

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Several studies have investigated the quality of life (QOL) after treatment for patients with intracranial aneurysms4,17,21). Many factors including the aneurysm origin, age and sex of the patient, neurological condition upon admission, extension of the hemorrhage, physical handicap, the presence of depression, cognitive impairment, the Glasgow Outcome Scale (GOS) and sleep problems were found to be associated with the QOL of patients who underwent cerebral aneurysm surgery1,5,6,7,10,16,20).
Recently, in QOL assessments, there has been growing interest in the individual's subjective feelings on life aspects. With regards to the outcome assessment of the patients treated with intracranial aneurysms, a single graded scale such as the GOS, modified Rankin Scale, Barthel Index and the National Institutes of Health Stroke Score may not necessarily address all of the aspects of recovery, especially cognition and the patient's perception of health9). Therefore, although the patients may have good neurological outcomes and possess cognitive function after intracranial aneurysm surgery, they may still have the potential to experience a poor QOL. In addition, the treatment modalities of the intracranial aneurysms, especially endovascular procedures or minimally invasive operations, have evolved considerably in recent years. The rates of mortality and morbidity related to the surgical or endovascular treatment of ruptured or unruptured intracranial aneurysms have also decreased substantially3,8,13). However, the QOL of aneurysm patients treated with minimally invasive methods has not yet been evaluated.
Min et al.11) developed the World Health Organization Quality of Life (WHOQOL) instrument-Korean version, which has 100 detailed items; however, this instrument has not been validated and used to evaluate patients with cerebrovascular diseases but general Korean populations.
This study aimed to investigate the QOL of patients who underwent anterior circulation aneurysm surgery and had a good outcome by validating and using the WHOQOL instrument-Korean version. Moreover, the study also focused on the identification of contributing factors associated with surgical methods in the patient's perception of health.
MATERIALS AND METHODS
Study design and patients
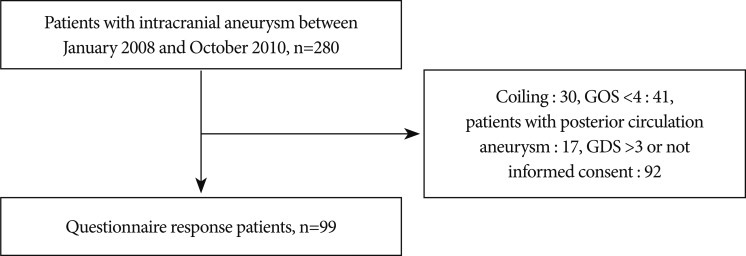
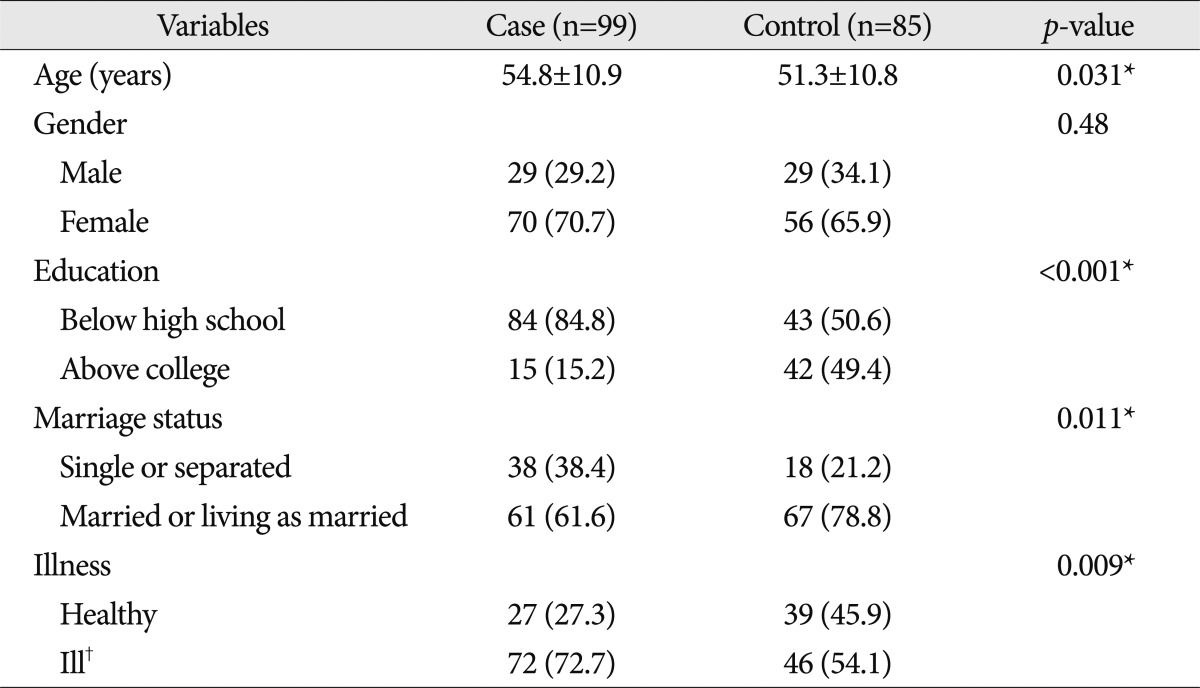
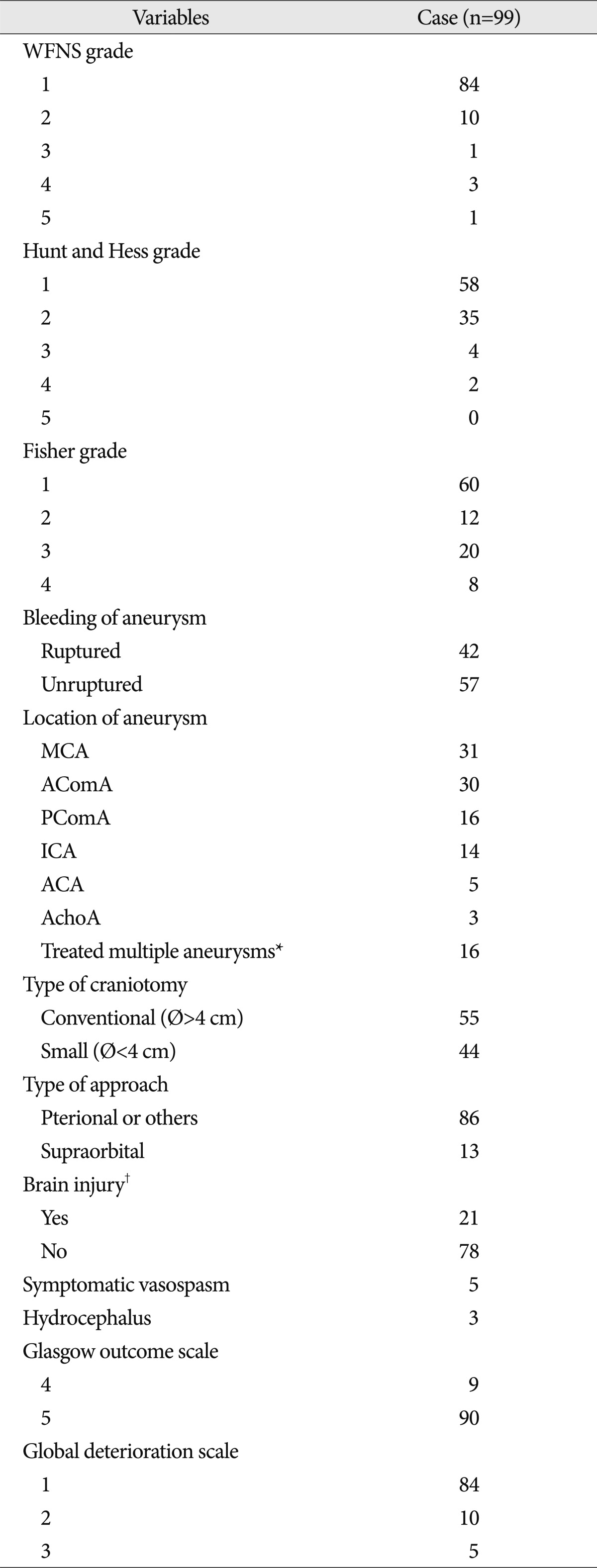
This study was a retrospective case - control study where the participants were recruited from a single center. The source population consisted of aneurysm patients from our institute who underwent surgical treatment between September 2008 to October 2010. Patients who were newly diagnosed or patients who were surgically treated for an anterior circulation aneurysm and showed a good neurological outcome at 6 months after surgery were selected. A good outcome at 6 months was defined as the following : GOS score ≥4 and a global deterioration scale (GDS) score ≤3. The exclusion criteria were patients with a poor outcome, patients who exhibited a posterior circulation aneurysm, and patients who were treated with a coil embolization or did not provide their informed consent. Out of a total of 280 patients with 290 intracranial aneurysms, 181 patients were excluded (31 coiling patients, 17 posterior circulation aneurysm patients, 41 patients with GOS less than 3, and 92 patients with GDS greater than 3 or were without informed consent) (Fig. 1). The final number of aneurysm patients included in this study was 99. The total number of control subjects was 85, which included the hospital staff, their family and acquaintances, and the patients' families (the demographic data are described in Table 1). The QOL values and clinical factors associated with QOL such as age, sex, education, marriage status, illness, World Federation of Neurosurgical Societies (WFNS) grade, Hunt and Hess grade, Fisher grade, brain injury, rupture of the aneurysm, craniotomy size, surgical approach and hospital charges were assessed in either the case or control groups (Table 1, 2). This study was approved by the local institutional review board.
Surgical methods and outcome evaluation
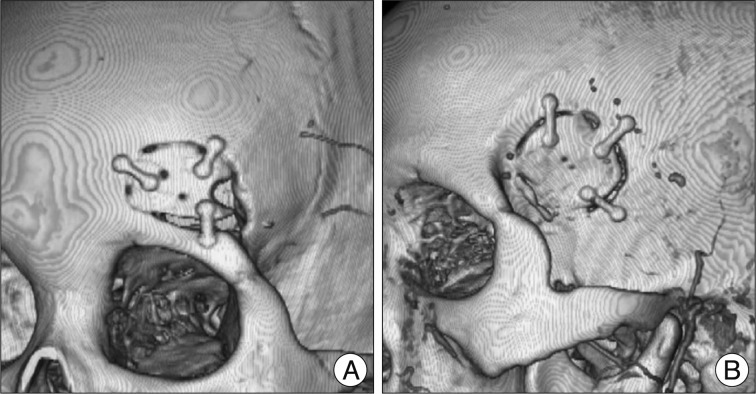
During the study period, all of the operations were conducted by one cerebrovascular team, and the surgical approach was determined according to the aneurysm site, dome direction, control of the parental artery, hemorrhage volume and site, brain swelling and the patient's or surgeon's preference. A conventional craniotomy was defined as a standard pterional craniotomy as described by Yasargil and Fox24) or by a bifrontal craniotomy of the distal anterior cerebral artery aneurysm or anterior communicating aneurysm with or without extraventricular drainage. A supraorbital craniotomy was conducted via an eyebrow skin incision as previously described by Perneczky et al. (Fig. 2A)18,19). Recently, one study reported a microsurgical experience using supraorbital keyhole operations on anterior circulation aneurysms15).
However, the supraorbital keyhole operation has several limitations in its effectiveness, particularly with some cases of the middle cerebral artery (MCA) bifurcation aneurysms, where the M1 segment is too long or there is a lateral and caudal direction of their aneurysm domes, supraclinoid internal carotid artery (ICA) aneurysm, or posterior communicating artery (PComA) aneurysm with posteroinferior projection2,14). Nathal and Gomez-Amador14) previously described a sphenoid ridge keyhole approach for cerebral aneurysms that also has several limitations including the limited opening of the sylvian fissure to increase the tendency towards a more significant brain retraction. We have performed a modified small pterional craniotomy with a similar skin incision as the conventional pterional craniotomy but with a subfascial muscle dissection. A single burr hole was made at the point 3-4 cm posterior from the frontozygomatic point and 1 cm ventral from the superior temporal line of the skull, using a high-speed drill. A dural dissector was used to separate the dura mater from the bone, particularly in elderly patients, to avoid dural tearing during sawing. The margin of the craniotomy forms a superior boundary up to the superior temporal line and inferiorly to the temporal bone. The center of the craniotomy could be moved towards the frontal or temporal lobe depending on the direction of the intradural surgical trajectory towards the target aneurysm (Fig. 2B).
We divided the craniotomy types according to size into conventional craniotomy of which the minimum diameter was greater than 4 cm and small craniotomy, which was characterized by a supraorbital or frontotemporal craniotomy of which the maximum diameter was less than 4 cm (Fig. 2). The surgical methods consisted of two approaches : the supraorbital approach and the pterional/others approach. All of the patients' profiles were assessed by a retrospective chart review, and the patients' neurological outcomes were evaluated at the time that the questionnaire was obtained. The craniotomy size was measured in the postoperative brain using a 3-dimensional multi-detector CT scan. The brain injury, however, was identified only as a low density lesion that was more than 1 cm according to a postoperative CT image taken within two weeks.
Instruments and calculation of scores
QOL was evaluated using the WHOQOL instrument-Korean version, which was previously validated by Min et al.11). This questionnaire measures the patients' general health across six dimensions : 1) physical domain (PHY), 2) psychological domain (PSY), 3) levels of independence (IND), 4) social relationship (SOC), 5) environmental domain (ENV), and 6) spiritual domain (SPI). The overall QOL score was the sum of the questions regarding global QOL. Each of the domains consisted of 8-16 questions and addressed 1-4 facets. The facet scores for the WHOQOL were calculated by the mean of all of the items included in each facet according to the description of the WHOQOL group. The domain scores were also calculated by multiplying the mean of all of the items included within the domain by four, and items proposed in the negative form were calculated by subtracting the given score from 623). The potential scores for all of the domain scores were 6 to 20, and all of the scores were transformed based on a scale that ranged from 0 to 100 as an equation of [(raw score-4)/16]×100.
Statistical analysis
All of the independent predictors including age, sex, education, marriage status, illness, brain injury, presence of subarachnoid hemorrhage, craniotomy size, surgical approach and hospital charges were assessed and included in the statistical analysis. The dependent variables were the transformed scores of the 6 domains, 24 facets and total scores. First, all of the variables were compared between the case and control groups using the chi-squared test and t-test. Second, a reliability analysis using Cronbach's alpha and Pearson's correlation of the WHOQOL Korean version in both the patients and the control subjects was performed. Further analysis of the QOL value differences between the case and control subjects was conducted following an adjustment of the baseline differences using multivariate analysis. A subgroup analysis of the QOL values according to the presence of the subarachnoid hemorrhage, brain injury, craniotomy size and surgical approach was also conducted. In unruptured aneurysm patients, the QOL values according to craniotomy size were also compared with t-test. To evaluate the random effects in this study regarding the QOL in patients with an anterior circulation aneurysm and a good outcome, the differences of the hospital charges according to the contributing factor of the QOL in this population was compared using the t-test. A p value of less than 0.05 was considered significant using two tailed statistics. The data analyses were performed using Statistical Analysis System version 9.1.2.
RESULTS
General characteristics
Gender was not significantly different between the case and control groups. However, the case group was significantly older, less educated, and had a higher percentage of solitary life or illness (Table 1). In this study, 16 of the 99 patients had two aneurysms, and they were all surgically treated with a single craniotomy and surgical approach. Most of the patients initially showed a favorable neurological status with a WFNS grade of less than 2 (94%) and a Hunt and Hess grade of less than 2 (93%). There were 42 patients with ruptured aneurysms and the location order of the aneurysms were as follows : MCA, anterior communicating artery, PComA, ICA, anterior cerebral artery and anterior choroidal artery. A conventional craniotomy was performed on 55 patients, and a small craniotomy was performed on 44 patients. The pterional approach was used in 86 patients, and the supraorbital approach was performed in 13 patients. A brain injury was defined as a low density of more than 1 cm in the immediate postoperative brain CT scan. A symptomatic vasospasm was found in 5 patients and a hydrocephalus ventriculoperitoneal shunt was required in 3 of the patients. The GOS at 6 months was 4 in 9 patients and 5 in 90 patients. In contrast, the GDS at 6 months was 1 in 84 patients, 2 in 10 patients and 3 in 5 patients (Table 2).
Reliability and validity of the WHOQOL Korean version
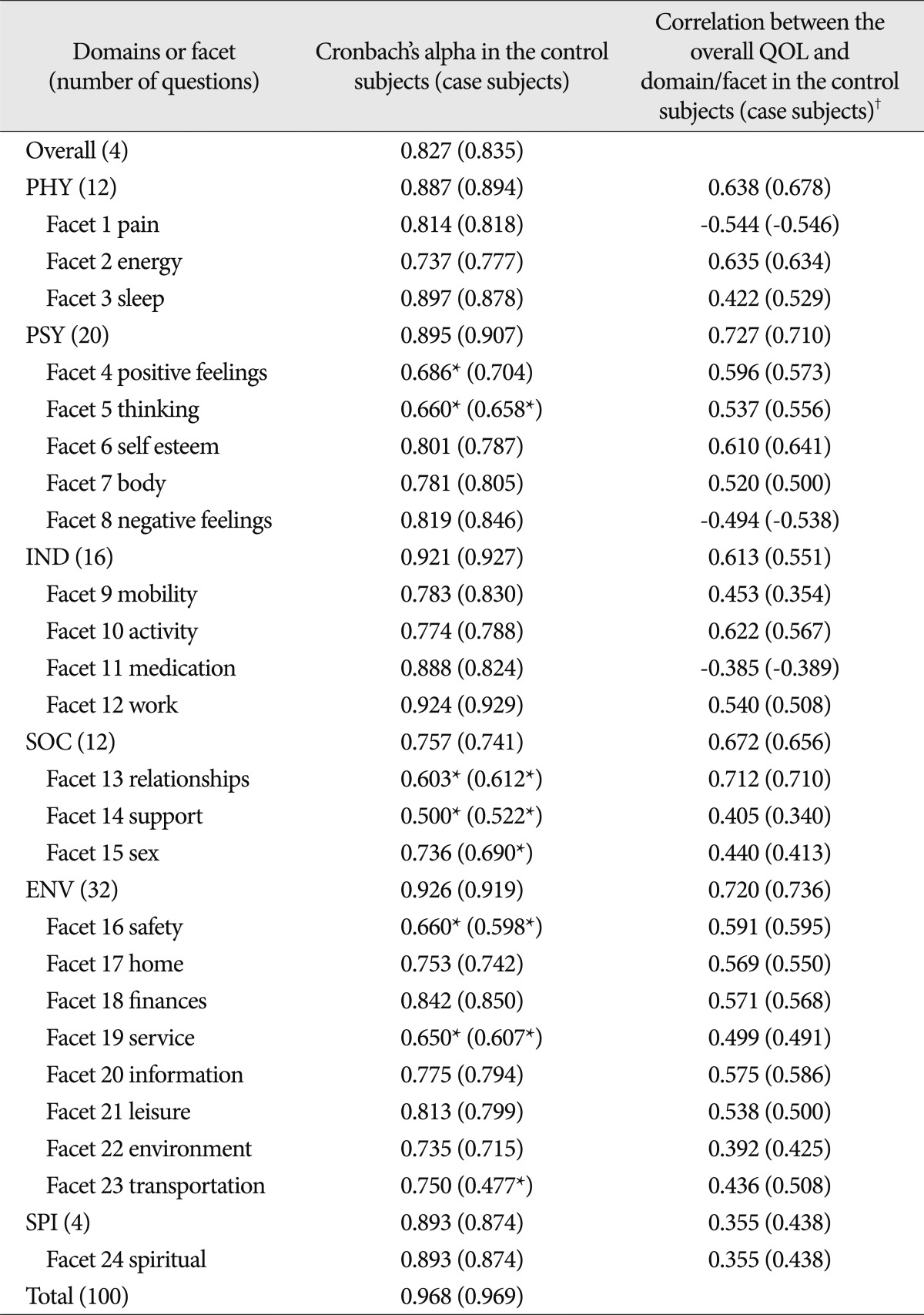
The internal consistency and construct validity of the WHOQOL Korean version of the patient case and control subjects are given in Table 3. The Cronbach's alpha values for the total score were 0.968 and 0.969 in the control and patient case subjects, respectively. The alpha value for the domain and facet score ranged from 0.500 to 0.926 in the control subjects and 0.477 to 0.927 in patient case subjects. The alpha value for all of the domains was higher than 0.7 in the control and patient case subjects. Facet 4 (positive feelings), facet 5 (thinking), facet 13 (relationships), facet 14 (support), facet 16 (safety) and facet 19 (service) revealed that Cronbach's alpha was less than 0.7 in the control subjects. Facet 5 (thinking), facet 13 (relationships), facet 14 (support), facet 15 (sex), facet 16 (safety), facet 19 (service) and facet 23 (transportation) showed alpha values of less than 0.7 in the control subjects. The Pearson correlation between the domain scores and the overall QOL ranged from 0.355 for the SPI to 0.720 for the ENV in the control subjects and 0.438 for the SPI to 0.710 for the PSY in the patients, which suggests a statistically significant correlation in the control subjects (p<0.0001). The correlation coefficient in the patient case subjects between the domain and the overall QOL scores ranged from 0.438 and 0.710 for the SPI and PSY, respectively.
Comparison of QOL values in the case and control groups
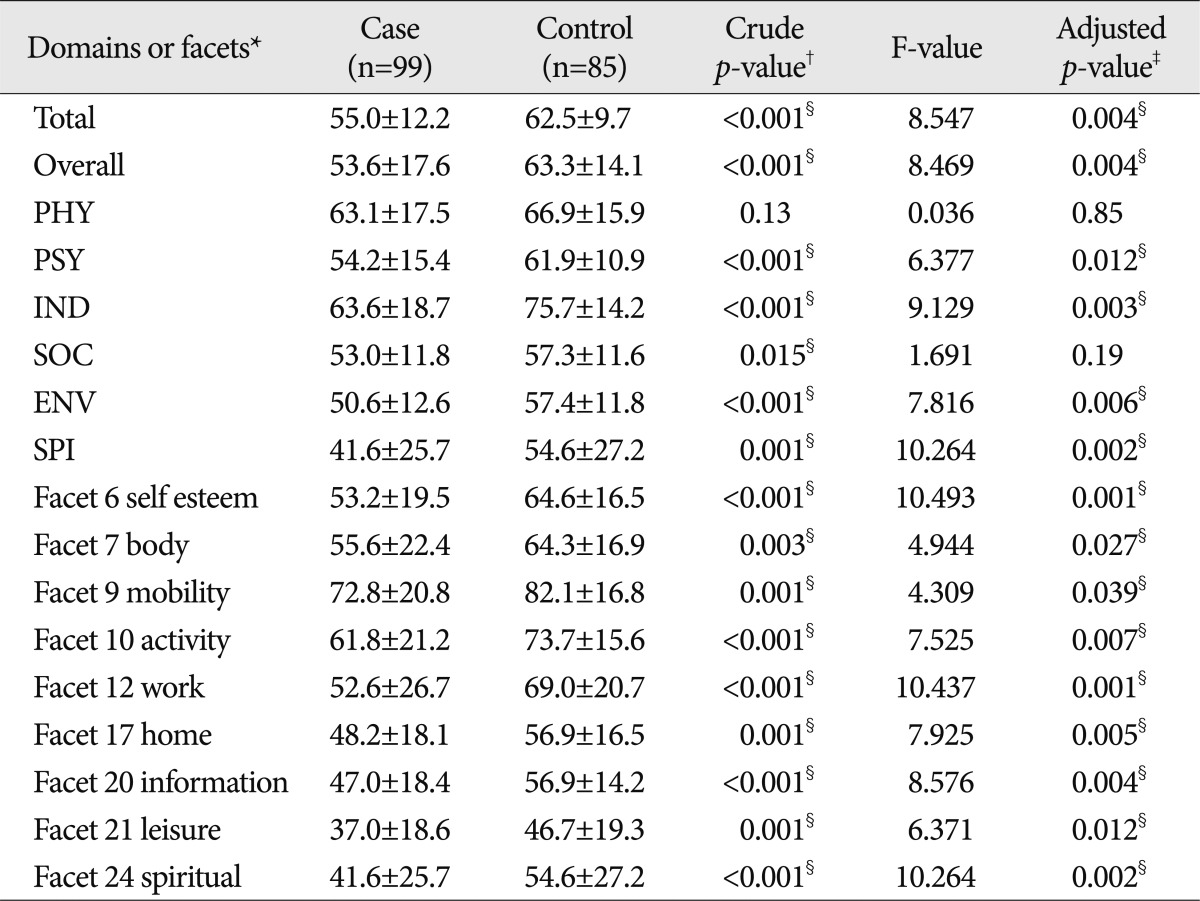
The total QOL values of the case group were significantly lower than that of the control group (p=0.004). The overall QOL scores and QOL scores of all of the domains, with the exception of the PHY and SOC in the case group, displayed significantly lower values than in the control group (Table 4). On the facet level, after an adjustment of all of the independent variables including age, education, marriage status and illness, facet 6 (self esteem), facet 7 (body), facet 9 (mobility), facet 10 (activity), facet 12 (work), facet 17 (home), facet 20 (information), facet 21 (leisure) and facet 24 (spiritual) in the case group were significantly lower than the control group (Table 4).
Subgroup analysis of the QOL values and hospital expenses in the case group
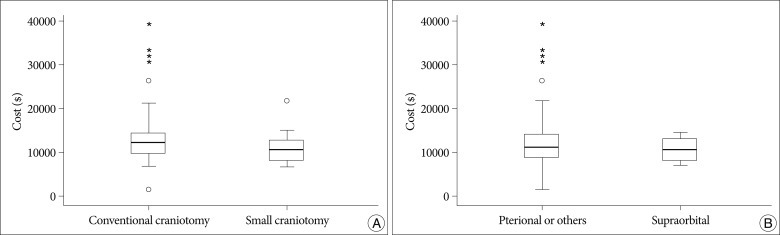
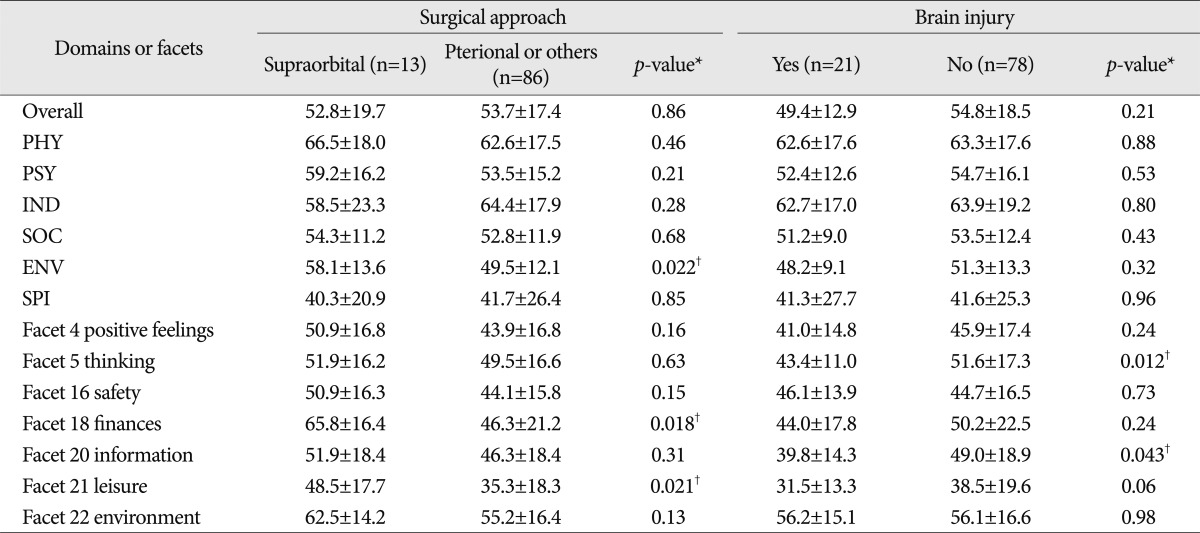
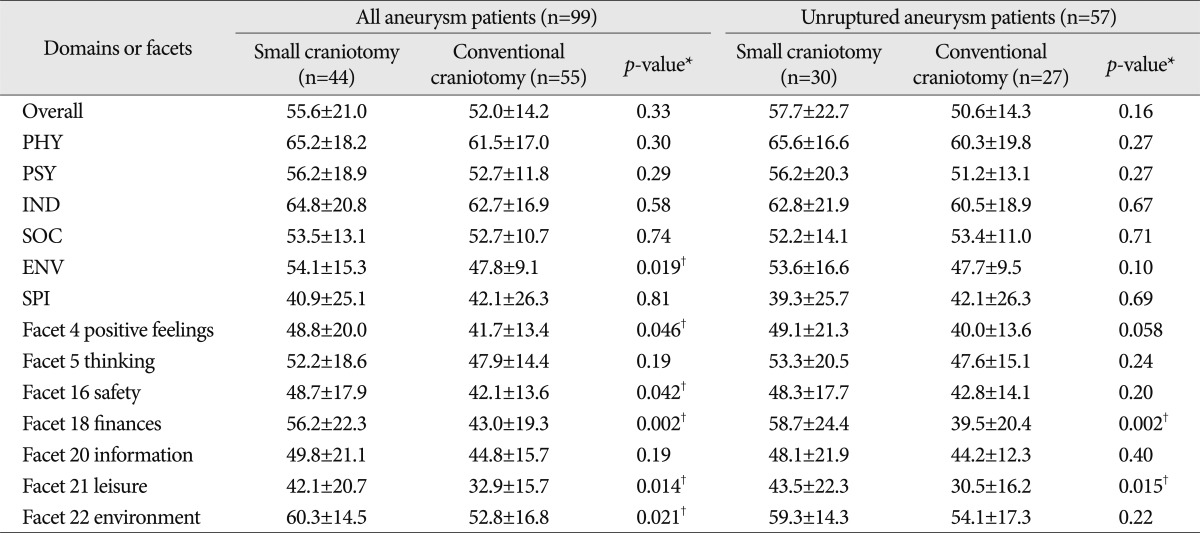
When the aneurysm patients were classified according to aneurysm rupture, there was no difference in any domain and facet between the ruptured and unruptured groups (not shown in Tables). With the exception of facet 5 (thinking) and facet 20 (information), the aneurysm patients with brain injury demonstrated lower QOL values than subjects without brain injury (Table 5). At the analysis for the whole aneurysm patients, according to the craniotomy type and surgical approach, the values for the total QOL, overall QOL and all of the domains except for the ENV were not significantly different. The QOL values for the ENV were higher in the small or supraorbital group than in the conventional or pterional/others group (Table 5, 6). The supraorbital group revealed higher values in the facet 18 (finances) and facet 21 (leisure) than the pterional/others group (Table 5). The small craniotomy group showed higher values of QOL in facet 4 (positive feelings), facet 16 (safety), facet 18 (finances), facet 21 (leisure) and facet 22 (environment) than in the conventional craniotomy group (Table 6). However, at the analysis for only the unruputred aneurysm patients, there was a significant difference between two groups according to craniotomy size in facet 18 (finances) and facet 21 (leisure) (Table 6). Of the total expenses paid for treatment during the hospitalization period, the patients who underwent a small craniotomy paid lower hospital charges than those treated with a conventional craniotomy (p=0.006), while the patients treated with the supraorbital approach did not have lower hospital expenses than those treated with the pterional/others surgical approach (p=0.25) (Fig. 3).
DISCUSSION
Min et al.11) first validated the WHOQOL instrument-Korean version, which has not been used for the evaluation of QOL in patients with cerebrovascular disease. In this study, the WHOQOL instrument-Korean version was first used to assess the intracranial aneurysm patients treated with clipping surgery. Consistent with previous results of QOL in the general Korean population, our study showed greater alpha values than 0.7 for all of the domains in both the control and case subjects, while facet 5 (thinking), facet 15 (sex), facet 16 (safety) and facet 23 (transportation) fell below 0.7, including facet 13 (relationships), facet 14 (support) and facet 19 (service), which were lower than the results obtained by Min et al.11). The Pearson correlation between each domain and the facet scores in both the overall QOL and the domain/facet was significantly high. Consistent with the results of Min et al., the correlation value for the SOC between the overall QOL and domain was relatively low in the control and case subjects (0.355 and 0.438, respectively). Therefore, the WHOQOL Korean version may be valid and reliable for the assessment of QOL in patients with an anterior circulation aneurysm.
Although the patients showed good GOS and GDS scores, patients treated with anterior circulation aneurysms regardless of subarachnoid hemorrhage demonstrated lower QOL scores for the total, overall, PSY, IND, ENV and SPI scores compared with normal control subjects (Table 4). These findings suggest that the QOL in aneurysm patients with neurologically good outcomes is an important outcome indicator, which is consistent with the findings of Kim et al.9). In addition, the subgroup analysis revealed a contrast with previous studies of intracranial aneurysm patients regarding their QOL according to surgical methods. We found that the smaller the craniotomy size, the better the ENV score. Our results also showed a better score for the ENV in the supraorbital group compared with the pterional/others group (Table 5). Regarding facets, facet 18 (finances) and facet 21 (leisure) were significantly different according to the type of craniotomy and surgical approach in anterior circulation aneurysm patients regardless of exclusion of subarachnoid hemorrhage patients (Table 5, 6). The hospital expenses did not show a significant difference according to the surgical approach, bleeding of the aneurysm and brain injury, while in the small craniotomy group, the patients had less expensive hospital charges during their admission period (Fig. 3). Therefore, these findings suggest that the differences in the QOL according to the craniotomy type may not result from random effects. Interestingly, patients with brain injury showed a low score for facet 5 (thinking) and facet 20 (information). This finding indicates that the WHOQOL instrument is a very sensitive tool for patients with mild cognitive dysfunction.
Recently, studies have reported that limited craniotomies require minimal brain retraction and thus significantly decrease approach-related morbidity2,12,14,15,19). However, the safety and efficacy of keyhole craniotomy is still controversial because of the uncontrollability of the insurmountable brain swelling at the opening the dura and the inability to perform partial or complete lobectomies22). We performed a modified small pterional craniotomy on patients with anterior circulation aneurysms, which is unlike the pterional keyhole approach14). Regardless of the surgical approach, the craniotomy size may affect the QOL of aneurysm patients, especially in the environmental domains including finance and leisure.
Our research showed additional beneficial aspects of minimally invasive operations, but there are several limitations of the study design, including the low participation rate, small sample size and the retrospective review. In spite of multivariate analysis, as there was not a matched sampling of control groups, therefore, we should consider the sampling bias. In the future, a prospective randomized study regarding the safety and efficacy of minimally invasive operations for anterior circulation aneurysms will be required.
CONCLUSION
The WHOQOL instrument-Korean version is a useful tool for the measurement of QOL in patients who were surgically treated for intracranial aneurysms. The QOL in patients who experienced an anterior circulation aneurysm surgery, despite having a good neurological outcome, was low in all of the domains except for the physical and social domains. The craniotomy size may affect the QOL in patients who underwent an anterior circulation aneurysm surgery and had a good outcome.
 XML Download
XML Download