

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Incidental dural tear is a well-known complication of spinal surgery3,11). Large migrated lumbar disc herniations predispose patients to dural tear, and unrecognized dural tears have been known to occur during discectomy for this condition2,8). Here, we report 2 cases of nerve root herniation into the intervertebral disc space through an unrecognized ventral dural tear. Despite a relapse of severe sciatic pain after surgery, the diagnosis was delayed because of the existence of multilevel lumbar stenosis.
CASE REPORT
Case 1
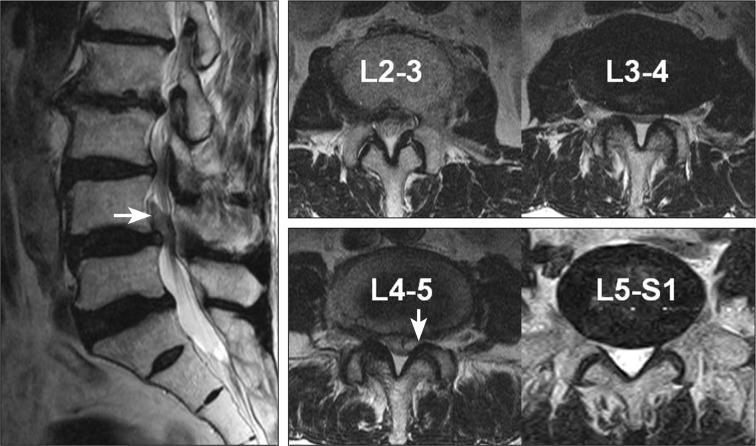
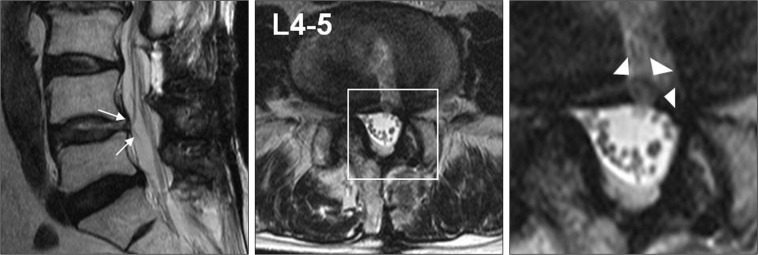
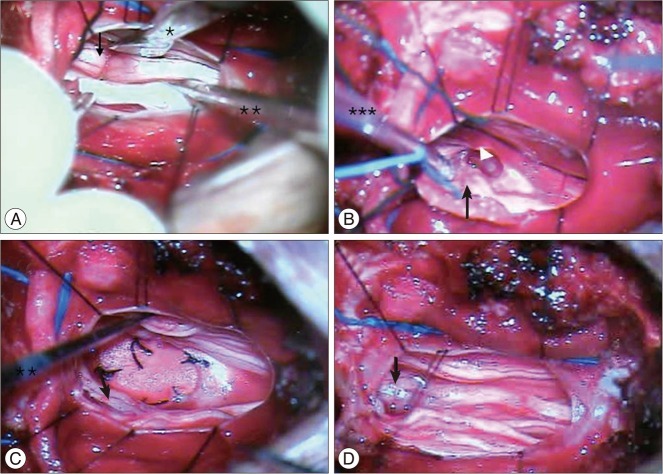
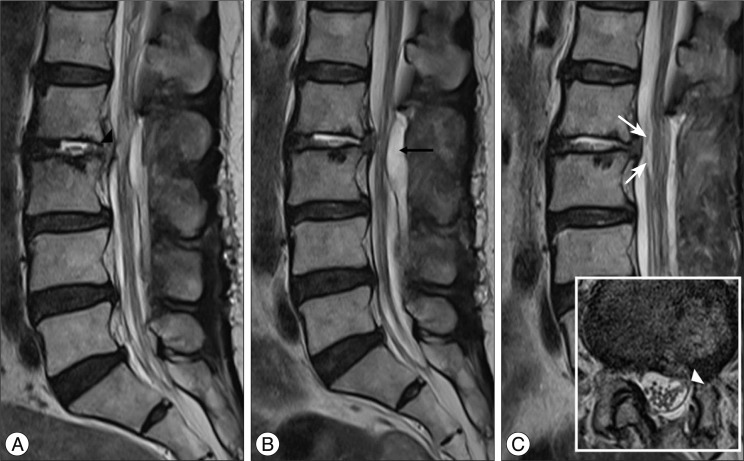
A 56-year-old man presented with pain in the lower back, radiating from the left buttock to the anterior leg. The onset of symptoms occurred 4 weeks before presentation. Physical examination revealed numbness in the left big toe with intact motor function. The deep tendon reflexes were decreased on both lower extremities. Plain radiography of the spine showed no definite instability. Magnetic resonance imaging (MRI) (Fig. 1) demonstrated a very large disc herniation at the left L4-5 level (with upward migration evident on sagittal scans), spinal stenosis at the L2-3, L3-4, and L4-5 levels, and mild lateral recess stenosis at the left L5-S1 level. Microscopic discectomy was performed at the left L4-5 level. The preoperative radiating pain from the left buttock to the anterior leg was greatly improved after the initial operation (Fig. 2A), and the patient was discharged on the sixth day after surgery. Ten days later, he visited the outpatient clinic with severe pain radiating from the left buttock to the posterior thigh. He was unable to maintain a supine position because of the pain, which was most severe during position changes. The symptoms had started 1 week before presentation at the outpatient clinic and had worsened over time. MRI showed no apparently significant interval change from the immediate postoperative MRI (Fig. 2B). Because the patient continued to complain of left buttock pain, additional decompression for the left L3-4 and L5-S1 levels was performed (Fig. 2C). However, his buttock pain did not improve and continued to be most severe in the morning and during position changes. The symptoms worsened in spite of conservative treatments including oral analgesics, physiotherapy, and root block. Eventually, the patient could not sit down or walk even 100 m because of severe pain radiating from the left buttock to the posterior thigh. The pain was especially aggravated when the patient was in a flexion position. Finally, we found ventral herniation and entrapment of a nerve root at the L4-5 level on an MRI rescan (Fig. 3), a diagnosis that had been missed since his first visit to the outpatient clinic, with newly developed buttock and posterior leg pain following the first operation. The patient underwent open surgery under a microscope. After total laminectomy of L4, a linear dural incision was made at the level of the L4-5 disc space. Rootlet herniation through the ventral dural defect with severe adhesion between the rootlet, dura, and disc was observed (Fig. 4). We repositioned the herniated rootlet and repaired the dural defect by using artificial dura. After meticulous hemostasis, the dorsal dura was closed in a watertight fashion. Postoperative MRI revealed complete release of the rootlet, and the patient's symptoms markedly improved. He was discharged on the 12th day after surgery without any further complications. The patient showed mild paresthesia of the left foot without any pain at the 6-month follow-up.
Case 2
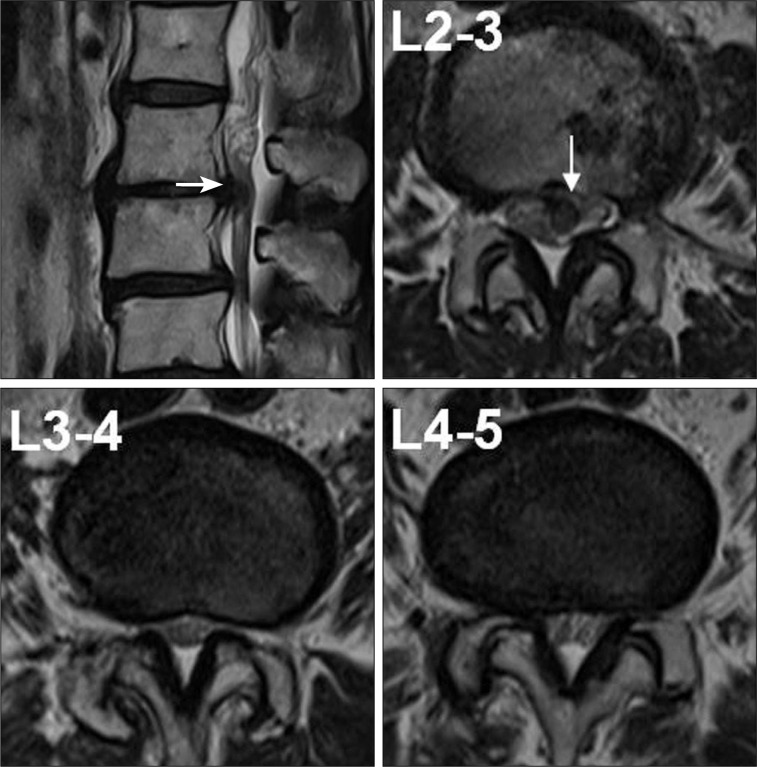
A 64-year-old woman presented with pain in the lower back, radiating from the left buttock to the lateral leg. This symptom had surfaced 3 months before the presentation. Physical examination revealed left knee flexion weakness (Gr. 4) and numbness in the left lateral leg. The deep tendon reflexes were normal for both lower extremities. Plain radiography of the spine showed no definite instability, but MRI (Fig. 5) showed paramedian extruded disc herniation at the left L2-3 level and spinal stenosis at the L3-4 and L4-5 levels. Microscopic discectomy was performed at the left L2-3 level without any complications. Although the radiating pain greatly alleviated immediately after the surgery, it relapsed the next day. The pain was too severe for the patient to stand or even change her position while in the supine position, and the pain did not subside even after an opiate injection. MRI showed no significant postoperative findings such as recurrent disc herniation or hematoma. The patient underwent additional decompression for the left L3-4 and L4-5 levels (Fig. 6A). MRI performed 1 week after the surgery showed an epidural hematoma at the L2-3 level. We performed computed tomography (CT)-guided needle aspiration to decompress the thecal sac (Fig. 6B, C), but this did not alleviate her pain, which had continued to worsen over time. Eventually, she developed lower extremity motor weakness and muscle atrophy (knee flexion, Gr. 1; ankle dorsiflexion, Gr. 4; and big toe dorsiflexion, Gr. 3). Finally, we performed microscopic exploration at the L2-3 level and found that approximately 4 rootlets had herniated into the L2-3 disc space. We released the entrapped rootlets and repositioned them via the transdural approach, and the ventral dural defect was then closed with artificial dura. Postoperative MRI showed complete release of the rootlets. Although the patient's pain markedly alleviated after this surgery, she continued to experience knee flexion weakness, which has been ameliorating with rehabilitation. The patient showed improvement of the knee flexors with mild paresthesia of the lower extremities at the 6-month follow-up.
DISCUSSION
Incidental dural tear is a common complication of spinal surgery, and the reported incidence rates range from 3.1% to 14%3,11). The risk of dural tears is increased by conditions such as fibrotic adhesion, scar tissue from prior surgery, eroded dura, or redundant dura in patients with large disc herniations2,8). Advanced patient age and the surgeon's training level are other factors affecting the incidence9). Good long-term outcomes have been reported when incidental dural tears were recognized intraoperatively and repaired primarily3,5). Common sequelae associated with dural tear are headaches and wound infection in the short term and persistent cerebrospinal fluid (CSF) leak, pseudomeningocele, neurologic deficits, and arachnoiditis in the long term3). Nerve root herniation is an infrequent complication of incidental dural tear. Nishi et al.6) reported the occurrence of nerve root herniation into the facet joint through the arachnoid space after multiple laminectomies and discectomies. Töppich et al.10) reported 2 cases of nerve root entrapment in the intervertebral space after lumbar discectomy. One of these cases was due to an unrecognized dural tear and the other from an incidental dural tear that was recognized and repaired using Gelfoam and fibrin glue. Both cases followed clinical courses similar to the present cases. The patients experienced temporary improvements immediately after surgery and then had sudden relapses of sciatic pain. The symptoms were aggravated by movement. Ahn et al.1) summarized the typical symptoms of nerve root entrapment syndrome as follows : relapse of intractable radicular pain that may be either dermatomal or nondermatomal, resembles electric shock in nature, and depending on the location of the dural tear, is aggravated by walking or position change and is accompanied by various neurologic deficits. It is very important that the possibility of nerve root herniation be considered when a patient presents with these clinical features. When the dural tear is unrecognized, nerve root herniation is less likely to be diagnosed and treated with revision surgery if its presence is not strongly suspected. In the present cases, when postoperative MRI confirmed the absence of hematoma, recurrent disc herniation, or infection, we misdiagnosed the patient's relapse of sciatic pain after surgery as nerve root compression from remaining multiple lumbar stenoses. Therefore, this report shows that nerve root herniation should be included as a differential diagnosis for new or recurrent sciatic pain after spinal surgery when there is no evidence of recurrence or infection on imaging studies1).
Several radiographic findings are especially suggestive of nerve root herniation. CSF signal in the disc space on MRI implies the presence of a dural tear. CSF had collected in the disc space in the present cases, which we failed to recognize, but it had already been present immediately after surgery. Since the CSF collection was localized to the disc space, neither CSF drainage through the wound drain nor CSF collection in the posterior epidural space occurred. Another important finding that can be observed on sagittal MRI is nerve root displacement, which takes the shape of a gull's wing. On retrospective review of the present cases, we could visualize this nerve root displacement through the ventral dural tear into the disc space. Although a single rootlet is easy to overlook, a strong impression of its presence can be formed. It is our opinion that these 2 radiological findings are very useful for diagnosing nerve root herniation.
In the present cases, we found a direct entrapment of the rootlet within the annulus of the intervertebral disc. Several authors have reported dural tears in which the rootlet was irritated without direct entrapment1,10), which induces pain only during movement. This can be diagnosed only by clinical manifestations and operative findings and not by imaging findings. Patients who are at an increased risk for dural tears should be carefully examined when they complain of new or recurrent sciatic pain. The multilevel lumbar spinal stenosis in the present cases confounded early and correct diagnosis. Although the imaging findings were highly suggestive of nerve root herniation, we focused on finding compressive lesions. This excessively narrow focus delayed diagnosis and treatment of these patients.
Re-exploration with repositioning of the herniated nerve root and repair of the dura with or without artificial dura must be performed as soon as possible. Incidental dural tears do not adversely influence the long-term prognosis if they are properly repaired3-5). In addition to nerve root herniation, unrepaired dural tears can lead to pseudomeningocele formation, persistent CSF leakage, meningitis, or arachnoiditis7,11). Ahn et al.1) pointed out that unrecognized dural tears follow complex clinical courses because delayed widening of the dural opening by CSF pressure can cause significant neural entrapment, which cannot easily be detected. In the present cases, we found severe adhesion between the nerve root, the surrounding dura, and the intervertebral disc. Since the diagnosis was delayed, the nerve root herniated through the ventral dura and closed the hole. While this stopped the CSF leakage, inflammatory changes fixed the nerve root between the ventral dura and intervertebral disc. This made it difficult to release the nerve root without further injury. The most important aspects in the management of nerve root herniation are early recognition and prompt repair.
CONCLUSION
Nerve root herniation is a rare complication after discectomy for lumbar disc herniation. Clinical manifestations and suggestive radiological findings have important diagnostic value. Clinicians must consider the possibility of nerve root herniation, especially in patients who are at risk for dural tears. Early diagnosis and primary repair with reposition of nerve root are sufficient for treatment.

 XML Download
XML Download