

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
During carotid neck surgery, meticulous dissection technique and detailed anatomical knowledge must be applied in order to avoid injuries of neurovascular structures surrounding the carotid artery. Extracranial hypoglossal nerve injuries were not uncommon and occurred in 2-17% of cases7). The sternocleidomastoid (SCM) artery plays a role to identify the hypoglossal nerve during carotid neck surgery but its origin sites are various13). The aims of our research are to describe the SCM artery originated from the lingual artery and to review its clinical importance.
CASE REPORT
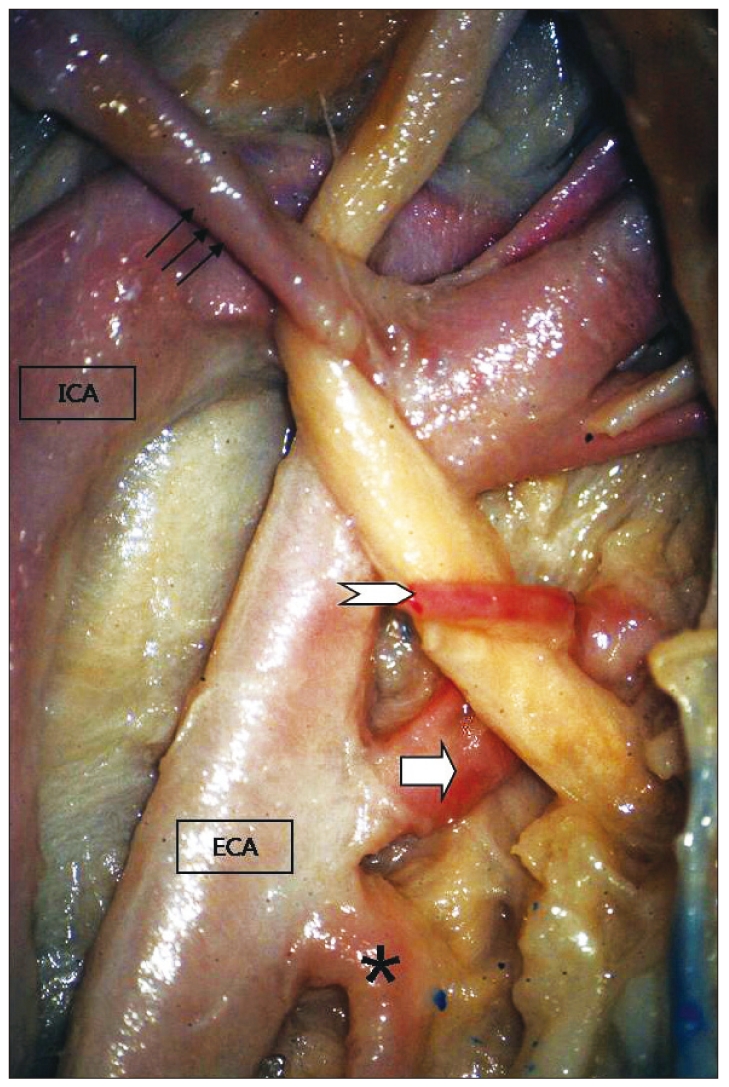
Carotid neck dissection was performed on a formalin-fixed adult cadaver head. Specimen was fixed in 10% formaldehyde solution. Anatomical specimen was examined using 10× magnifications with a Lexica (St. Louis, MO, USA) surgical microscope. This case showed that the SCM artery originated from the lingual artery and it crossed over the hypoglossal nerve (HN) (Fig. 1). The distance between carotid bifurcation and the lingual artery was 14.8 mm. The course of the HN was parallel to ECA. The distance between carotid bifurcation and the HN over the ECA was 21.7 mm. The distance between carotid bifurcation and the HN over the ICA was 26 mm. The carotid bifurcation was located at the level of 5th cervical vertebra. This case showed that the SCM artery displaced the HN inferiorly, and the arterial loop over the HN was very close to the carotid bifurcation.
DISCUSSION
During carotid neck surgery, it is very important to know anatomical details in order to avoid neurovascular injuries. Because of various neurovascular courses surrounding the carotid artery in the neck, numerous extracranial cranial nerve injuries have been reported with an incidence rate of 3-47.5%4,15,16). Among those injuries, hypoglossal nerve injuries were most common7). Even though the HN has various running courses in the neck, different landmarks have been proposed to recognize the level of the HN1-3,5,12,13,17,20). Characteristic vascular loop crossing over the HN is mainly made by the OA itself or the SCM artery originated from the OA. The SCM artery as well as the occipital artery plays a role as a good landmark for the identification of the HN but the origin site of the SCM artery is not always consistent13). Antonius et al. and Luis BF et al. reported that the blood supply to the SCM muscle can be categorized into 3 parts : upper, middle, and lower8,11). The upper third of the SCM muscle was found to be constantly supplied by branches of the occipital artery. The middle third of the SCM muscle receives its blood supply from a branch of the superior thyroid artery (42%), the ECA (23%), or both (27%). In most cases, the lower third is supplied by a branch arising from the suprascapular artery (>80%). In this case, the SCM artery supplying the middle part of the SCM muscle originated from the lingual artery; it is extremely rare case. Antonius et al. reported only one case during 31 necks (61 preparations) dissection11). The lingual artery (LA) is one of the main arteries supplying the tongue and the floor of the mouth. It usually originates from ECA at the level of the posterior tubercle of the hyoid bone19). It also originates from the superior thyroid artery in 1-2%10,18). In 10% to 20% of cases, the LA shares a common trunk with the facial artery, typical from 4 branches : suprahyoid branch, dorsal lingual branch, deep lingual branch, and sublingual artery14). The LA also has various levels on the ECA13): average distance from the carotid bifurcation to the lingual artery was 9.99±6.60 mm on the right side and 12.63±8.36 mm on the left side. In total, 4 cases showed that the lingual artery was level with or lower than the carotid bifurcation13). In general, the LA is not a limiting factor in exposing the carotid bifurcation during carotid neck surgery. However, if vascular loop by the SCM artery originated from the LA go over the HN, displacing and positioning the HN inferiorly like this case, we should take into consideration in order not to injure the HN because the location of the HN hooked by the SCM artery arising from the LA was closer to the carotid bifurcation than in the case where the SCM artery arising from the OA crossed over the HN. We also found that the carotid bifurcation was located at the level of C5 vertebra on fluoroscopy, relatively lower than in the usual cases. The level of the carotid bifurcation is variable, but by means of angiography, the carotid bifurcation is usually located at the level of C46), whereas anatomically, the bifurcation is most frequently located at the level of the disc between C3 and C49). In general, if the level of the carotid bifurcation is relatively low, the risk of the HN injury can be low. However, if the HN is displaced and positioned inferiorly by the SCM artery from the lingual artery like this case, the HN injury can occur more easily during carotid neck surgery.
 XML Download
XML Download