

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Recently, anterior interbody fusion (ALIF) has been performed in various spinal disorders and has become a more common and popular procedure. A wide range of diseases entity has been treated by ALIF, including degenerative spondylosis, spinal trauma, tumors, infections and deformities. In particular, foraminal height narrowing is one of the appropriate indication for ALIF. Moreover, ALIF has allowed the spine surgeon to achieve better outcomes for multilevel interbody fusion and to achieve optimal lumbar lordosis2,15).
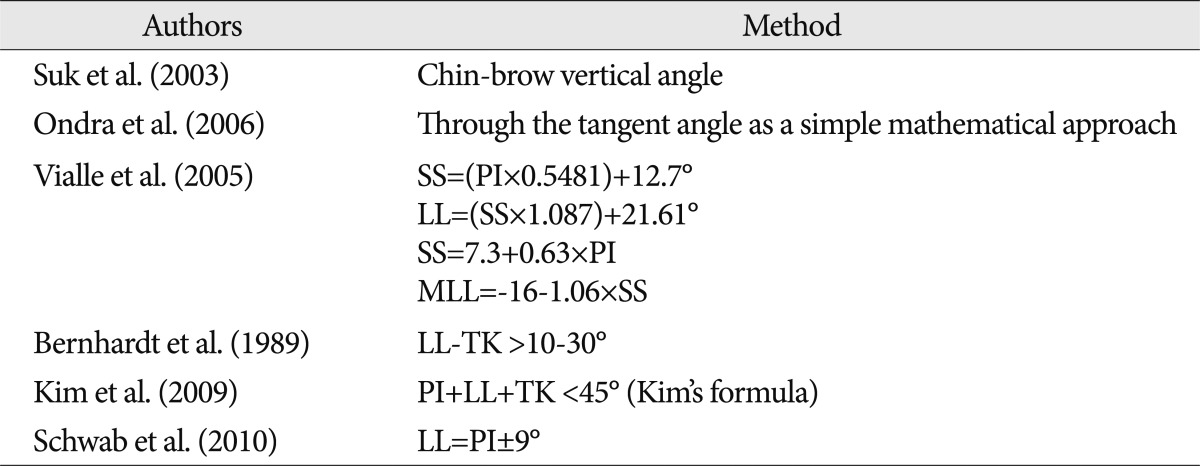
The ideal spinal alignment and the degree to which lumbar lordosis should be corrected during the spine deformity surgery has been discussed in numerous reports. Suk et al.22) have recommended a chin-brow vertical angle kyphosis correction plan and a method to determine prognosis after the surgery. Ondra et al.14) have suggested that tangent angle can be used for a simple mathematical approach to the vertebral pedicle subtraction osteotomy for a correction of lumbar lordosis (LL). However, the above studies offered parameters only for the correction of fixed-type kyphosis. For a flexible-type kyphosis, Vialle et al.25) have studied the importance of sagittal imbalance of the spine for the treatment of patients with various spine angles. Pelvic incidence (PI), maximum lumbar lordosis, and sacral slope are the parameters which should be included in lumbar lordosis correction calculations, and the relationships between these values are shown in Table 1.
However, the previous reported methods are very complex and they have become difficult to apply and calculate on operation. These methods also require special materials, such as a clinical photo. In the past, uncomplicated methods to achieve an optimal sagittal balance were often sought and studied. In a study by Bernhardt et al.1) 1989, a well-balanced spine was found to have between 10 and 30 degrees more lumbar lordosis than thoracic kyphosis. Kim et al.17) introduced various factors which predicted the achievement of optimal sagittal balance, PI+LL+TK <45°, that showed sensitivity for predicting ideal sagittal balance (Kim's formula). In recent years it has been suggested that LL values should be corrected at least to the value of PI, PI+ or -9 degrees20).
For the correction of LL and spinal sagittal balance, a spine surgeon must perform many types of osteotomies which are not insignificant operations; these operations carry various perioperative risks and are procedures associated with high morbidity13). Due to the high risks associated with various osteotomy operations, we have concluded that the aggressive osteotomy techniques should be replaced with more benign operations to achieve optimal postoperative lumbar lordosis. Anterior interbody lumbar fusion is another surgical procedure used to achieve adequate sagittal balance which is performed using a fixed set angled cage. We have studied the angle of these fixed settings with the goal of determining the possibility of achieving optimal sagittal balance.
MATERIALS AND METHODS
Patient population
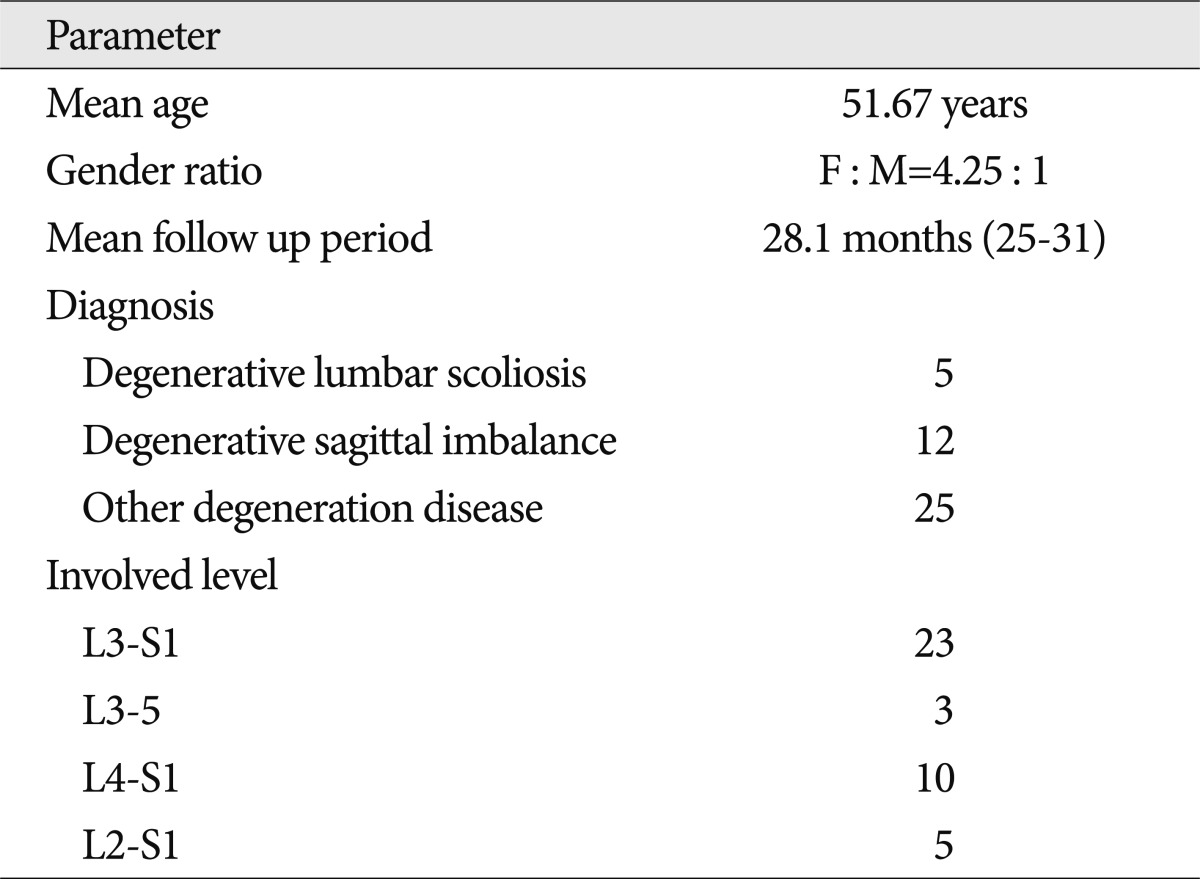
We retrospectively reviewed the radiograph results of 42 patients with lumbar degenerative disease. Three parameters were evaluated on lateral whole spine radiographs of 42 patients in the multilevel ALIF group : LL, PI and sagittal vertical axis (SVA). Patients underwent more than two level anterior lumbar interbody fusions combined with posterior screw fixation at our hospital between 2008 and 2009. All of the patients were followed for a minimum of 2 years after the surgery. The numbers of patients undergoing surgery were : L3-S1 (3 levels); 23 cases, L3-5 (2 levels); 3 cases, L4-5-S1 (2 levels); 10 cases, L2-S1 (4 levels); 5 cases. Diseases entities included degenerative lumbar scoliosis, degenerative sagittal imbalance, and other degenerative diseases. The ratio of males and females was 1 : 4.25. The mean follow-up period and the mean age were 28.1 months and 51.76 years, respectively (Table 2).
Surgical procedures
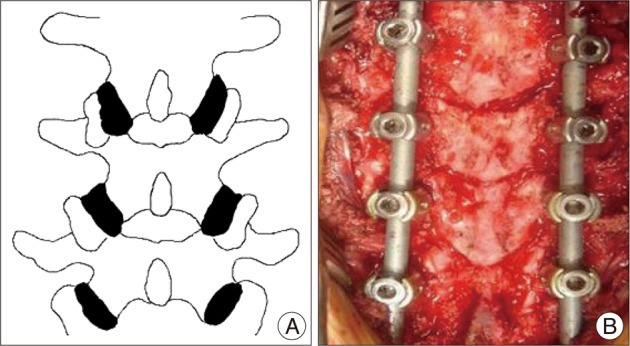
All of the ALIF procedures were performed by a spine surgeon applying a two-stage operation technique with an interval between each stage of one week. The first phase was a posterior approach for spinal decompression and facet release using a V-osteotomy (Fig. 1). The second phase was an anterior approach for interbody fusion with prone positioning to support the posterior instruments. For ALIF, the spinal column was approached through a paramedian incision followed by retroperitoneal dissection. After dissection, the disc spaces were confirmed with radiographs, excision of the anterior longitudinal ligament and the intervertebral discs was performed using standard techniques. The end plate preparation was achieved completely and carefully without causing a damage8,12). After removing disc material, spinal decompression was confirmed. Interbody devices used for wedge shaped cage angle setting had an angle distribution of 14, 16, 18 degrees (Medtronics™). All of the patients underwent the pedicle screw insertion by a standard midline approach following their ALIF procedure. Facet release osteotomy was the same as V-osteotomy and was performed in all patients.
Post-operatively, all patients ambulated as early as possible and wore a thoraco-lumbo-sacral orthosis for a period of 12 weeks. We obtained standing whole spine radiographs prior to discharge and thereafter at 1, 3, 6, and 12 months, and then annually.
Clinical outcome
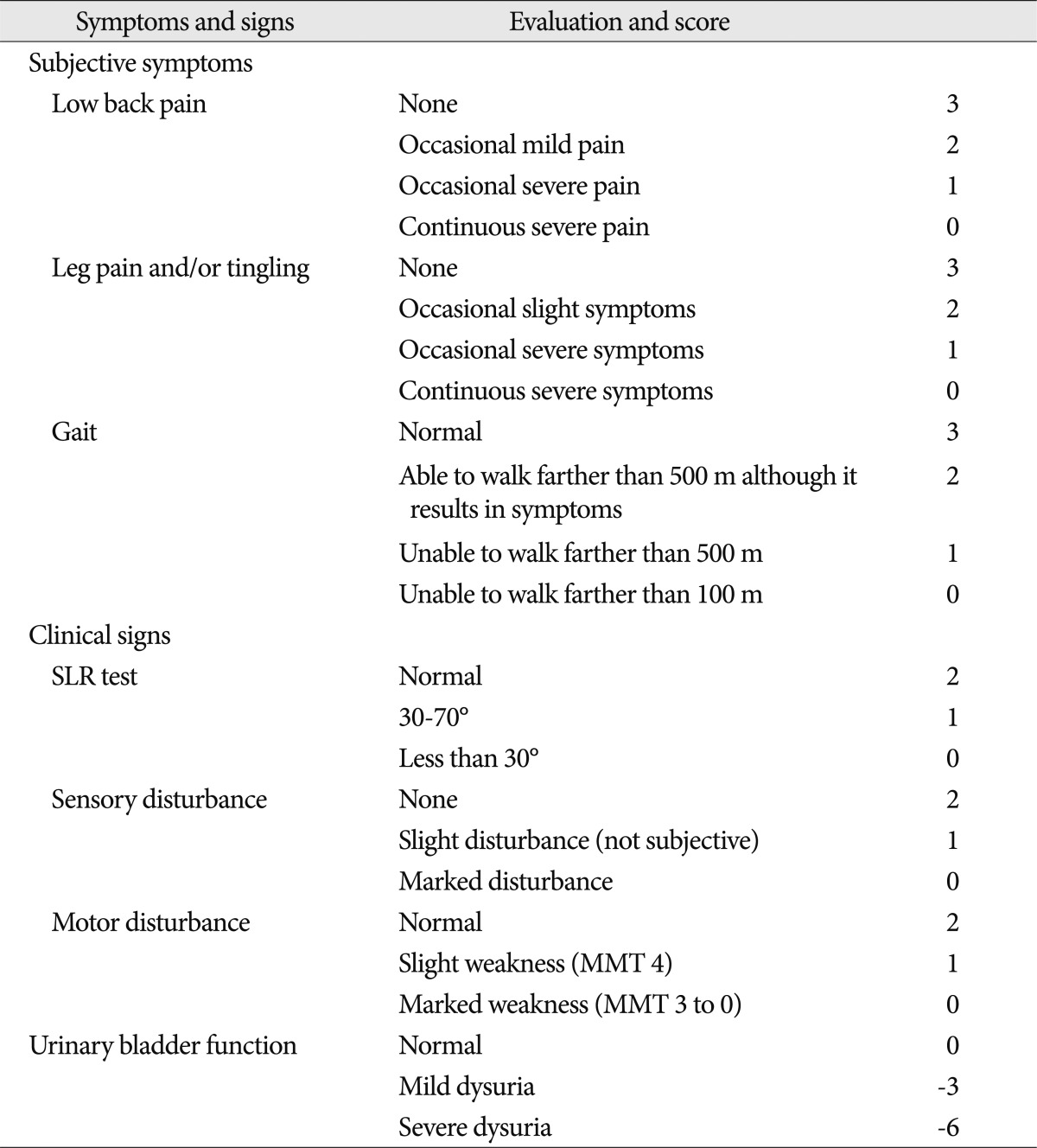
The Japanese Orthopedic Association (JOA) score for the low back pain syndrome (Table 3) was used to assess the clinical outcome. We have collected the clinical information preoperatively, and at 3, 6, 12, and 24 months post-surgery. The recovery rate was determined based on the final JOA score and allowed surgical outcomes to be rated as favorable (100-50%) or poor (49-0%).
Radiologic parameters and evaluation
We reviewed both preoperative and postoperative of whole spine lateral simple X-rays views. There are, however, several parameters to evaluate sagittal balance. We only focused on LL, PI and SVA. Preoperative LL was compared to the last follow-up LL. Because the PI has been known as constant value, we checked a preoperative value and applied it.
Postoperative change of disc height was measured by using a method which averages the sum of the measurements at the anterior and posterior disc regions3). We have obtained mean disc height calculations of each level during the immediate postoperative period, 1 year and 2 years after surgery. Cage subsidence was defined as a decrease in disc space height by more than 2 mm on the final follow-up radiograph. Each value was determined by two different neurosurgeons using the same method calculated an average.
All of the patients were check plain radiograph, but we could not check the computed tomography (CT) scan for all the patients. Although CT scan examination was more precise tool than plain radiograph for measuring disc space height, we have chosen the plain radiograph as tool of measuring the subsidence and suggested inter-observer reliability.
Statistical methods
All statistical analysis were performed using SPSS version of 12. Preoperative and postoperative group results were compared by using the paired t-tests. The p values of <0.05 were considered statistically as significant. Inter-observer reliability was calculated using an intraclass correlation coefficient (ICC) for LL, PI, SVA and disc space height. The ICC values were graded using criteria : excellent for values in the 0.90-1.0 range, good for 0.70-0.89, fair/moderate for 0.50-0.69, low for 0.25-0.49, and poor for 0.0-0.24.
Material
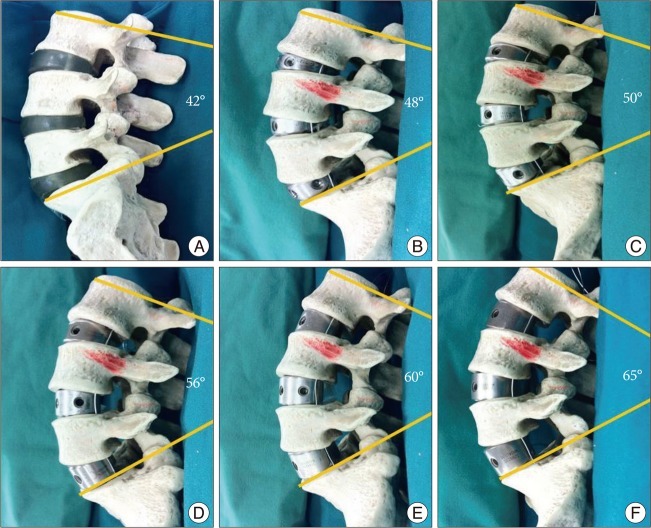
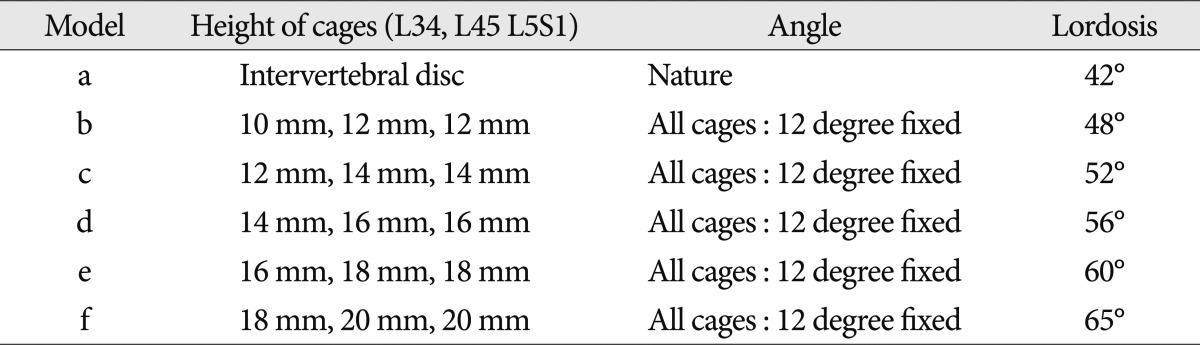
We regarded the multilevel ALIF not only as an interbody fusion but also building's story concept. We simulated through a plastic lumbar spine model which can get around easily. By insertion of the ALIF trial cage (different heights and 12 degrees fixed angle, Medtronics™), we checked the changes in segmental lordosis. We have applied this concept to the actual surgery and analysis to determine how much lumbar lordosis is needed to achieve an optimal sagittal balance during multi-level ALIF.
RESULTS
After analyzing the spinal model with the ALIF cage, those with a higher cage height had more lumbar lordosis (Table 4) (Fig. 2). The result showed that a widened disc space provides more posterior space and compression.
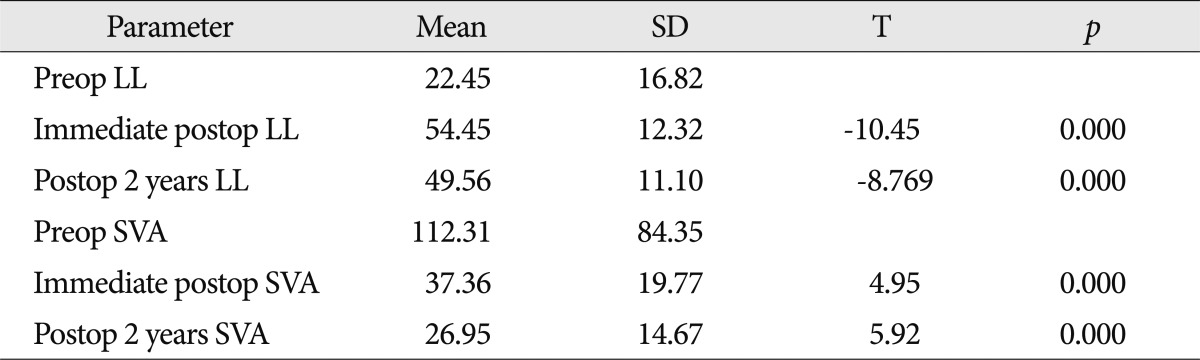
All patients underwent more than a two level ALIF. The mean preoperative LL and SVA values were 22.45 degrees and 112.31 mm, respectively. The mean pelvic incidence was 55.38 degrees. Immediate postoperative mean LL and SVA were 54.45 degrees and 37.36 mm. In addition, we have followed patients for at least 2 years and found mean LL and SVA to be 49.56 degrees and 26.95 mm, respectively. Inter-observer reliability analysis for measurement of PI, LL and SVA demonstrated ICCs of 0.87 (good reliability) 0.94 (excellent reliability) and 0.83 (good reliability), respectively.
The postoperative LL approximated pelvic incidence and was corrected to greater than 30 degrees compared to the preoperative LL after multilevel ALIF. Postoperative SVA was also corrected to less than 50 mm. Postoperative goals of both LL and SVA were achieved and we were able to obtain spinopelvic harmony (LL=PI±9, SVA <50 mm)20). Furthermore, preoperative and postoperative LL and SVA results were compared using paired t-tests with p values of <0.05 considered to be statistically significant (Table 5).
The mean immediate postoperative intervertebral disc height was 17.17± 2.09 mm, 17.24±2.49 mm, 18.90±2.47 mm at the L3/L4, L4/L5, L5/S1 levels, respectively. At the final follow-up visit, mean intervertebral disc height was reduced to 15.7±2.09 mm, 16.57±2.64 mm, 17.94±2.63 at each of the above spinal levels. Excluding operations at L2/L3 (5 levels), between 2008 and 2009 there were a total of 110 disc spaces subjected to the operation (L3/L4 : 31 levels, L4/L5 : 41 levels, L5/S1 : 38 levels). Cage subsidence was defined as a decrease in disc space height by more than 2 mm on the final follow-up radiograph. Using this definition, 25 of 110 disc spaces (22.7%) developed cage subsidence into the surrounding vertebral body. Inter-observer reliability analysis for measurement of disc height demonstrated ICCs of 0.78 (good reliability).
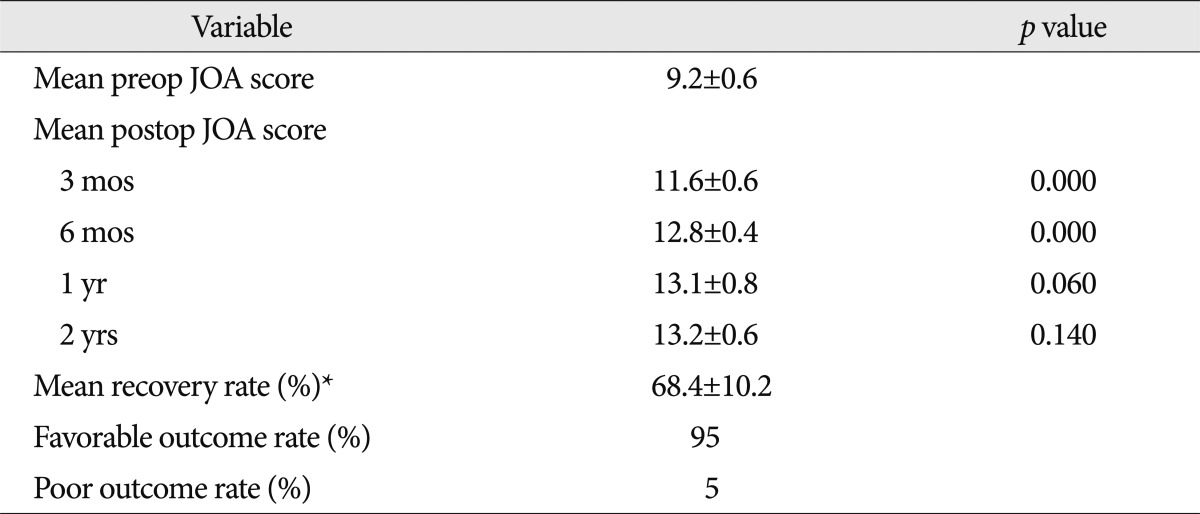
Clinical outcomes of the patients who underwent a multilevel ALIF were assessed by using the JOA score (Table 6), which allowed us to provide a summary of clinical outcomes in all patients. The pre-operative mean JOA score was 9.2±0.6 (±SD). There was a statistically significant difference between the preoperative and 3-month JOA postoperative score as well as a difference in the JOA at postoperative months 3 and 6 (p=0.000). The mean recovery rate was 68.4%±10.2% and a favorable outcome was seen in 40 patients (95%). A poor outcome was seen in only 2 patients (5%). Two years after surgery, the mean JOA score was 13.2±0.6 and represented a statistically significant difference from the preoperative score.
We had some patients who underwent the multilevel ALIF and we included one representative case of a patient suffering from degenerative lumbar disease.
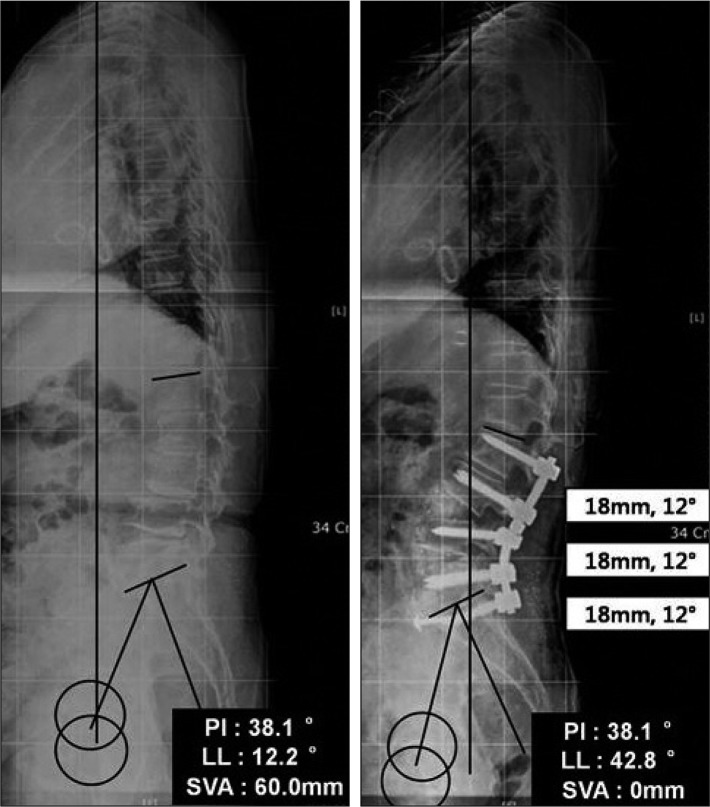
Case (F/66) (Fig. 3)
This patient suffered from low back pain which occurring from 15 years ago. Her pain was aggravated for one year and then it subsequently developed pain in both buttocks. She presented with a stooped posture and while performing housework she was frequently used her elbows for support, evidenced by skin hypertrophy. We diagnosed her with degenerative lumbar scoliosis, sagittal imbalance, and multilevel spinal (foraminal) stenosis at levels L3, L4, and L5. We offered her a surgical solution and we then performed a two-stage operation. The first stage of the operation included L5 posterior decompression, posterior screw fixation (levels L3, L4, L5 and S1), and V-osteotomy (levels L3, L4 and L5). The second stage of the operation was ALIF at levels L3/L4, L4/L5 and L5/S1 and rod instrumentation and compression allowing us to achieve optimal spinopelvic harmony and sagittal balance.
DISCUSSION
ALIF is a valuable technique with numerous advantages for spinal surgery. ALIF allows the expansion of disc space and foraminal height, as well as restoration of lumbar lordosis and spinal alignment without compromising posterior tension bands.
ALIF is the best method to restore foraminal height, segmental lordosis, and disc space height and has potentially improved sagittal balance and leads to better long-term outcomes compared to transforaminal lumbar interbody fusion8). In certain situations the canal and neural foramen may be indirectly decompressed and thus avoiding possible injury to the nervous system.
By accessing the lumbar spine through an anterior approach, we were able to achieve excellent anterior column exposure, with less muscular retraction, blood loss, and a shortened operative time. The complete removal of intervertebral discs allows for greater retraction of disc spaces, allowing for the insertion of large interbody devices for deformity correction.
Despite these advantages, some disadvantages to the procedure do exist. According to McDonnell et al.11), 11% of patients who underwent ALIF experienced major complications while 24% experienced minor complications. These unique complications are not seen in conventional surgery and include injuries to abdominal wall structures, great vessels, ureters, and numerous nerve plexuses.
The most harmful complication is vascular injury with reported frequencies ranging from 1% to 24%7). Specifically, the most common type of vascular injury is venous laceration the iliac vein, inferior vena cava and iliolumbar vein from vessel retraction. Arterial injuries occur less frequently than venous injuries due to their greater elasticity and mobility. Injuries to the left iliac artery and aorta injury are rare, occurring in less than 1% of cases10). There is also a risk of retrograde ejaculation from superior hypogastric plexus injury with a reported incidence occurring in 5.9-8% of cases7,11). Finally, lymphocoele formation is an additional serious but exceedingly rare complication19).
While complications of AILF may be more numerous when compared with the posterior spine surgical procedures recent efforts by many surgeons have been aimed at avoiding complications and have yielded many articles regarding safer techniques and have revealed intra-abdominal improved surgical approach8,9,24). Consequently, ALIF is a less demanding and dangerous procedure.
Many authors have reported on the disadvantages of disc space height reduction after ALIF and suggest subsidence will adversely affect foramen size and mechanical deformity correction3,6,18). Decreased disc space height after ALIF may lead to mechanical stresses such as increased intradisc pressure, intersegmental rotation, and contact force of facet joints.
Maintaining disc space height and segmental lordosis is important for preventing subsidence and adjacent segment degeneration23). In the present study, we have been applying a cage higher than 16 mm for all patients. Considering that we were able to maintain disc space height we possibly prevented subsidence. Moreover, obtaining a negative sagittal vertical axis and bending the spine posteriorly reduced anterior column stress force and provided a biomechanical load sharing effect. In this study, subsidence rate was 22.7% and the final follow-up lumbar lordosis was relatively maintained to approximately PI. Clinical studies have reported a wide range of subsidence occurrence, some studies of ALIF using a stand alone cage revealed subsidence rates of more than 40%4,21) while other studies have reported posterior and transforaminal lumbar fusion subsidence rates of 26.5%5). Compared to previous reports, our procedure has the potential to reduce the rate of subsidence.
CT scan is more favorable tool to reduce inter-examiner bias for measuring the disc space height than plain radiograph. Because the CT scan was not checked routinely for all the patients, we only measured the subsidence by using the plain radiograph. Inter-observer reliability analysis for measurement of disc height by using plain radiograph demonstrated ICCs of 0.78 (good reliability). Further comparative study of subsidence rate by using CT scan in our center may suggest more reliable result and need to be done.
Our operation procedure had two stages in all patients. The first stage was a posterior facet release and pedicle screw fixation; the second stage was an anterior approach for interbody fusion and a posterior approach for achieving sagittal and coronal balance by rod insertion. One week after the first stage operation, all patients underwent a second stage operation. We named this method a posterior-anteroposterior (P-AP) approach. Single stage operations of the same procedure require a longer operating time and may have more blood loss at one time. Mean operation time of the first stage and second stage was approximately 2.5 hours and 4 hours, respectively. In our center, mean operation time of a single stage operation was approximately 7 hours. Although the total time required for a two stage operation was similar to a single operation, each time interval was shorter. Prolonged surgical times may increase risks of surgical site infection16). Therefore we suppose that two stage operation (P-AP approach) may reduce the risk of surgical site infection compared to single stage operations. In our procedure, the mean estimated blood loss for the first stage of the operation was approximately 800 mL and 500 mL for the second operation. Recently reported blood loss over 1 L is now considered to be a significant independent risk factor for perioperative infection16). In our cases, the intraoperative blood losses were less than 1 L and with no surgical site infections. However, this observation was not part of our study and we do not have statistics to confirm our observations. Additional analyses are needed to define the advances of the P-AP approach.
There is another advantage of a P-AP procedure. We performed a first stage operation to remove posterior spinal structures such as facets, the ligament flavum and ligaments surrounding the facet followed by a rest period of one week. This period provided more release of posterior structures and spontaneously corrected the kyphoscoliosis. Moreover, the release of the posterior structures gave us an opportunity to raise the cage height in the anterior disc space.
In some cases involving L5 and S1, we used an anchoring, cancellous screw in the anterior vertebral body because L5-S1 is the junction of the lumbar and sacral spine segments and has a larger slipping force compared to other spinal segments (Fig. 3).
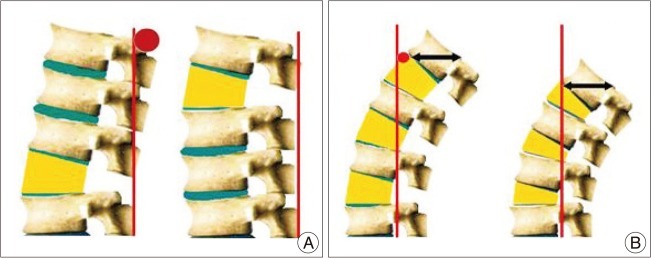
During this study we found that using a higher cage and inserting the cage at lower levels allowed for the achievement of optimal sagittal balance which can be explained and visualized by simple spine modes (Fig. 4).
CONCLUSION
According to our study, the patients who underwent multilevel ALIF by the same angled cage could obtain postoperative LL (49.56±11.1 degrees) equal to the pelvic incidence (55.38±3.35 degrees). The postoperative SVA was also corrected to less than 50 mm and we have obtained satisfying result of spinopelvic harmony measurements (LL=PI±9, SVA <50 mm).
Using the spine models, higher cage at a lower level could provide more lordosis.
We also suggest that a P-AP approach is beneficial to achieve the desired sagittal balance. Further comparative studies of the P-AP approach are needed to be done and should be compared to single stage operations.
 XML Download
XML Download