

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lumbar spondylolysis is common phenomenon, reported around 3-6% in the general population2,10,36). Although most of lumbar spondylolysis are asymptomatic, however it could cause chronic back or leg pain. Symptomatic lumbar spondylosis which does not respond to long-term conservative treatment requires surgical intervention.
For surgical treatment of lumbar spondylolysis, the conventional arthrodesis such as posterior interbody fusion or posterolateral fusion has been performed. The arthrodesis of pathologic segment eliminates the segmental motion, and may accelerate adjacent segment degeneration5,22,27).
Kimura18) noted surgical method putting bone chips into the defect of pars in 1968, and since then various kinds of direct pars repair surgeries have been introduced1,7,8,11,13,16,25,29,31,32). Direct pars repair could reconstruct the posterior spinal bony structure and preserve the segmental motion. However, depending on the surgical methodology, there are significant differences in fixation stiffness, complexity of surgical steps, and the incidence of postoperative complications. Thus, many clinicians still have difficulty to choose a proper surgical method for symptomatic lumbar spondylolysis.
The authors have performed a direct pars repair surgery using two different surgical methods; pedicle screw with universal hook system (PSUH) and direct pars screw fixation (DPSF). The authors performed a retrospective study to assess the clinical and radiological outcomes of the patients who underwent either surgical method, and compare the results between two different treated groups.
MATERIALS AND METHODS
The indications of the surgery for symptomatic lumbar spondylolysis were as follows; patients presenting with chronic low back or leg pain which was intractable with failed long-term conservative treatment; the imaging study showing pars defect on lumbar spine without significant instability; no definite neural compression on magnetic resonance image or myelogram; positive pars injection test; negative provocative discography. Pars injection test was performed under the fluoroscopic guidance. The needle was placed directly into the pars defect and 1 cc volume of local anesthetics (lidocaine) mixed with corticosteroid (triamcinolone) was injected. Positive pars injection test was defined as immediate pain improvement after injection, lasting for minimum 12 hours.
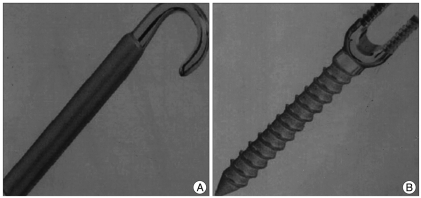
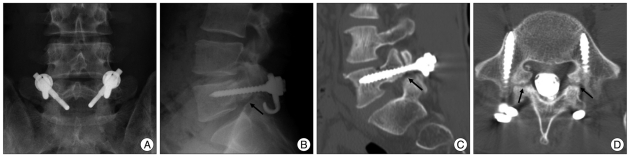
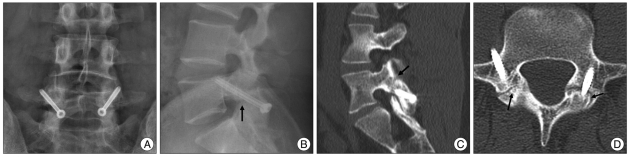
Between April 2001 and March 2008, 47 consecutive patients with symptomatic lumbar spondylolysis underwent direct pars repair surgery by a single surgeon. PSUH was used during first half of the study period and DPSF during the second half. The surgery was done in following steps. Under general anesthesia, the patient placed in prone position. After midline vertical skin incision and paravertebral muscle dissection, pathologic level of the spine was exposed. Following removal of the granulation tissue in pars defect, the sclerotic bone exposed on either side of the defect and was carefully roughened using Kerrison rounger or a micro-drill. The bone chips for auto-graft were taken from the adjacent lamina and put into the defect of pars with micro-impactor. In the cases of PSUH, a pedicle screw (AESCULAP® standard screw) (Fig. 1A) was placed at the pathologic spine, and then a lamina hook coupled with a rod (AESCULAP® universal hook) (Fig. 1B) was applied. While applying compression force, the part of rod was secured to the pedicle screw with a fixing nut (Fig. 4A). The same procedure was done on the opposite side. In the cases of DPSF, a path across the defect was drilled under the direct visualization. Then, the cortical screw was placed into the base of the articular process under the bi-planar fluoroscopic guidance. The same procedure was repeated on opposite the side.
The clinical outcome was measured using visual analogue pain scale (VAS) and Oswestry disability index (ODI). The length of operation time, the amount of blood loss, the duration of hospital stay, and surgical complications were assessed. The dynamic lateral plain radiographs and high-resolution computed tomography (CT) scans (LightSpeed VCT scanner, GE Healthcare) were obtained at final follow-up visits to evaluate fusion status. Radiologic fusion was defined as follows; no radiolucent gap in pars on plain X-ray; no difference between flexion and extension lateral films; and definite bony bridge at pars defect on postoperative CT scan. Statistical analysis was performed using SPSS (SPSS, Version 10, SPSS, Chicago, IL, USA). A p-value <0.05 was considered statistically significant.
RESULTS
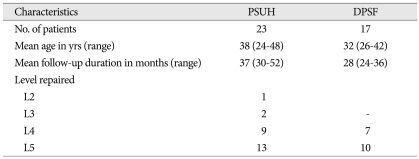
There were 23 cases in the PSUH group, and 15 in the DPSF group. Most of patients were male in each group. Mean age was 32.4 years. Most common operated level in each group was L5. The demographic data of the patients in each group is listed on Table 1.
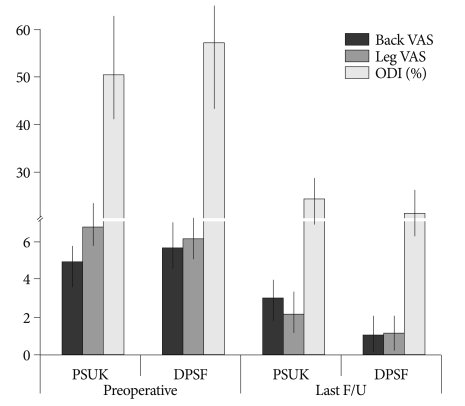
At the end of follow-up, the average back and leg VAS scores were significantly lower than the preoperative values, 4.7±1.3 versus 2.2±0.9 (p<0.05) and 6.8±3.5 versus 2.6±1.2 (p<0.05), respectively. The average ODI score was also reduced from 52.8±18.6% to 20.6±15.2%. However, the clinical outcomes of each group were dissimilar. In the PSUH group, the preoperative average back and leg VAS scores were reduced from 4.9±1.4 and 6.8±3.5 to 3.0±0.9 and 2.2±0.9 respectively at the last follow-up (p<0.05). And the preoperative average ODI score decreased from 50.6±16.6% to 24.6±13.4% at the last follow-up. In the DPSF group, the preoperative average back and leg VAS scores were reduced from 5.7±1.2 and 6.1±2.4 to 1.1±1.2 and 1.2±1.0 at the last follow-up (p<0.05). And the preoperative average ODI score decreased from 57.4±18.8% to 18.2±12.6% at the last follow-up (p<0.05). Although PSUH group showed statistically significant clinical improvement at the last follow-up, the degree of improvement was less than the DPSF group (p<0.05) (Fig. 2).
The operation time in the PSUH group ranged from 157 to 220 minutes, with an average of 174.9 minutes. In the DPSF group, the operation time ranged from 135 to 175 minutes, with an average of 141.7 minutes. The operation time of the PSUH group was significantly longer than that of the DPSF group (p<0.05). Blood loss during operation was 300 to 700 cc in the PSUH group, averaging 468.8 cc. In the DPSF group, blood loss was 200 to 400 cc, averaging 298.8 cc. Blood loss of the DPSF group was significantly less than that of the PSUH group (p<0.05). The average hospital stay after operation was 8.9 days in the PSUH group, ranging from 5 to 12 days, and 7 days in the DPSF group, ranging from 5 to 7 days. The PSUH group needed longer hospital stay after operation than the DPSF group (p<0.05).
In the PSUH group, there was one case of screw misplacement which caused radicular leg pain after operation, and repositioning of the screw was performed by revision surgery. One patient, who underwent direct repair of L5 pars defect showed spinal stenosis at L4-5 level after 4 years postoperatively and was treated with the simple decompression. One case presented with lumbar disc herniation at L4-5 level which required surgical treatment 2 years postoperatively, after the direct repair of L4 pars defect. In the DPSF group, one patient suffered from transient mild leg pain which disappeared after 5th postoperative day. Except this case, there was no case which showed new symptom or instrument failure during follow-up period.
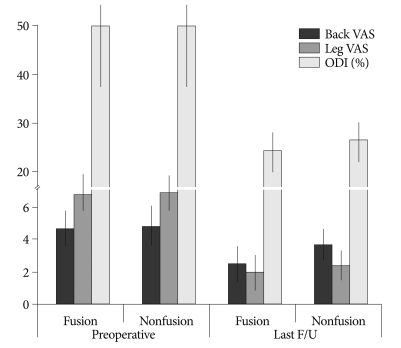
At the final follow-up, the successful bone fusion was achieved in 18 cases of the PSUH group with 78.3% of success rate, and 14 cases of the DPSF group with 93.3% success rate. The DPSF group demonstrated superior fusion success rate than the PSUH group (p<0.05). To compare clinical outcomes related to fusion, the PSUH group was divided into two groups; fusion group and nonfusion group. Nonfusion group showed less clinical improvement compared to fusion group (Fig. 3).
DISCUSSION
A clinical meaning of direct pars repair of symptomatic lumbar spondylolysis is the elimination of pain origin and the reconstruction of disease segment while preserving segmental motion. The first try of direct pars repair, proposed by Kimura, included just onlay graft with bone chip on defect of pars19,20). It required a longtime bed rest for 2 months postoperatively until bone fusion. Since then, various kinds of direct pars repair surgery have been introduced. Among them, Scott wiring technique which uses a wire to compress the defect, is technically demanding and has a potential of wire loosening or breakage, thus it has been restrictively used26). The technique using a hook screw specialized for pars repair (Morscher's technique)24), would be relatively simple, however early reports had shown a high incidence rate of pseudoarthrosis (up to 35%)14,28).
Fan et al.10), recently compared the biomechanical stiffness of different direct pars repair methods; pedicle screw with lamina hook system (TSRH's Hook plus screw fixation), direct pars screw, and Scott wiring technique by cadaveric test. In their results, the pedicle screw with lamina hook and direct pars screw groups showed the similar degree of stiffness as intact levels in flexion, extension, and rotation movement. However, Scott wiring technique showed less degree of stiffness than other techniques. Similarly, several reports also proved that both pedicle screw with lamina hook and direct pars screw techniques could provide enough stiffness in pars direct repair, however, the wiring technique could not23,35,37). Accordingly, the prior two techniques have been popular in the modern era.
In the present study, the authors compared clinical and radiological outcomes of these two techniques; pedicle screw with lamina hook system (PSUH) and direct pars screw (DPSF). The surgical technique of PSUH in the present study is similar with the technique suggested by Kakiuchi16). He introduced the pars repair technique by bridging with a rod anchored by a cephalad pedicle screw and a caudad laminar hook. The rod is secured to the pedicle screw and the laminar hook with applying compression force. A direct pars screw fixation as proposed by Buck3,4), is the simplest procedure among the pars repairing techniques being used in these days.
In the present results, the PSUH group showed longer operation time, more blood loss, and longer hospital stay than the DPSF group. Regarding the authors' experiences, assembling the pedicle screw, rod and lamina hook into a complete set and fixation with applying compression force was not easy, even though the system used in the present series consisted with only two parts; a pedicle screw and universal hook coupled with rod. It required substantial hard effort to apply compression in most of the cases while spending more time and more soft tissue manipulation, thus it might be the reason for longer operation time, more bleeding and a longer postoperative care. Moreover, although a specialized device was used to apply a forceful compression force, frequently either side of defect was not approximated enough and there was still a large gap in the pars even after full compression (Fig. 4B). This improper approximation of the defect could not afford the enough compression force to enhance the fusion rate (Fig. 4C, D).
On the other hand, the DPSF is an easy procedure requiring simple surgical steps. If the access hole and path was successfully drilled under the fluoroscopic guidance, the remaining steps can be carried out without any difficulty. This simplicity could reduce an operation time and soft tissue damage. Insertion of a lag screw with a forceful pneumatic driver as a final step makes a strong approximation of either side of the defect, and it could enhance bone fusion rate. Accordingly, the fusion success rate of the DPSF group was significantly higher than that of the PSUH group.
The reports arguing about using pedicle screw with lamina hook system have indicated that this method could provide a large area for fusion, thus fusion rate would be high6,8,26,30). Recent retrospective study for 11 patients who underwent pedicle screw with lamina hook system (TSRH's Hook plus screw fixation) for lumbar spondylolysis, reported 90.9% of fusion success rate with significant clinical improvement during 36 months follow-up9). However, the present study showed a contrary result. The PSUH group showed lower fusion success rate than the DPSF group, 78.3% versus 93.3%. Even though a surface area for fusion would be larger, the less compression force could negatively influence on the fusion success. Also, the fusion failure would affect the clinical outcome, and the PSUH group showed less degree of improvement than the DPSF group at the last follow-up.
All operations in the present series had been performed by single surgeon. Regardless of pars repairing methods, the preparation procedures before the instrumentation were clearly the same. Therefore, the authors believe the difference of the results between two groups could suggest the superiority of direct pars screw in the surgical treatment of symptomatic lumbar spondylolysis, compared to pedicle screw with lamina hook system.
In the DPSF, there has been a concern of difficulty in making a hole and a path for the direct screw fixation, especially in the cases having a thin lamina. The authors had used a 2.7-mm diameter lag screw in all patients, and there were no difficulties to place the screw, and no case of screw failure was noted. However, this technique is definitely a demanding procedure depending on the lamina narrowness. If the thickness of lamina was narrower than the screw diameter, it would be difficult to place a screw. And, there is a possibility to injure the existing nerve root by a misplaced or a longer screw. The risk of screw misplacement could be minimized by using bi-planar fluoroscopy. By carefully observing AP and lateral fluoroscopic views simultaneously during the drilling to make a path, a proper placement of the screw can be obtained. A screw length should be as long as the distance between the lower end of lamina and just above the base of the articular process. If the screw length was longer, existing nerve root could be injured. Thus, careful measurement of screw length after making a path is mandatory.
The adjacent segment diseases following spinal arthrodesis has been considered as major issue12,17,21,27). Although the veritable clinical efficacy is still not proven, a biomechanical study suggests that the motion preservation of the treated segment by direct pars repair do not affect adjacent segments motion. Mihara et al.23), analyzed the biomechanical effect of lumbar spondylolysis using calf lumbar spine in four different conditions as follows : 1) intact spine; 2) bilateral pars defects spine; 3) pars defect repair with direct pars screws; and 4) pedicle screw-rod fixation. According to their results, the pedicle screw-rod fixation limited the motion of instrumented segment, and significantly increased the intervertebral motion at the upper adjacent level. However, the direct pars screws restored the stability to the level of the intact spine without increase upper segment motion. In terms of clinical study, unfortunately, there has been no valuable comparative study between the direct pars repair and spinal arthrodesis to determine which method is more effective in the surgical treatment of symptomatic spondylolysis. Schlenzka et al.31), reported long-term (14.8 years) retrospective comparative study between the direct pars repair and segmental fusion, regarding clinical outcome, re-operation rate, radiological outcome, and complication rate. In the results, they stated that there was no significant difference in all outcome scores between two groups, and suggested the benefits of direct repair was questionable. However, their study only dealt with Scott wiring technique. Scott wiring has been known to have a lot disadvantages such as less stiffness, many intraoperative complications, and wire breakage after operation. Moreover, its usage is getting decrease nowadays. Thus, the actual benefit of direct pars repair using direct pars screw or pedicle screw and lamina hook is not proven yet, thus, it should be verified by well-designed comparative study.
The limitation of the present study is its retrospective and nonrandomized nature, as well as small number of cases, the lack of a control group and non-matched group size. However, most of symptomatic lumbar spondylolysis is successfully treated with conservative manner34), and spondylolysis advancing to spondylolithesis and combining with foraminal stenosis has to be surgically treated with interbody fusion20,33). Thus, the cases of symptomatic lumbar spondylolysis which required the direct pars repair surgery would be rare, and it is difficult to obtain enough data for prospective large series study in a single institute. Nevertheless, this study revealed that the pars repair with direct pars screw was more effective than the method using pedicle screw with lamina hook system in the surgical treatment of symptomatic lumbar spondylolysis.
CONCLUSION
The present study suggests that direct pars repair surgery would be useful to improve clinical symptoms of symptomatic lumbar spondylolysis without significant morbidity. However, the technique using direct pars screw would be more effective than the method using pedicle screw with lamina hook system, in terms of operation time, amount of blood loss, hospital stay, and fusion success rate, as well as clinical outcome. A well-controlled and further long-term follow-up clinical study is warranted.
 XML Download
XML Download