

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
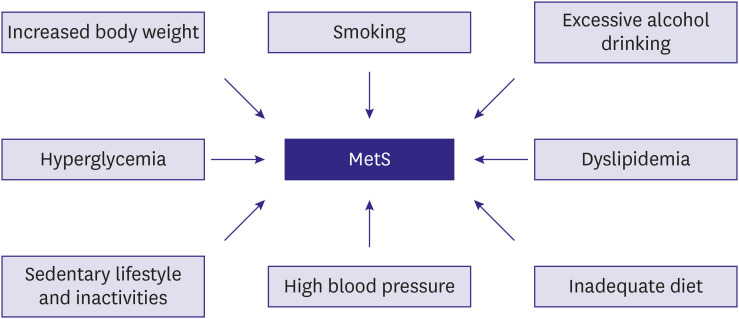
Metabolic syndrome (MetS) is a clinical condition characterized by a clustering of obesity-associated cardiovascular risk factors including abdominal obesity, hypertriglyceridemia, decreased high-density lipoprotein (HDL) cholesterol, high blood pressure, and/or impaired glucose tolerance (Table 1 and Figure 1).1)2)3)4) Recognizing and understanding MetS is clinically important because of its high prevalence and potential harmful effects on the cardiovascular system. As the prevalence of obesity gradually increases, the number of patients with MetS is increasing worldwide.5)6) National Health and Nutrition Examination Survey (NHANES) data showed that the overall prevalence of MetS in the United States increased from 32.5% in 2011–2012 to 36.9% in 2015–2016.7) According to the data analyzing the Korean National Health and Nutrition Examination Survey (KNHANES), the overall age-standardized prevalence of MetS slightly increased from 21.6% in 2007 to 22.9% in 2018 in South Korea.8) In subjects in their 60s, the prevalence of MetS gradually decreased from 47.5% in 2007 to 41% in 2018, but in men in their 30s (from 19% to 24.7%) and 40s (from 25.2% to 36.9%), the prevalence of MetS has increased rapidly over the past 12 years.8) As each component of MetS is a risk factor for cardiovascular disease, it is obvious that the combination of these risk factors substantially augments cardiovascular risk.9) Many clinical studies have shown that MetS is associated with the risk of developing diabetes mellitus, cardiovascular disease and mortality.10)11)12)13)14)15)16)17)18)19) Therefore, efforts should always be made to prevent the occurrence of cardiovascular complications related to MetS. Lifestyle modification is the most important and effective strategy to manage the MetS, improving cardiovascular prognosis. In this review, we address specific lifestyle modification for each risk factor in the management of MetS.
Table 1
Diagnostic criteria of metabolic syndrome suggested by Korean Society of CardioMetabolic Syndrome
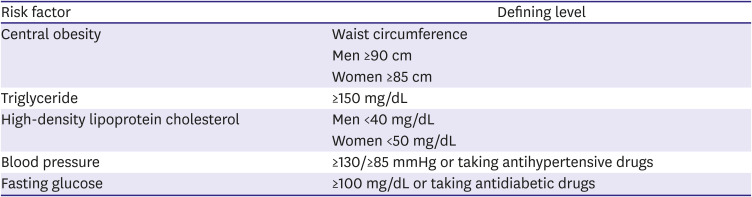
Metabolic syndrome is defined as having 3 or more of the 5 five risk factors shown in Table 1.
WEIGHT CONTROL
Abdominal obesity is associated with systemic inflammation, insulin resistance, and increased cardiovascular risk;20) it is the main diagnostic criterion for MetS. According to the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III), abdominal obesity was defined as a waist circumference ≥102 cm in men and ≥88 cm in women.2) In Korea, waist circumference ≥90 cm in men and ≥85 cm in women are used as diagnostic criteria for MetS.3)
Increased body weight is associated with MetS prevalence and incidence. According to the NHANES III, MetS was present in 5% of subjects with normal weight, 22% of those who were overweight, and 60% of those who were obese.21) In the Framingham Heart Study cohort, the weight increase by 2.25 kg or more over 16 years was associated with a 21% to 45% increase in the risk of developing MetS.22) A large waist circumference alone predicts up to 46% of individuals who will develop MetS within 5 years.23) The prevalence of rapidly increasing obesity among adults will lead to higher rates of MetS in the near future.5)6) Therefore, the importance of preventing obesity and improving physical activity should be emphasized. The key management strategies for MetS are aggressive lifestyle modification and increased physical activity focused on weight reduction. A 15-year follow-up study showed that young adults who maintained stable body weight had minimal progression of risk factors and lower MetS incidence.24) On the other hand, individuals with increased body mass index during the follow-up period had a higher incidence of impaired glucose tolerance and diabetes mellitus than those with stable or decreased body mass index.24) A moderate decrease in weight induced by a very low calorie diet resulted in substantial reductions in systolic/diastolic blood pressure, glucose, triglycerides and total cholesterol at 4 weeks.25) Also, a greater weight loss, as achieved by lifestyle modification, was associated with a greater reduction in the prevalence of MetS.26) Because sustained weight loss can improve all elements of the MetS, it not only reduces the risk of developing MetS, but also the reverse of the metabolic complications related to the MetS.27) It has been suggested that the effect of weight loss on reducing the risk of developing MetS was more effective with lifestyle therapy than with diet pills.26) Therefore, it is more important to maintain an appropriate body weight through lifestyle modifications such as exercise and diet control rather than through taking weight-loss medications. A realistic goal for weight reduction is to reduce body weight by ~7% to 10% over a period of 6 to 12 months.28)
SMOKING CESSATION
The smoking rate of men in Korea is the highest among major Organization for Economic Cooperation and Development (OECD) countries.29) Various toxic substances, such as nicotine, carbon monoxide and oxidizing gas from cigarette, cause abnormalities in lipoprotein metabolism, endothelial cell dysfunction and insulin resistance, which increase the risk of MetS.30)31)32)33)34) Nicotine stimulates the release of adrenaline, which increases blood pressure and heart rate.35) It has been suggested that nicotine induces lipolysis in adipose tissue, increases triglyceride, and low-density lipoprotein (LDL) cholesterol, and decrease HDL cholesterol in the blood.36) Insulin resistance by smoking alters the distribution of body fat and exacerbates central obesity.37) Smokers generally drink too much and do not exercise well, and thus these poor lifestyle habits further increase the risk of MetS. According to a meta-analysis of 56,691 people from 13 studies, smoking increased the risk of MetS by 1.26 times.34) The risk of MetS due to smoking increases in proportion to the amount of smoking.33) Smoking cessation reduces the risk of developing MetS, cardiovascular disease and mortality,31)38)39) so smoking cessation should be emphasized. However, for some time after quitting smoking, weight gain may occur, so lifestyle modification should be implemented more thoroughly after smoking cessation.40) Individuals are also required to avoid second-hand smoke or e-cigarettes as they also increase the risk of MetS and cardiovascular disease.41)42)43) Willingness and motivation of the patient to quit smoking are very important for successful smoking cessation. In particular, since strong and clear advice from doctors is known to increase the success rate of smoking cessation, doctors should motivate patients to stop smoking.44) Cognitive-behavioral therapy can be effective in stopping habitual thought and behavior associated with smoking and in accepting positive thought about smoking cessation.45)46) Specific methods of cognitive behavioral therapy include: 1) specifying and avoiding smoking-provoking situations (eating, coffee or alcohol drinking, etc.), 2) notifying people around when starting smoking cessation, 3) taking action to delay smoking (taking a deep breath, drinking water, brushing teeth, taking a walk, etc.), 4) using alternatives to smoking (such as chewing gum or vegetables). After quitting smoking, moderate-intensity aerobic exercise (jogging, cycling, dancing, swimming, mountaineering, etc.) lowers stress, suppresses the desire to smoke and reduces withdrawal symptoms; therefore, it is effective in maintaining smoking cessation.31)47)48) Since weight gain after smoking cessation usually occurs,31)49) it is important to maintain appropriate weight through regular exercise and healthy eating habits.31)47)48) Avoiding fatty, sweet and high-calorie foods as well as making a habit of eating vegetables and fruits every day is helpful in smoking cessation.31)50) The guidelines proposed by the American Heart Association recommend the following smoking cessation steps: 1) collection of information about smoking conditions, 2) assessment of withdrawal symptoms or attempts to quit smoking, 3) recommendation of smoking cessation, 4) explanation on the specific methods of smoking cessation and selection of the method, and 5) thorough follow-up.45)
ALCOHOL DRINKING IN MODERATION
As of 2017, alcohol consumption per person in Korea was 8.7 liters, which is similar to the OCED average.29) Among risk factors related to MetS, light to moderate drinking has been demonstrated to reduce cardiovascular disease, diabetes and mortality.51)52) However, blood pressure rises and blood triglyceride level increases in proportion to the amount of alcohol consumption.53) Therefore, guidelines for drinking behavior are needed. The amount of alcohol consumption per person is steadily increasing in Korea.54) Especially, the rate of binge drinking is high, and the proportion of women drinking is showing a steady increase.55) A J-shaped association between the amount of alcohol drinking and MetS risk has been reported: compared with nondrinking, light or moderate drinking was associated with decreased risk of MetS, while heavy drinking was associated with increased risk of MetS.56)57)58) In addition, blood pressure and alcohol intake are generally known to have a linear relationship between them, but it is reported that drinking less than 3 glasses a day lowers blood pressure.59) Lipid profile and alcohol intake are also non-linear and have a relationship between U- and J-types.60)61) Moderate drinking is known to improve insulin sensitivity, and reduce the risk of diabetes.62) On the other hand, a large amount of alcohol does not affect the development of diabetes, so diabetes also has a J-type association with alcohol consumption.62) According to a study that analyzed 7,962 subjects using data from the KNHNES, drinking less than 15 g per day lowered the risk of MetS in men by 29% in men and by 20% in women.53) However, drinking 30 g or more per day increased the risk of high blood pressure (blood pressure >130/80 mmHg) and hypertriglyceridemia (triglyceride >150 mg/dL) by 20–30%.53) According to a recent meta-analysis, drinking less than 5 g per day reduced the risk of MetS by 14%, whereas drinking more than 35 g per day increased the risk of MetS by 1.8 times.57) Collectively, light to moderate alcohol consumption has a beneficial effect on MetS components as well as on MetS. The World Health Organization (WHO) recommends limiting alcohol consumption to less than 40 g per day for men and 20 g per day for women.63) Reflecting this in Korea, it is recommended to limit intake to less than 4 glasses of soju for men a day and 2 glasses of soju a day for women.
DIET CONTROL
The goal of MetS prevention and treatment is to reduce cardio-cerebrovascular disease and death. Among various prevention strategies, a proper diet plays a crucial role. The type and total amount of fat intake are important. There exists a good correlation between blood lipid concentration and the progression of arteriosclerosis. The consumption of saturated fat in Korea is gradually increasing due to the Westernization of lifestyle. The risk of cardiovascular disease decreases when saturated fatty acids are replaced with polyunsaturated fatty acids.64)65) Trans-fat is mainly found in breads, sweets, and processed foods such as milk and meat. Trans-fat increases total cholesterol and decreases HDL cholesterol. It is also known that eating more than 2% of total calories in trans-fat increases the risk of cardiovascular disease by 23%.65) Therefore, it is recommended to consume unsaturated fatty acids, and minimize trans-fat intake.65) Carbohydrate is converted to glucose in the body and used as an energy source, but after excessive consumption, it is converted to fat, which increases triglycerides and reduces HDL cholesterol.66)67) In particular, it was reported that Koreans consume more carbohydrate and have a stronger association with MetS than in do Westerners.68) Therefore, patients with MetS should reduce carbohydrate intake. Koreans consume 2- to 3-fold amount of salt recommended by the WHO. Excessive intake of sodium increases body fluid content along with blood pressure.69) A low sodium diet may lower blood pressure.70) Although vitamin intake is believed to slow vascular aging through its anti-oxidative effect, there have been few studies confirming the preventive effect of cardiovascular disease through vitamin intake.71) Dietary fibers are not digested and absorbed by the body; however, they can absorb various ingested substances thus can improve hyperlipidemia and prevent constipation.72) However, excessive fiber consumption can interfere with nutrient absorption. The Dietary Approaches to Stop Hypertension (DASH) diet is one developed by doctors and nutritionists to control the diet of hypertensive patients with the aim of eating various nutrients in a balanced manner. It consists of fresh vegetables, fruits, low-fat dairy products, brown rice, whole grains, fish, and lean chicken, which can significantly lower systolic blood pressure.73)
EXERCISE AND PHYSICAL ACTIVITY
Exercise is essential for weight loss along with diet control.74) In addition, exercise has the effect of lowering the risk of cardiovascular disease and increasing life expectancy.75)76) It is clear that there is an inverse correlation between the total amount of moderate-intensity exercise and the incidence or mortality of cardiovascular disease, and these effects become more apparent as the amount of exercise increases.77) It is recommended that at least 150 minutes of moderate intensity exercise (fast walking, biking at least 8 kilometers per hour, active yoga, light swimming, etc.) or more than 75 minutes of high intensity exercise (jogging, running, cycling at least 15 kilometers per hour, tennis, intensive swimming, etc.) every week for the prevention of cardiovascular disease.77) There is also a negative dose-response relationship between physical activity and the prevalence of MetS.78)79) Exercise and increased physical activity not only decrease waist circumference, blood pressure, and body fat mass, but also improve insulin resistance and lipid profiles.75)80) For the primary prevention of obesity, about 150–250 minutes of moderate intensity exercise per week, along with an energy equivalent of 1,200 to 2,000 kcal per week, can help prevent weight gain.81) The recommended amounts of physical activity to promote clinically significant weight loss and to prevent weight gain after successful weight loss is 225–420 minutes and 200–300 minutes per week, respectively.82) Both aerobic and strength exercise are important. Aerobic exercise clearly reduces the risk of cardiovascular disease,75) and resistance exercise not only improves physical function, but also reduces blood glucose and blood pressure. Although resistance exercise alone contributes to body fat loss, the effect on overall weight loss is minimal.83) It has been suggested that combined aerobic and resistance exercise is more effective in controlling blood glucose than aerobic or resistance alone.84) Since exercise alone is less effective in losing weight, it is necessary to combine with an appropriate calorie restriction diet.85) Regular exercise also plays a crucial role in maintaining weight after weight loss.86) The sedentary lifestyle is prevalent in modern society. Energy consumption in this lifestyle is only 1.5 times higher than that during rest (energy consumption during exercise is 10 to 20 times higher than during rest). It has been demonstrated in many studies that this sedentary lifestyle is a major cause of MetS, cardiovascular disease or diabetes. Therefore, it is very important to increase the amount of physical activity and reduce the amount of time sitting in everyday life.75)
COGNITIVE BEHAVIORAL THERAPY
The behavior pattern that lasts over a long period of time since childhood is likely to persist even into adulthood. These environmental factors interact with genetic factors to form a lifestyle. In addition, exposure to wrong medical common sense through the advice of non-medical professionals can lead to an improper lifestyle. Therefore, the role of primary healthcare providers who can continuously manage patients is more emphasized in cognitive behavioral therapy to prevent MetS. Medical professionals should build positive relationships with patients consistent in their attitude to behaviors. When patients’ medical condition, life environment, knowledge level, experience and interests over a long period of time are widely understood, motivation for appropriate counseling and desirable behaviors tailored to each patient can be successfully achieved and sustained.87)88) It has been suggested that motivational interviewing with doctors is very effective in inducing smoking cessation.44) In addition, if decision-making is shared not only with the patient but also with the neighboring family, this can lead to more continuous and consistent changes.89) Since it is not easy to correct a wrong lifestyle that the patient has maintained for a long time, clinicians should ask whether they are able to follow the decision-making.89) Moreover, if positive changes are seen, clinicians encourage them to maintain and reinforce those behavioral changes. However, since it is necessary to maintain the lifestyle and behaviors that the patient judges to be correct, it is most important to help control and monitor them by themselves.90) Through these positive interactions, the patient must eventually set long-term goals for himself, and based on confidence through changed behaviors, he/she must be able to set new improved goals.
BLOOD PRESSURE CONTROL
Hypertension is one of the most important diseases that threaten global human health.91) According to the factsheet of hypertension published by the Korean Society of Hypertension in 2020, the prevalence of hypertension among Koreans aged >20 years is up to 29%, and 61.6% of hypertensive patients have diabetes or dyslipidemia as well.92) According to Korean data, among the components of MetS, hypertension is the most important factor, which is observed in 39.9% of men with MetS, and in 25.4% of women with MetS followed by low HDL cholesterol.8) To prevent the occurrence of atherosclerotic cardiovascular disease in patients with MetS, management of high blood pressure is essential. The priority treatment for blood pressure control is lifestyle modifications including salt restriction, diet, weight loss, exercise, smoking cessation, and reducing alcohol consumption.93)94)95)96) The salt intake of Koreans is higher than the recommended amount of the WHO. Reducing salt intake to less than 5 g/day is effective in lowering blood pressure.94) According to a recent meta-analysis, reducing salt intake by 4.4 g per day had an average blood pressure lowering effect of 5.4/2.8 mmHg in hypertensive patients.97) The DASH diet is recommended for blood pressure control. It can reduce salt intake, and promotes the consumption of vegetables, fruits, lean meats, whole grains such as whole wheat, brown rice and the inclusion of micronutrients in the menu.94)95)96) The DASH diet has been proven to have a substantial blood pressure-lowering effects.93) It was reported that the group that maintained the DASH diet showed a blood pressure lowering effect of 11.4/5.5 mmHg during the 8-week observation period.93) Overweight is also an important causative factor of hypertension, and it is known that a loss of 1 kg in body weight has a blood pressure-lowering effect of about 1 mmHg.98) Since Koreans have a higher incidence of abdominal obesity than Westerners, it is recommended to keep waist circumference below 90 cm for men and 85 cm for women along with low body mass index.3) Exercise lowers blood pressure as well as reduces body weight and blood sugar/cholesterol, thereby decreasing the occurrence of cardiovascular diseases and death.76)80)82) A meta-analysis has demonstrated that an average weight loss of 5.1 kg has a blood pressure-lowering effect of about 4.4/3.6 mmHg, which can be explained by a 1 mmHg drop in blood pressure when 1 kg of body weight is lost.98) The Korean Society of Hypertension recommends performing aerobic exercise 5 to 7 times a week, 30 minutes or more at a time to lower blood pressure, and the aerobic exercise includes breaking walk, jogging, cycling, swimming, jumping rope, and aerobic gymnastics.94) Smoking raises blood pressure through sympathetic hyperactivity, so it is recommended to quit smoking.99) Excessive drinking is associated with an increase in blood pressure or cardiovascular disease, so it is recommended to reduce alcohol consumption to less than 40 g per day for men and 20 g per day for women.63)
DYSLIPIDEMIA CONTROL
To achieve satisfactory therapeutic outcomes in patients with dyslipidemia, non-pharmacologic interventions, such as diet, exercise, limited consumption of alcohol, and smoking cessation, should be the first-line therapy.100)101)102) The Korean dietary pattern is typically a high-carbohydrate and low-fat diet. High-carbohydrate diet intake is associated with increased risk of hypertriglyceridemia and hypo-HDL cholesterolemia.66)67) Therefore, total carbohydrate intake should not exceed 65% of total energy, and sugar intake should be reduced below 10–20%.102) It is recommended to consume energy at a level to maintain appropriate weight and to reduce total fat intake below 30% of total energy.102) Saturated fatty acid is a dietary factor that has the most significant effect on serum LDL cholesterol levels. A 1% increase in the proportion of saturated fatty acids in total energy intake has been reported to increase LDL cholesterol levels by 0.8–1.6 mg/dL.103) Thus, it is recommended to keep saturated fatty acids <10% of total energy and should be further reduced (<7% of energy) in the presence of hypercholesterolemia.101) The evidence relevant for the intake of unsaturated fatty acids in dyslipidemia is not yet sufficient, but LDL cholesterol levels decrease when saturated fatty acids are replaced with monounsaturated fatty acids or omega-6 polyunsaturated fatty acids.102) Trans-fat intake is associated with increased LDL:HDL cholesterol ratio and cardiovascular risk.65) Hence, it is advisable to avoid trans-fat intake. A daily fiber intake of 25 g or more is recommended since dietary intake of fibers can reduce the risk of cardiovascular disease by decreasing blood glucose and LDL cholesterol levels.72)104) Alcohol consumption can increase serum triglycerides by reducing the activity of lipoproteinase, so alcohol is limited to 1–2 glass a day in hypertriglyceridemic patients.102)105)106) In patients with dyslipidemia, it is recommended to increase physical activity and perform moderate-intensity aerobic exercise regularly 4–6 times a week for at least 30 minutes.102)107) Resistance exercise is recommended to be performed at least twice a week.108) In general, it is known that the effect of exercise or weight loss to control dyslipidemia is not better than in hypertension or diabetes.101) Smoking causes abnormalities in reverse cholesterol transport and increases free fatty acids in the blood by promoting fatty acid breakdown,109) which results in increases in total and LDL cholesterol and triglyceride and decreases in HDL cholesterol.110) As a significant risk factor for cardiovascular disease, smoking cessation is strongly recommended in patients with dyslipidemia.102) Quitting smoking provides many benefits especially in terms of increasing HDL cholesterol and reducing cardiovascular risk.111)
BLOOD GLUCOSE CONTROL
Patients with MetS have 2-fold higher risk of developing cardiovascular disease and 5-fold higher risk of developing type 2 diabetes.10)11)12)13)14)15)16)17)18)19) Therefore, it is important to lead a healthy lifestyle with a balanced diet. According to the United States NHANES, there was a significant relationship between physical activity and insulin sensitivity,112) and the American Heart Association (AHA) recommends regular moderate-intensity exercise at least 5 times a week and 30 minutes or more at a time.113) Increased physical activity can prevent the development of diabetes,114)115) which is more effective in preventing diabetes than an oral hypoglycemic agent, metformin, that improve insulin sensitivity.116) Maintaining proper dietary habits is also crucial for preventing diabetes.114) Basically, it is important to reduce calorie intake, and lowering the proportion of carbohydrates among nutrients is effective in lowering plasma triglycerides, blood glucose, and visceral fat. A low-fat diet also has the effects of reducing calorie intake, which can lower blood pressure, blood cholesterol, inflammatory indices, and insulin sensitivity.117) High intakes of saturated and trans fatty acids increases the risk of insulin resistance and diabetes.118) Otherwise, consuming monounsaturated fatty acids or polyunsaturated omega-3 fatty acids helps improve abdominal obesity, insulin resistance and dyslipidemia.118) It is inconclusive how the daily level of protein intake affects blood glucose control117); however, ingestion of protein from fish rather than meat is more helpful in improving insulin resistance and inflammation. The Mediterranean diet is known to be effective not only in lowering blood glucose, but also in controlling hypertension, dyslipidemia, and inflammation.119)120) It consists of fruits, vegetables, nuts, legumes, whole grains, and fish with a larger amount of monounsaturated fatty acids or polyunsaturated omega-3 fatty acids.119) The Mediterranean diet has a similar weight loss benefit, but lowers the blood levels of glucose and C-reactive protein more significantly when compared to a low-fat diet.121) Legumes is effective in controlling blood glucose after a meal by reducing the absorption rate of carbohydrates.122) There is no evidence that routine supplementation with antioxidants (vitamin C, vitamin E, carotene, etc.), herbal supplements and micronutrients (cinnamon, curcumin, vitamin D, aloe vera, chromium, etc.) improve glycemic profiles.117)
Dairy products, eggs and fibers have favorable effects of lowering blood sugar, so it is recommended to consume their appropriate amounts for individuals with diabetes mellitus or high blood glucose levels.123)124)125) Moderate alcohol intake is known to have beneficial effects on glycemic control and insulin sensitivity, but excessive drinking causes hyperglycemia and weight gain.62)117) No more than 2 drinks per day for men and no more than 1 drink per day for women is recommended in patients with diabetes.117)
CONCLUSIONS
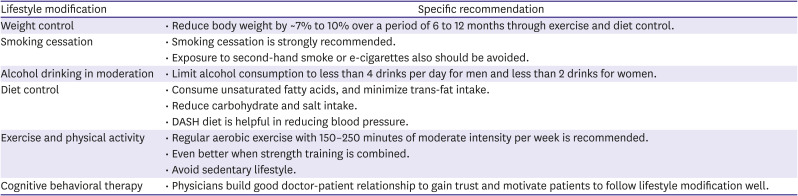
The most fundamental and effective way to manage MetS is lifestyle modification such as smoking cessation, regular exercise and proper eating habits. Key points of lifestyle modifications are shown in Table 2. A healthy lifestyle can prevent or delay the onset of MetS in susceptible subjects. In patients with MetS, lifestyle modification improves profiles of each component of MetS, and reduces the risk of developing diabetes and cardiovascular disease. Therefore, leading a healthy lifestyle should be emphasized for cardiometabolic health, regardless of MetS. In order to maximize benefits from lifestyle modification, it is important to change a lifestyle based on the results of many studies. We summarized practical methods for lifestyle modifications based on published data, which will help clinicians manage MetS.
Table 2
Summarization of lifestyle modification methods for MetS management
 XML Download
XML Download