

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Leptomeningeal dissemination of tumor cells is frequently observed in terminal stage of malignant brain tumors, regardless of the primary origin. Occasionally, benign brain tumors, such as low-grade gliomas, spread to the subarachnoid space14). Recently, report of leptomeningeal dissemination of low-grade glioma is increasing as reflecting the common use of diagnostic magnetic resonance imaging (MRI)15). It is known that approximately 5% of low-grade gliomas present with leptomeningeal dissemination at the time of diagnosis, and 7-10% of low-grade gliomas present with leptomeningeal dissemination at the time of disease progression15). One study reported the frequency of leptomeningeal dissemination via histology : pilocytic astrocytoma 3%, low-grade fibrillary astrocytoma 2%, gangliolioma 4%, mixed glioma 5%10). The frequency categorized by primary tumor site was as follows : cerebellum and brainstem 3%, cerebral cortex 1%, diencephalic region 7%, and spinal cord 1%10).
Leptomeningeal infiltration of tumor cells with local recurrence is common. We report an uncommon case involving a low-grade brainstem glioma with spinal dissemination, but without local recurrence.
CASE REPORT
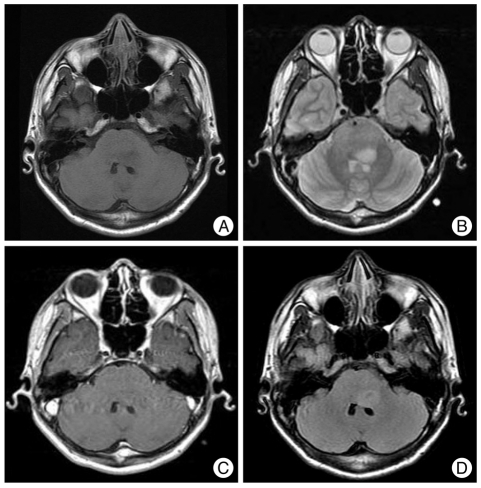
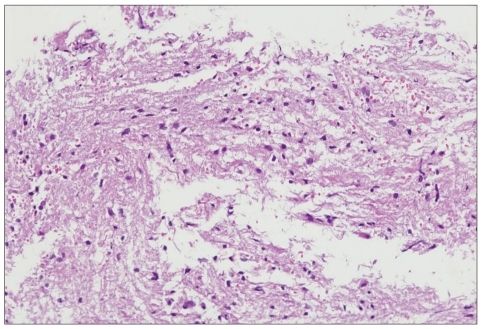
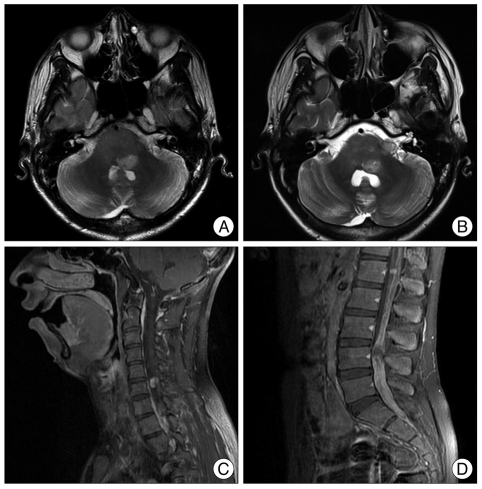
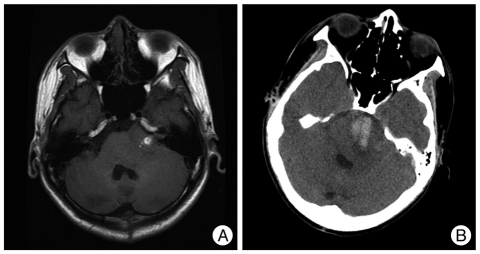
The patient was a 16-year-old boy who presented with diplopia, decreased vision, and gait disturbance of 2 months duration. On the neurologic examination, he had a limitation of the left lateral gaze and a facial palsy. Cerebellar function tests showed left-sided swaying on tandem gait. Brain MRI demonstrated about 2.0×2.4 cm pontine lesion with low-signal intensity on T1 weighted image (WI) and high-signal intensity on T2WI without gadolinium enhancement (Fig. 1). MR spectroscopy showed a slightly increased choline/creatinine ratio (1.07) and lactate peak, suggestive of a tumoral component and considered to be a pontine glioma. A biopsy was performed via an intrafacial triangle approach using the safe entry zone of the brainstem11). The histologic features were conspicuous cytoplasmic processes, mild nuclear pleomorphism, modest hyperchromasia, and no mitotic activity (Fig. 2). The immunohistochemical staining for glial fibrillary acidic protein was positive and the labeling index of Ki-67 was 5-7%. A fibrillary astrocytoma was diagnosed. Radiation therapy (total dose, 5400 cGy) was administered for the pontine lesion. The symptoms, especially the gait disturbance, were slightly improved after treatment; however, he still had a facial palsy and a limitation of lateral gaze. On the follow-up 4 months after diagnosis, decreased tumor size was noted (Fig. 3A). Seven months after diagnosis, the gait disturbance was worsened and new-onset lower back pain developed. The brain MRI showed a new lesion at the left cerebellopontine angle without an interval change in the primary lesion compared to the former images (Fig. 3B). A spinal MRI demonstrated leptomeningeal dissemination of the entire spine, primarily in the lumbosacral area (Fig. 3C, D). Radiation therapy was started in the spinal seeding area (total dose, 3750 cGy). Subsequently, chemotherapy with a carboplatin plus vincristine regimen was administered. However, his general condition worsened with drowsy mentality. A brain MRI showed an enlarged lesion associated with hemorrhage at the left cerebellopontine angle (Fig. 4A). Two month later the patient was in a stuporous state and brain CT had a hemorrhagic lesion involving the left cerebellopontine angle and pre-pontine space which had increased in size (Fig. 4B). The disease progressed and he died 13 months after the diagnosis.
DISCUSSION
Low-grade gliomas of the brain are common primary brain tumors, accounting for approximately 15-35% in most reported studies and characterized by slow progression and a median survival between 5 and 10 years2,6). Despite the long-term survival, most patients eventually die as a result of the progression into malignant gliomas. Leptomeningeal dissemination is another factor associated with poor prognosis.
Dissemination of tumor cells is the usual course of disease in primary central nervous system neoplasms; indeed, all types of brain tumors could undergo dissemination. This characteristic can be observed at the time of presentation or at the time of disease progression, primarily in medulloblastomas, germ-cell tumors, and high-grade gliomas8). Most reports have described neuraxis dissemination concurrent with or following recurrence at the primary site8,10). Civitello et al.3) reported that leptomeningeal dissemination was present in 6 of 162 children (3.7%) with low-grade gliomas : at diagnosis of the original tumor in one patient and with or following local relapse in four patients. One patient showed the leptomeningeal dissemination as a relapse sign but there was no examination for local recurrence. Spinal spread of primary intracranial tumors is more common in malignant brain tumors and some autopsy series have reported that such spreading occurs in 20-36% of supratentorial tumors and up to 60% of infratentorial tumors15,17). The incidence of tumor dissemination at the time of autopsy is probably higher than the clinical incidence of symptomatic metastasis. In low-grade gliomas, leptomeningeal dissemination is relatively rare. However, according to some reported studies, it has been estimated that 5% of low-grade gliomas are disseminated at the time of diagnosis, and 7-10% are detected along with the progressive course of the disease15). The increased use of MRI studies might in turn increase the detection of disseminated disease.
Controversy exists regarding the risk factors for low-grade glioma dissemination. The underlying pathogenesis is unclear and there is no histologic evidence by which to differentiate disseminated disease from localized disease; however, some risk factors have been reported, such as invasion of the ependyma and fragmentation of tumor in contact with the CSF5). The proximity of the tumor to the ventricular system and intra-operative ventricular entry may increase the risk of CSF dissemination9). Depending on the location, tumor arising from the diencephalon appears to predispose to leptomeningeal dissemination10). On the contrary, one study suggested that intra-operative ventricular entry, primary tumor proximal to the ventricular system, and surgical resection could not increase the risk of tumor dissemination4).
Some studies have demonstrated the mechanism of leptomeningeal dissemination8,16). Dissemination of tumor cells via the CSF is probably the primary mechanism for metastases within the central nervous system. Spread via the ventricular CSF might be the most likely mechanism of tumor dissemination in hypothalamic tumors. Bell et al.1) proposed that leptomeningeal dissemination can occur after surgical manipulation. The patient presented herein underwent a biopsy via the telovelar approach. The floor of the fourth ventricle was exposed via dissection of the tela choroidea and inferior medullary velum along the natural avascular plane on the left side. A biopsy was performed directly through the floor of the fourth ventricle. Seven months later, disseminated disease was detected in the cerebral subarachnoid space at the cerebellopontine angle and spinal cord, but not in the ventricular system. This pattern suggests direct shedding of tumor from the lateral foramen of the fourth ventricle through the operative tract into the subarachnoid space and transport via the CSF to distant sites within the neuraxis.
Patients with low-grade astrocytoma with neuraxis dissemination at the time of diagnosis have been reported to be a median survival of 15 months8). The course of disease varies from rapid progression, despite chemotherapy and radiation therapy, to prolonged stabilization. Radiation therapy can give long-term disease stabilization in some cases. Treatment with carboplatin, alone or combined with vincristine, has been reported to achieve durable disease stabilization in patients with primary or recurrent low-grade gliomas, even in young children who were asymptomatic with widespread neuraxis disease7,12,13). The overall prognosis for patients with leptomeningeal dissemination at the time of recurrence appears to be worse than the prognosis for patients with a localized recurrence, and far better than for patients with a malignant brain tumor with dissemination3,10). However, the patient described herein had progressive features, even after radiation therapy and subsequent chemotherapy with carboplatin plus vincristitine. Furthermore, tumoral hemorrhage caused mental status changes and he died after 13 months.
 XML Download
XML Download