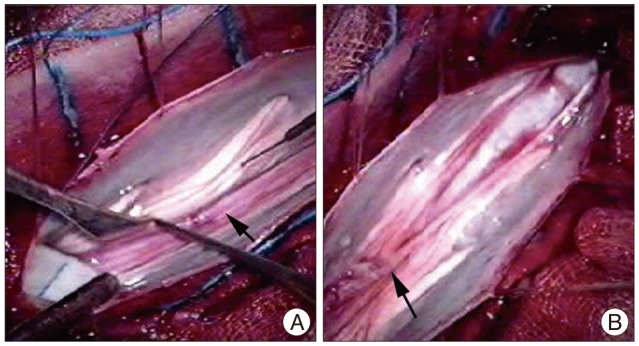
Afterwards, a L5 and S1 laminectomy was performed to release the tethered cord syndrome by the thickened filum terminale21). The nerve roots appeared slightly adherent to the dura at the L-5 level, and resection of the thickened filum was made because the cord was tethered at the level of the lesion (Fig. 4). The patient had an uneventful postsurgical recovery.
DISCUSSION
SCM is a rare spinal anomaly that refers to a longitudinal division of the spinal cord into two divided hemi-cords6,11). This malformation has been reported to be associated with a split of the spinal column, spinal bony spurs, myeloceles, myelomeningoceles, lipomas, and dermal sinus15,16).
SCMs are often located in the lumbar and thoracolumbar regions. Sinha et al. reported the incidence rates for cervical and cervicothoracic locations as 3% and 1%, respectively21).
Symptoms related to congenital anomalies occur most commonly in childhood, so SCMs were initially regarded as a pediatric problem; but in many patients the diagnosis is not established until symptoms manifest in adulthood1,9,18,19).
Embryologically, the spinal cord is formed by the integration of two paramedian notochords along the midline17). When this integration is defective, a SCM can develop.
SCMs are classified as one of two types, according to the unified theory : in type I SCM, the hemi-cords are always invested with individual dural sacs and the medial walls of the sacs always ensheath a rigid (bony or cartilaginous) midline spur; and in type II SCM the hemi-cords are always within a single dural sac and the midline septum is always composed of non-rigid fibrous or fibrovascular tissues16,17). Based on this classification, our case can be classified as type II because the spinal cord was divided by a fibrous septum at the level of T-9.
An interesting finding of this case was the relationship between the anatomic location of the fibrous septum and the level of duplication of the SCM. Embryologically, SCM is caused by a primary neurulation defect. According to the unified theory of embryogenesis proposed by Pang et al.17), an abnormal communication (endomesenchymal tract) between the ectoderm and endoderm causes regional splitting of the notochord, and each separated notochord induces the surrounding paraxial mesoderm and subsequent dysgenesis of the spinal cord. Thus, the level of the fibrous septum and duplicated level of the spinal cord should be similar. However, the fibrous septum was located farther above the level of the spinal cord duplication in this case. It might be because this case was associated with a thickened filum terminale. A low-lying conus and thick filum terminale are related to abnormal retrogressive differentiation of the secondary neural tube with failure of terminal cord involution7,17). The thickened filum terminale fixed conus and relative ascent of the spinal cord was not complete. This embryologic background could be the basis for the fibrous septum located proximal to the level of the spinal cord duplication in this case. And also, anatomical location of the fibrous septum and level of cord duplication of this case could delineate the sequence of spinal cord development.
This anatomic relationship might be helpful to identify the fibrous septum to detether type II SCM patients associated with thick filum terminale. Associated skeletal dysgenesis such as spina bifida, hemi-vertebrae, or a laminar defect might also be helpful to decide the level of detethering surgery.
An awareness of the presence of associated congenital anomalies is surgically important to improve postoperative outcomes and to determine surgical priorities3,8,22) For example, if the SCM is accompanied by a thickened filum terminale, the septum should first be excised to release the cord. Otherwise, the abruptly released cord will suddenly be pulled upwards, resulting in spinal cord injury below the level of the SCM14).
CONCLUSION
Unlike pediatric patients, adult-onset SCM may present without neurocutaneous or overt skeletal abnormalities. A thorough evaluation of associated anomalies is mandatory to make a therapeutic plan for patients with SCM. Although it is rare, careful preoperative examination and refined microsurgery may provide good outcome for the patient.

 XML Download
XML Download