

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The most common treatment for hydrocephalus is insertion of a ventriculoperitoneal (VP) shunt. A VP shunt is associated with several well-recognized complications, including infection, hemorrhage, neural trauma, shunt malfunction, and blockage. One of the complications that causes a shunt system malfunction is migration of the distal catheter. Migration of the distal end of the catheter to different regions such as the thoracic cavity, pulmonary artery, bladder, scrotum, heart, and stomach had been reported4,5,9,10,12,15). However, proximal migration of the distal end of a catheter to the subgaleal space has been rarely reported3,6,8,11). We present an unusual case of a preterm baby with a VP shunt and scalp swelling 21 days after the shunt operation. The distal catheter had migrated completely into the subgaleal space and was coiled inside the space.
CASE REPORT
An 8-month-old boy was admitted to our clinic with scalp swelling that developed 21 days after a VP shunt operation. He had no other neurological symptoms except scalp swelling. He was a preterm baby born at 24 weeks of gestational age and was only 520 g at birth. The patient had developed a massive intraventricular hemorrhage associated with hydrocephalus on brain ultrasonography. Furthermore, the QUAD test for preterm screening was positive for Down's syndrome. He had many severe preterm complications, including hematological problems such as anemia and thrombocytopenia that required transfusion; pulmonary problems such as respiratory distress syndrome treated with surfactant and a chest tube was inserted to manage pneumothorax. He also had retinopathy and many cardiac problems such as patent ductusarteriosus (PDA), ventricular septal defect, right ventricular hypertrophy, and a patent foramen ovale. We intended to wait for natural closure for most problems but PDA required ligation surgery. Endocrinological problems such as hyperglycemia, hypothyroidism, and osteopenia were managed with hormones and mineral replacement. Urological complications such as a dilated bladder and ureter and hydronephrosis developed but were mild; thus, we decided to follow-up closely without surgical intervention. He also had a small bowel perforation and bilateral inguinal hernia, which had gone through repair surgery.
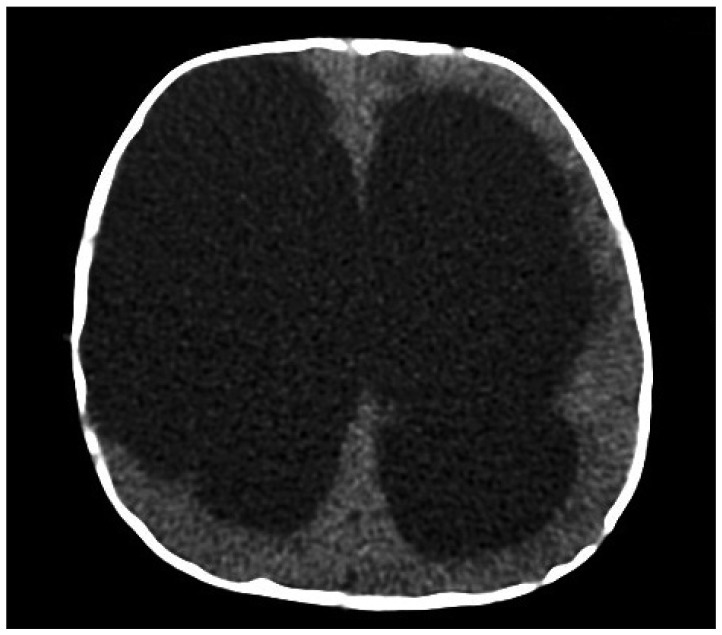
For only 25 weeks after birth, he had 3 surgeries, brain ultrasonography was conducted and progression of the hydrocephalus and encephalomalacic changes in the right frontal lobe was found (Fig. 1). Spinal tapping for intracranial pressure control was held every day until shunt surgery was capable. At 30 weeks of his gestational age (14 weeks of corrected age) his body weight was 4500 g (<10 percentile) a VP shunt has been inserted using an ultra small, low pressure valve system (Strata®; PS Medical, Gola, CA, USA) and a distal catheter of about 30 cm in length was placed in the peritoneal cavity. No complications occurred except mild redness of the left clavicle area where the catheter passed. The patient was discharged without any complications 12 days after surgery.
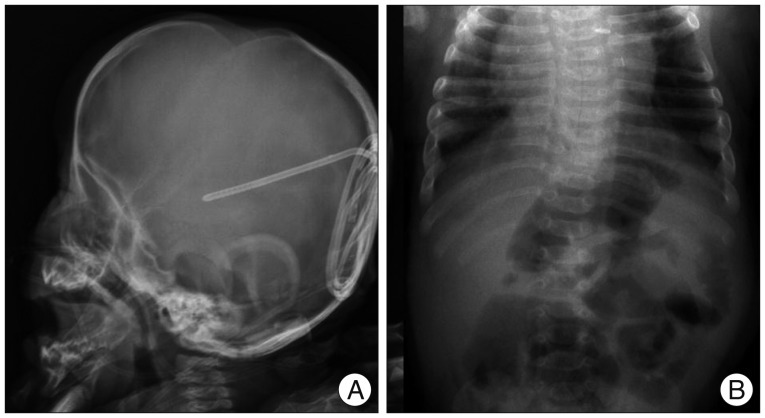
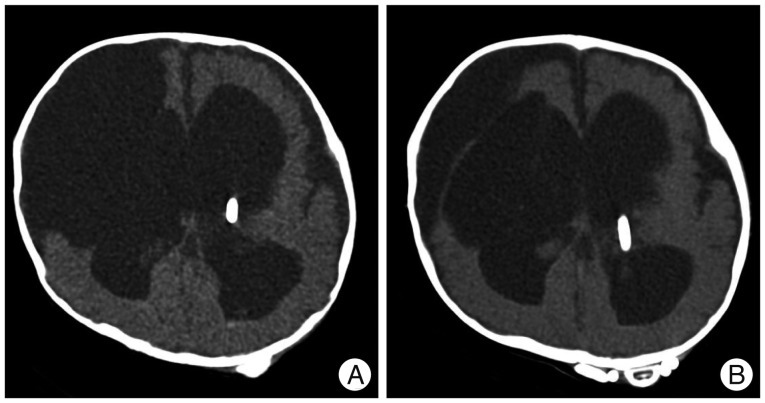
He visited our outpatient office with prominent swelling of the surgical site 21 days after surgery, and a round coil like mass was palpable under the scalp, but no neurological changes were noticed. Simple chest, abdomen, and skull X-ray images were taken, and no shunt catheter on the trunk was found, but the distal catheter had migrated upward into the subgaleal space (Fig. 2). Brain computed tomography scans indicated decreased ventricle size compared to those taken before surgery (Fig. 3). Shunted cerebrospinal fluid (CSF) was thought to be absorbed in the subgaleal space and shunt function seemed to be maintained.
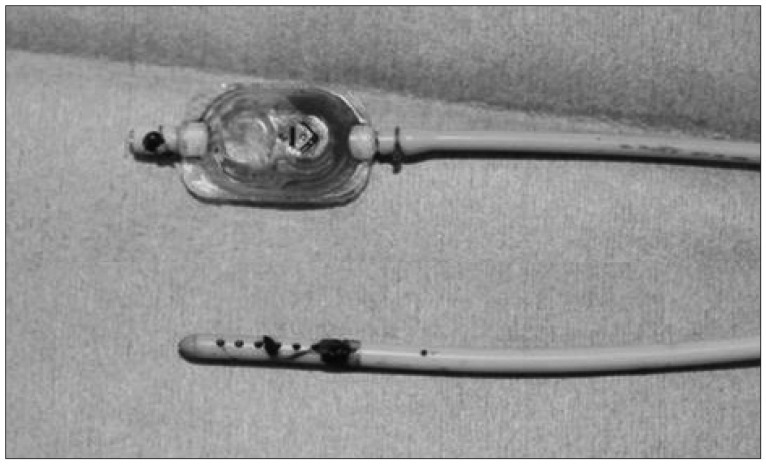
The distal catheter inserted previously for the VP shunt was found coiled freely in the subgaleal space under the primary incision during revision surgery. The shunt was otherwise functioning, but the reservoir was filled with an old hematoma, and the CSF was bloody and turbid (Fig. 4). We placed an extraventricular drainage (EVD) tube rather than a shunt system to wait for the CSF to clear out to prevent shunt system blockage. The VP shunt was reinserted 1 week after the EVD, and the patient was discharged. No further problems were noted during regular follow-ups at the outpatient office.
DISCUSSION
Various complications can occur during a shunt operation, but they can be summarized into infection, mechanical failure, and functional failure3). Although shunt complications are often multifactorial, a non-infectious cause for a shunt complication generally requires shunt revision3). Mechanical failure of a shunt system includes disconnected parts and obstruction and migration of the shunt system.
Among them, catheter migration is a less common event. Sayers reported migration of a distal catheter resulting in malfunction in only three of 1390 shunt procedures16). A review of the literature revealed numerous sites for distal catheter migration, including the liver, heart, umbilicus, colon, bladder, small intestine, stomach, scrotum, anus, and chest. These migrations usually involve perforation of the hollow viscus or penetration of involved organs. However, migration of a shunt system upward through its previous pathway has been rarely reported. We found 12 cases that migrated upward; seven to the subgaleal space3,6,8,11) and five to the ventricle2,7,13).
Numerous hypotheses for upward migration of shunt distal tubing have been reported. Pang and Wilberger14) considered that reabsorption of subgaleal fluid may generate negative pressure, dragging the distal tubing proximally. Scott et al.17) postulated a "windlass effect", with some granulation tissue or valve placed below the scalp, which acts as an anchoring point and the patient's repeated head motion allows the distal tubing to be pulled in a proximal direction. Abou el Nasr1) considered that increased abdominal pressure during crying may act as pushing force for distal tubing to migrate upward. The memory of devices placed in packaging allows the tubing to recoil as explained by Dominguez et al.6) as a "memory phenomenon". A shunt placed in the occipital area rather than the frontal area has a relatively short distance between the ventricular and peritoneal ends, allowing for a straight and unobstructed upward migration pathway7). Unishunt catheters with a spring coil mechanism and no interposed valves or flushing devices are more frequently involved in migration3). Acharya et al.2) reported that shunt migration depends on various factors such as the type of catheter and reservoir used. In our review of 12 other reported cases, every case used a different shunt device with or without a valve system and we could not find any association between the type of device and its tendency to migrate upward. The average age at first VP shunt surgery in the 12 cases, except a woman aged 32, was 333 days, and the average number of days to revision was 48. In our case, initial shunt surgery was conducted at 100 days after birth and the revision was 21 days after the initial surgery. Shunt migration in children is more frequent. None of the migration hypotheses are clearly defined but many similar cases include the "windlass effect". Shunt migration in children seems to be more frequent, because the shorter length of a distal catheter than that of adults makes it easier for the shunt to migrate, and children cannot control their head motion, which leads to the windlass effect. In our case, repeated head motion was denied by the patient's parents, and the shunt catheter used was not packaged in a coiled fashion. Thus, the windlass effect and memory phenomenon did not explain our case. No massive dissection of the subgaleal space was found during the first surgery, and no subgaleal fluid collected after surgery. As catheter migration cannot be clearly prevented, it is important to secure a shunt device during surgery and follow a child's symptoms and wound postoperatively.
CONCLUSION
Proximal migration of VP shunt distal tubing is a rare complication. Reabsorption of subgaleal fluid and repeated head motion of the child were considered to pull the catheter proximally in a windlass motion. Proper fixation of the components by suturing the shunt chamber and catheters as well as minimal dissection under the scalp is important to prevent migration of a shunt device. But, no clear issues such as the child's head motion were observed in the present case. We present an unusual case of complete migration of a distal catheter of a shunt system under the scalp. Similar cases indicated that repeated flexion-extension movements of a patient's head may play a major role in migration of a distal catheter to a more proximal location.
 XML Download
XML Download