

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The goal of treatment of cerebral aneurysm is completely obliteration of their lumen, excluding the entire aneurysm from the arterial circulation. Usually microsurgical clipping attains this goal, but aneurysm remnants can occur in 5.2% of patients who undergo postoperative angiography16). These remnants are associated with potential for subarachnoid hemorrhage from rupture and regrowth over time6, 7). In second operation, surgeons often experience technical difficulty because of scars or dense adhesions surrounding the aneurysm, and configuration and location of aneurysm5).
There have been technical improvements in endovascular coiling, and technology has allowed some of these remnants to be treated safely1,15). However, endovascular coil embolization also has limitations in the treatment of wide-neck aneurysm due to possible coil migration into the parent artery and long-term recurrence4,18). Technical advances make it possible to treat wide-neck aneurysm using variety of endovascular strategies such as double catheter technique10), balloon-assisted coiling13), and stent assisted coiling2,14). Recently, the stent-jack3) and semi-jailing9,19) techniques have been introduced for patients with broad-necked aneurysm. We report a case of remnant wide-neck aneurysm with small caliber parent artery (about 1 mm) following clipping, treated by a temporary semi-jailing technique12) using the Enterprise stent system (Cordis Neurovascular, Miami, FL, USA).
CASE REPORT
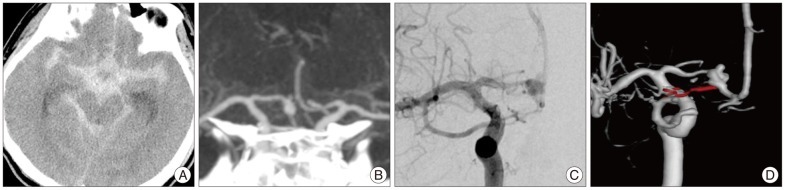
A 41 years old man with seizure like movement was admitted to our hospital. He had a history of hypertension treatment for 3 years. On neurologic examination, the patient was drowsy (Glasgow Coma Score : E3, V4, M6). He showed 2/5 and 3/5 strength in the right and left lower extremity and 5/5 strength in both upper extremities. Hunt-Hess classification was 3, and Fisher grade was 4. Initial computed tomography (CT) revealed the presence of a subarachnoid hemorrhage and aneurysm in the A1 segment of the anterior cerebral artery (ACA) with inferior and superior projection. The patient was treated with surgical clipping and upper extremity weakness was fully recovered. But superior and posterior portion of the aneurysm remained on follow-up transfemoral cerebral angiography (Fig. 1). We decided to treat the remnant aneurysm using an endovascular modality.
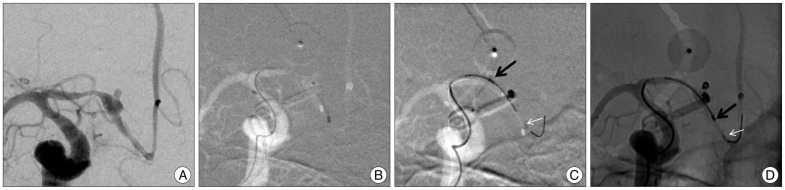
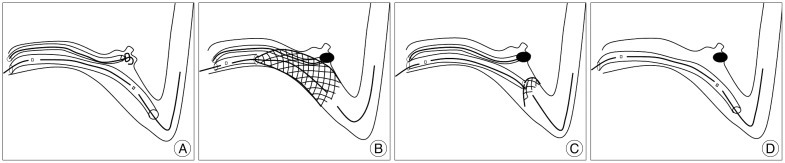
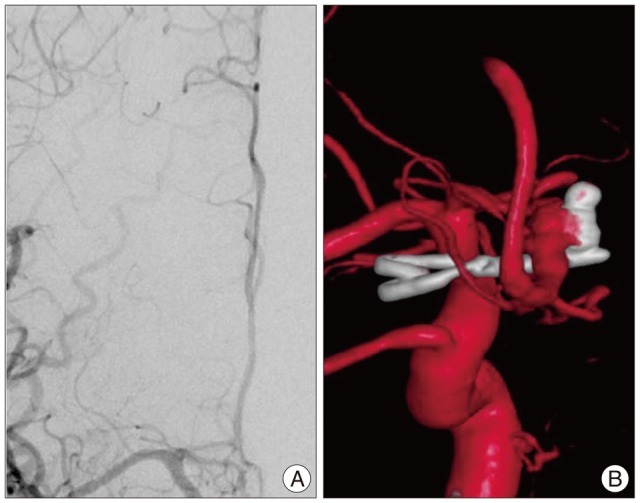
The patient was placed on 300 mg of clopidogrel, 100 mg of aspirin one day before embolization and 75 mg of clopidogrel, 100 mg of aspirin on the day of operation. Treatment was performed under general anesthesia and via the transfemoral approach. Under full heparinization, a 6-French guide catheter was placed in the right internal carotid artery. A Prowler Select Plus microcatheter (Cordis neurovascular, Miami, FL, USA) was navigated across the aneurysm neck over a 0.014'' microguidewire. An Excelsior SL-10 microcatheter (Striker, Fremont, CA, USA), for coil delivery were carefully navigated to the aneurysm. Through Prowler Select Plus microcatheter, a 4.5×22 mm Enterprise stent advanced and readied for deployment. The stent was partially deployed (up to 30-60% of its length) bridging the aneurysm's wide neck. Subsequent coil packing (4 coils, sizes ranging from 2×30 mm to 1.5×10 mm, Micrus Endovascular) resulted in subtotal occlusion of the aneurysm without coil herniation through the stent struts into the parent lumen (Fig. 2). Whenever each coil was inserted, the stent was partially recaptured into the Prowler Select Plus microcatheter then the SL-10 microcatheter was removed for angiography to ensure safety of the small caliber parent artery (Fig. 3). A final control angiogram confirmed aneurysm occlusion, and preservation of the blood flow within the territory including A1 segment (Fig. 4). The patient awoke without neurological deficit. One day follow-up CT showed no abnormal low density in ACA territory. Follow-up transcranial doppler ultrasonogram showed patent blood flows of bilateral ACAs (right : left, mean=78 : 74, systolic 118 : 104, diastolic=54 : 55). Further clinical and neurological follow-up examinations are planned after 1 and 3 months, and digital subtraction angiogram (DSA) follow-up are planned after 6 months.
DISCUSSION
The aneurysm remnants after surgical clipping may be caused by anatomic complexities, technical difficulties at the time of surgery and regrowth after surgery5,8,11). In this case, the superior and posterior compartment of aneurismal sac cannot be clipped because of limitation imposed by the configuration and location of the aneurysm.
Second surgeries usually face scars or dense adhesions surrounding the aneurysm in proportion to the interval between surgeries5). With evolution of devices and techniques of endovascular treatment, an alternative to surgical clipping in the management of cerebral aneurysm is now offered. In addition, endovascular and surgical modalities can be successfully incorporated into a single therapeutic plan and can result in good outcome7,17).
From a technical point of view, remnant coiling is usually possible if the remnant is at least as deep as it is wide and if it is at least 2 mm in diameter1). However, there are several challenging factors in the endovascular treatments of wide-neck aneurysm with small caliber parent artery. First, it is highly possible that protruded coil induce parent artery occlusion. Second, supporting devices such as balloon and stent have several limitations. Using the balloon remodeling technique in small caliber parent artery can cause periodic flow arrest to the parent vessel, which may result in thromboembolic or rupture complications. Permanent stent deployment in small caliber parent artery also has a risk of in-stent stenosis or occlusion as the long-term outcome. The recommended parent vessel diameter for permanent deployment of Enterprise stent is 2.5-4 mm. Another limitation of stent, not associated with this case, is antiplatelet medication. Stent-assisted coiling of wide-neck aneurysms is not recommended in patients with gastrointestinal bleeding, complex medical problems, or those scheduled for subsequent surgery, and in patients with acute subarachnoid hemorrhage because antiplatelet medication is required. The technique depicted in this case report was very helpful in successfully coiling a wide-neck aneurysm with small caliber parent artery.
There are some important things to do in this procedure that should be discussed. It was very critical to lock the stent delivery wire with a hemostatic valve once the stent was partially deployed, to prevent further deployment of the stent12). Repeated recapture and coil microcatheter removal are necessary to ensure the patency of a small caliber parent artery on DSA. Before recapture of the stent, it is important to wait for several minutes to make sure of coil mass stability, and ascertain coil mass stability under digital subtraction background during retrieval. If coil movement is detected during stent retrieval, redeployment of the stent would be the rescue maneuver.
 XML Download
XML Download