

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The management of pathologic lesions located at or close to the anterior and middle skull base may require the removal of the anterior clinoid process (ACP) to achieve proper neurovascular control during the surgical procedure3,9,17). Owing to the deep location of the ACP and the complexity of the anatomical structure around it, anterior clinoidectomy requires precise knowledge of the anterior and middle skull base neuroanatomy. At present, because neurointervention techniques and radiosurgery have replaced skull base surgery around the ACP, opportunities to remove the ACP haves dwindled. However, anterior clinoidectomy is an essential technique when removing parasellar tumors or clipping paraclinoid aneurysms, for instance.
Since Dolenc7) introduced the extradural technique of complete anterior clinoidectomy, other safe techniques and their tremendous advantages have been introduced in many articles3,5,14,16,18,19,21). However, articles about the morphometrical benefit from anterior clinoidectomy are rare, and the research performed in Korean is even more rare12,15).
The purposes of this study were to quantify, with direct measurement, the length of the optic nerve and the internal carotid artery (ICA) before and after extradural anterior clinoidectomy and to measure the height and basal width of the ACP, as well as other critical landmarks around the ACP in Korean adults.
MATERIALS AND METHODS
Eleven 10% formalin-fixed Korean adults (6 men, 5 women) cadaver heads were examined for a total of 20 sides, excluding two damaged sites. Specimens were placed on a handmade headrest and positioned for a frontotemporal approach. A large frontotemporal approach was performed. The temporal muscle was tractioned toward the zygomatic arch after interfascial dissection. Craniotomies were done using a high-speed electric drill (Midas Rex, Legend). Microanatomical dissections were performed with a surgical microscope (Zeiss Contraves; Zeiss, Inc.). Parts of frontal and temporal lobe were removed for precise measurement. At first, all data were gained by scientific divider and then calculated using a digital caliper in units of 0.01 mm. All measurements were made by a single investigator.
Measurement before anterior clinoidectomy
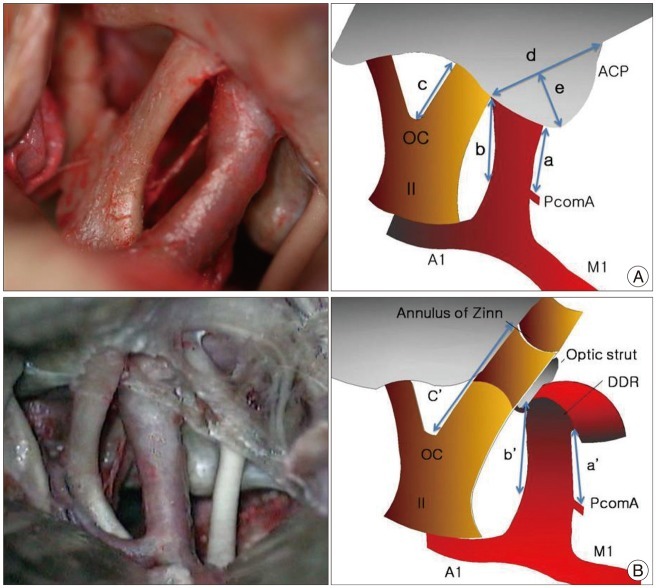
For convenience during the investigation, the frontotemporal lobes were partially removed. According to the Bouthillier et al.2) classification of the ICA, the C6 (ophthalmic) segment of the ICA was measured. The lateral length of the C6 segment, from the most proximal visible point where it was covered by the ACP to the origin of the posterior communicating artery (PcomA), was measured. The medial length of the C6 segment, from the most proximal visible point covered by the superior root of the ACP to the medial ICA point opposite to the origin of PComA, was measured. The length of the optic nerve from the optic chiasm (OC) to the falciform ligament was examined. The basal width of the ACP, which is a projected line that extends laterally from the lateral edge of the optic canal to the apex of the angle formed by the sphenoid ridge and the lateral aspect of the ACP, was measured intradurally. The height of the ACP, from its base to the tip of the process perpendicularly, was also recorded (Fig. 1).
Extradural anterior clinoidectomy
After a large frontotemporal craniotomy, the dura covering the anterior cranial fossa was elevated from the orbital roof and the sphenoid ridge toward the ACP, after which the sphenoid ridge was drilled with a high-speed diamond drill. The frontotemporal dural fold could be visualized and incised. After the peeling of the meningeal layer of the cavernous sinus and the dura over the ACP, the fully exposed ACP was removed using the drill via an egg-shell drilling technique16). The remnant bone particles were removed with a rongeur.
Measurement after anterior clinoidectomy
A posterior orbitectomy and unroofing of the optic canal were done. The distal dural ring was incised with care and the optic sheath was opened along the lateral margin of the optic nerve until the cranial nerve (CN) III was encountered. After an extradural anterior clinoidectomy and an orbitectomy, the distal dural ring (DDR) and the optic strut were well visualized. Next, the distances between these structures along the ICA medially and laterally were measured. The length of the lateral C6 segment of the ICA from the DDR to the origin of the PcomA was recorded (a'). Then, we measured the length of the medial C6 segment of the ICA from the DDR to the point on the medial side of the ICA corresponding to the level of the PcomA origin (b'). The length of the optic nerve from the OC to the annulus of Zinn was then measured (c'). The origin of the ophthalmic artery (OA) on the ICA and its projection were identified. The distance between the optic strut and the falciform ligament was measured (f), as was the distance between the lateral portion of the DDR and the optic strut (g). The distance between the entry of the CN III into the cavernous sinus and the point of intersection with the CN IV was measured (h). After opening the optic sheath, the OA was exposed and the distance between its origin and the optic strut was recorded (i) (Fig. 2).
RESULTS
Intradural dimension of the ACP
The ACP had an inverted triangular shape and its end was medially projected. Then intradural measurements of the basal widths ranged from 7.30 mm to 14.00 mm, with an average of 10.82 mm. The heights ranged from 5.00 mm to 11.9 mm and averaged 7.61 mm (Table 1).
Comparative measurement of optic nerve and ICA with anterior clinoidectomy
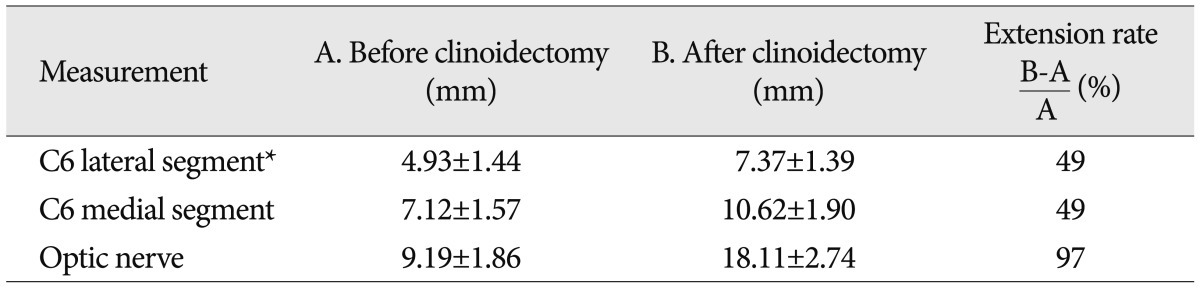
Before the anterior clinoidectomy, the mean length of the C6 lateral side (a) was 4.93 mm, and the ICA medial length (b) was 7.12 mm. The mean length of the optic nerve from the OC to the margin of the optic canal (c) was 9.19 mm. After the extradural anterior clinoidectomy, the mean length of the lateral ICA segment (a') and the medial ICA segment (b') were 7.37 mm and 10.62 mm, respectively, which showed a 49% extension of each distance. The medial length of the optic nerve from the OC to the annulus of Zinn (c') was 18.11 mm, which showed a 97% extended length (Table 2).
Relationship of paraclinoid and cavernous sinus regions
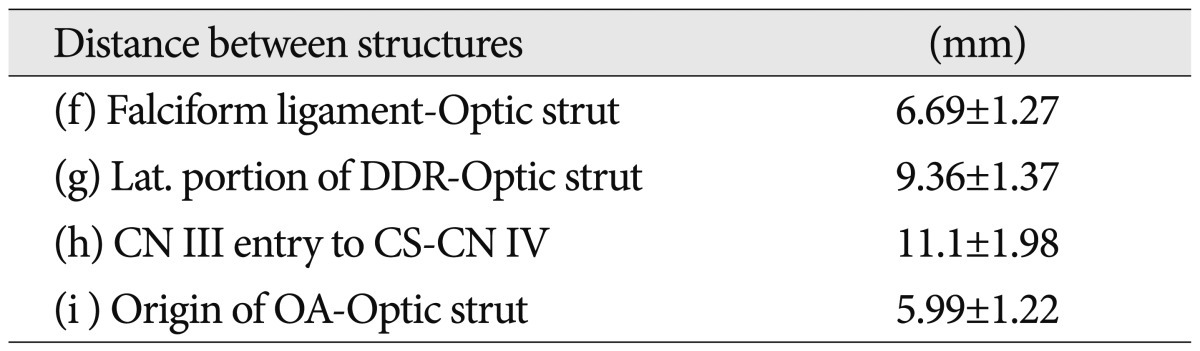
At the parasellar area, the average length from the falciform ligament to the optic strut (f) was 6.69 mm, while the average length from the lateral portion of the DDR to the optic strut (g) was 9.36 mm. The distance between the entry of the CN III into the cavernous sinus and the point of intersection with the CN IV (h) was 11.06 mm, while the distance between the origin of the OA and the optic strut (i) was 5.99 mm (Table 3).
At 15 sites, the origin of the OA was found in the intradural space, while the extradural orgin of the OA was seen at five sites. At six sites, the OA projected from the dorsal side of the ICA, whereas a dorsomedial projection was found at 14 sites. In two specimens, the origin of the OA differed on the two sides, one being intradural and the other showing an extradural origin (Table 4).
DISCUSSION
The ACP is a bony projection of the lesser sphenoid wing, and it is connected to the sphenoid body by two roots, a superior and an inferior root6). The superior root forms the roof of the optic canal, and continues as the planum sphenoidale. The inferior root forms the lateral and ventral walls of the optic canal and connects to the lesser wing. The ACP is normally composed of a thin shell of cortical bone and an inner trabecular bone. According to a study of dry skull by Lee et al.15), the means of the ACP width and height are 9.63 mm and 9.18 mm, respectively, in a Korean study. Compared with Lee's study using a dry skull, our measurement was made with fresh cadaver under surgical view intradurally. And the ACP's base was wider and the height was shorter. Compared to another study by Andaluz et al.1), the height and width were both longer in our study.
Many articles have been published about intradural and extradural anterior clinoidectomy3,5,14,16,18,19,21), and we performed an extradural anterior clinoidectomy as part of this investigation. In addition, several articles about the anatomy of the paraclinoid and cavernous sinus regions exist along with the surgical approaches through which these regions were exposed4,6,11,13). Since Dolenc7) described the extradural anterior clinoidectomy procedure, numerous modifications have been made. Anterior clinoidectomy is a technically difficult but invaluable component of surgery for a variety of anterior and middle-skull base pathologies1,6,20,21). Anterior clinoidectomy has been used widely during the clipping of paraclinoid aneurysms and removing of parasellar tumors, including meningiomas originating at the ACP, the medial sphenoid wing, or the optic canal. In the above cases, the tumor could extend to the optic canal or the optic nerve may be stretched over the tumor surface. As a result, the ACP needs to be removed to ensure an expanded space for manipulation. With the removal of the DDR of the ICA and the opening of the optic sheath, the operator gains an expanded view of the aforementioned area, after which mobilization can be gained as regards the ICA and ON for neurovascular protection7,12).
Several studies on the advantages of anterior clinoidectomy have been conducted, but studies performed in Korea are rare11,15). The purpose of our cadaveric study was to quantify the extended exposure of ICA, ON and other critical anatomical structures in the parasellar region in Korean adults. By means of anterior clinoidectomy, we found mean increases of 49% on the C6 segment of the ICA, both medially and laterally. Mean exposure of the ON increased by 97%. These increases in surgical exposure can offer numerous advantages, such as less traction of normal structures and sufficient exposure of pathogenic lesions. A study by Hwang et al.10) showed almost a 150% increased extension of ICA, a two-fold increase of ON and an opticocarotid triangle (OCT) exceeding 300% by means of an extradural anterior clinoidectomy. As traction of the ICA could be influenced by subjective factors, we did not check the OCT, but we measured medial and lateral sides of ICA, respectively. Other results were similar to our data. In a study of Andaluz et al.1), the exposure of the ICA increased by 60% and 112% in terms of the lateral and medial lengths, respectively. The exposure of the optic nerve was increased by nearly 150% in terms of the length. These results were different from ours, and different anatomical features according to race may have been a factor in these differences.
After an extradural anterior clinoidectomy and orbitectomy, the falciform ligament and the DDR were removed with the opening of the optic sheath. We also measured the distance around the paraclinoid and cavernous sinus regions. Compared with the studies by Collignan and Link4), the distance from the optic strut to the origin of the OA and to the lateral portion of the DDR was longer in our study. Moreover, the distance between the entry of the CN III into the cavernous sinus and point of the intersection with the CN IV was longer, as was the distance from the optic strut to the falciform ligament. We also assumed that racial differences in the skull anatomy may have contributed to those results.
After finishing the aforementioned procedures, we identified the origin of the OA related to the dura and the ICA. The OA usually originates from the intradural portion of the ICA at a reported rate of 79.9-98% in some studies5,8,13). In fewer cases, the OA originates from the extradural or interdural portion. In our study, an intradurally originating OA was found at 15 sites (75%) and an extradurally originating OA was noted at 5 sites (25%). In two cadavers, the origin of the OA was not equal on two sides. The OA may originate from the dorsomedial wall of the ICA or from the lateral and dorsal wall of the ICA5,8,13). According to another study, the origin of the OA in the dorsomedial aspect of the ICA occurred in 71% of the cases, while the rate for the dorsal aspect was 29%7). However, we found OAs originating from the dorsal wall of the ICA at 6 sites (30%) and from the dorsomedial side of the ICA at 14 sites (70%). These results were fairly similar to those of other studies.
The goal of our study was to quantify the acquired space for manipulation by extradural anterior clinoidectomy, orbitectomy, the release of the DDR and the opening of the optic sheath. Many studies have been conducted regarding this subject in other countries, but few have been done in Korea. Consequently, we tried to design a Korean study. There were some limitations in this research, mainly the small number of cadavers.
CONCLUSION
Anterior clinoidectomy is a difficult procedure with limited indications. This study was focused on the morphometrical benefit obtained by extradural anterior clinoidectomy in Korean adults. With the removal of the ACP, the length of the C6 segments of the ICA can be increased by approximately 49% and the ON length ca be nearly doubled. Although neurointervention techniques and radiosurgery have improved and are now used as a treatment for skull base pathologies, we suggest that this technique becomes a part of a neurosurgeon's essential skill set for treating pathologic lesions around the parasellar area.



 XML Download
XML Download