

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Long QT syndrome is a cardiac repolarization disorder, and is associated with an increased risk of torsades de pointes (TdP), a life-threatening type of polymorphic ventricular tachycardia, and sudden cardiac death [1]. Acquired and congenital forms can be distinguished. Acquired long QT syndrome is most often attributable to administration of specific medications and/or electrolyte imbalance.
Polypharmacy is frequently encountered in patients suffering from chronic pain. The coexistence of pain and depression is common, as is co-treatment for these conditions [2]. The association of antidepressants and antipsychotic medications with prolongation of the QT interval is well known [3]. However, many clinicians are less aware of the possible arrhythmic potential of other types of medication used to treat pain. This review provides insights into the risk for QT prolongation associated with drugs frequently used in the treatment of chronic pain.
MAIN BODY
1. Acquired long QT syndrome
The QT interval is defined as the duration from the beginning of the QRS complex to the end of the T wave. It is a surrogate parameter of ventricular depolarization and repolarization in the surface electrocardiogram (ECG). Heart rate influences the QT duration, so it is common to present the rate-corrected QT interval (QTc). This is calculated from Bazett's formula:
Prolongation of the QT interval above 470 ms for men and 480 ms for women should be regarded as abnormal [4]. Several risk factors for QT prolongation have been identified, including female sex, advanced age, drug-drug interactions, genetic predisposition, hypokalemia, hypomagnesemia, heart failure, and bradycardia [56]. To reduce the risk of developing TdP, the American Heart Association/American College of Cardiology recommends ECG recordings before and 8–12 hours after an initiation or increase in doses of medication associated with an increased risk of QT prolongation [4]. In the pathomechanism of the acquired long QT syndrome, the human ether-a-go-go related gene (hERG), a voltage gated potassium channel, plays a pivotal role, as it is blocked by various medications [7].
2. Non-steroidal anti-inflammatory drugs
The use of non-steroidal anti-inflammatory drugs (NSAIDs), whether prescribed or self-administered, is extremely prevalent. A recent epidemiologic study reported that nearly one third of the general population had used NSAIDs within the previous 4 weeks [8]. The cardiovascular risks associated with NSAIDs are well known and commonly attributed to thrombotic events caused by the inhibitory effect of cyclooxygenases inhibition on platelets and the endothelium; however, alteration of cardiac repolarization is a completely different mechanism which also increases cardiac non-thrombotic risk [9].
Ketorolac has been confirmed to increase QT duration. In one study, a single dose of ketorolac increased the QT duration by > 30 msec. In patients undergoing general anesthesia, a single dose of ketorolac increased QT duration by 58% [10].
Pathak et al. [11] presented three patients developing TdP within days after initiation of celecoxib therapy. Two of them had a preexisting history of long QT syndrome. In an ex-vivo experiment, celecoxib inhibited hERG channels [12].
For diclofenac, an in-vitro study observed no prolongation of repolarization in therapeutic doses. However, in the case of reduced repolarization reserves, high doses of diclofenac may lengthen repolarization and enhance pro-arrhythmic risk [13].
3. Opioids
Methadone is well known to increase the QT duration in a dose-dependent manner [14]. A recent prospective analysis of initiation of methadone therapy (maximum daily dose = 60 mg) in patients with chronic pain has found that 11% had a QTc > 450 ms at any time point and that the highest incidence was observed after 1 month of treatment [15]. Similar incidences of long QT syndrome have been reported in other studies investigating pain patients on stabile methadone doses [16].
In its clinical practice guideline on the safety of methadone, the American Pain Society emphasizes the risk of QT prolongation when using this agent [17]. ECG changes consistent with blockade of sodium and potassium channels, including long QT, are described for tramadol [18]. A recent study in 115 patients showed a clear positive correlation between plasma tramadol concentration and QT duration [19].
Buprenorphine was traditionally considered to be a relatively safe drug in regards to developing long QT syndrome [2021]. However, recent reports indicate that buprenorphine increases the risk of a prolonged QT interval [2223]. Most of the evidence comes from patients undergoing substitution therapy at considerably higher doses than those used in patients being treated for pain. However, the clinical significance of the observed effects is still debated [22].
Oxycodone has a low affinity for the hERG channels. It has been shown to prolong the QT interval in a dose-dependent manner [24]. In a retrospective analysis of 137 patients treated for oxycodone overdoses, 17% had an increased QTc interval [25].
A recent study prospectively analyzed the risk of developing long QT syndrome in patients on newly initiated pethidine treatment and found that up to 25% showed a pathologic prolongation of cardiac repolarization. The QTc and changes from the pre-treatment baseline QTc showed a positive correlation with plasma levels of pethidine and an even stronger correlation with those of the metabolite normeperidine [26].
4. Anticonvulsants
Lamotrigine blocks hERG potassium channels to a significant extent in vitro, but topiramate and gabapentin have considerably less effect [27]. In healthy volunteers, therapeutic doses of lamotrigine were not associated with significant QT changes [28].
Gabapentin enacarbil, a prodrug of gabapentin, had no effect on cardiac repolarization in healthy volunteers [2930]. In rabbits, therapeutic doses of pregabalin significantly prolonged the QT interval [31]. The clinical relevance of these findings in humans is still unknown because there have been no published clinical reports on the association between most antiepileptic drugs and QT prolongation [3233].
5. Antidepressants
Antidepressants are frequently used in patients with chronic pain for two reasons. Firstly, pain and depression are common co-morbid conditions, and secondly, some antidepressants have analgesic properties, e.g. those used in the treatment of neuropathic pain.
Generally, the increase in QTc is significantly greater for tricyclic antidepressants than for selective serotonin reuptake inhibitors; of the latter agents, citalopram has been demonstrated to cause the greatest increase in QT-interval [34]. There have been many reports of long QT-intervals and TdP in patients receiving citalopram [35]. In 2012, the US Food and Drug Administration addressed this problem in a safety communication [36]. Escitalopram was associated with less QT prolongation. More recent research has not found a correlation between plasma escitalopram levels and QTc duration [37]. In contrast, for amitriptyline, a tricyclic antidepressant that is frequently used to treat patients with pain, this correlation is proven [38].
Among the serotonin-noradrenaline reuptake inhibitors, venlafaxine is associated with the highest risk of long QT syndrome [39]. Concerns about such an association appeared soon after venlafaxine was approved for the treatment of depression [40]. However, no correlation could be found between serum venlafaxine concentration and prolongation of the QTc interval.
6. Cannabinoids
There is increasing evidence that the cannabinoids can alleviate chronic pain [43]. In a study performed in healthy volunteers, an oral mucosal spray containing delta-9-tetrahydrocannabinol/cannabidiol had no significant effect on ECG parameters, either in recommended or in supra-therapeutic doses [44]. In vitro experiments for JWH-030, a new synthetic cannabinoid, demonstrated blocking of the hERG channel and therefore potential QT prolongation [45].
8. Antiemetics
Antiemetics are frequently used to treat the nausea and vomiting associated with use of opioid analgesics. It is known that all the first-generation 5-hydroxytryptamine3 (5-HT3) receptor antagonists have the potential to increase the QT interval [48]. In a prospective clinical trial, a single 4 mg intravenous dose of ondansetron prolonged the QTc interval by 19.3 ± 18 ms. In another study, administration of ondansetron resulted in long QT syndrome in 31% of patients with heart failure and 46% of those with acute coronary syndrome, respectively [49]. A systematic review of literature in 2013 identified 60 cases of cardiac arrhythmia after administration of ondansetron [50].
For dolasetron, the US Food and Drug Administration has since released a safety warning addressing the its association with an increased risk of ECG changes, particularly in patients with pre-existing heart disease [51]. For granisetron, evidence remains unequivocal [525354].
Haloperidol is an interesting agent in the treatment of pain, in that it has both antipsychotic and analgesic actions [5556]. Further, it has a well-known antiemetic effect, which is achieved in doses that are considerably lower than shore recommended for psychiatric indications [57]. In a recent study, haloperidol was non-inferior to ondansetron in treatment of postoperative nausea and vomiting; unfortunately, the risk of QT prolongation was comparable [58]. Similarly, other substances in the butyrophenone group, e.g., domperidone and droperidol, have also been shown to have an increased risk of long QT syndrome [5960].
9. Proton pump inhibitors
Proton pump inhibitors are among the most frequently prescribed drugs and are overused, especially in long-term therapy [63]. They are known to cause hypomagnesemia because of loss of magnesium via both the renal and gastrointestinal routes [6465]. This mechanism could potentially have contributed in the case-report of a patient who developed life-threatening TdP 7 hours after oral administration of pantoprazole 40 mg [66]. For esomeprazole, no effect on ECG parameters could be found in healthy volunteers 1.5 or 3 hours after a 40 mg dose [67].
In another case report, addition of lansoprazole in a patient already taking disopyramide, a class Ia antiarrhythmic agent, was associated with development of in long QT syndrome (QTc 690 ms) and TdP [68]. There has been an even more dramatic case report of pulseless ventricular tachycardia in a patient who received lansoprazole in addition to long-term therapy with voriconazole, an antifungal agent known to prolong repolarization [69].
10. Diuretics
Use of diuretic drugs is common, especially in elderly patients. These agents are also the most common cause for drug-induced electrolyte disorders [70]. These adverse effects are dose dependent [71]. Electrolyte disturbances may indirectly increase the risk of TdP [7273]. Further, furosemide has long been known to increase the QT interval [74].
CONCLUSIONS
Prolongation of cardiac repolarization is a severe complication caused by many substances. Increasing awareness and ongoing research have raised suspicion regarding several pharmacological agents. However, the clinical significance of single reports and in-vitro experiments is not always clear.
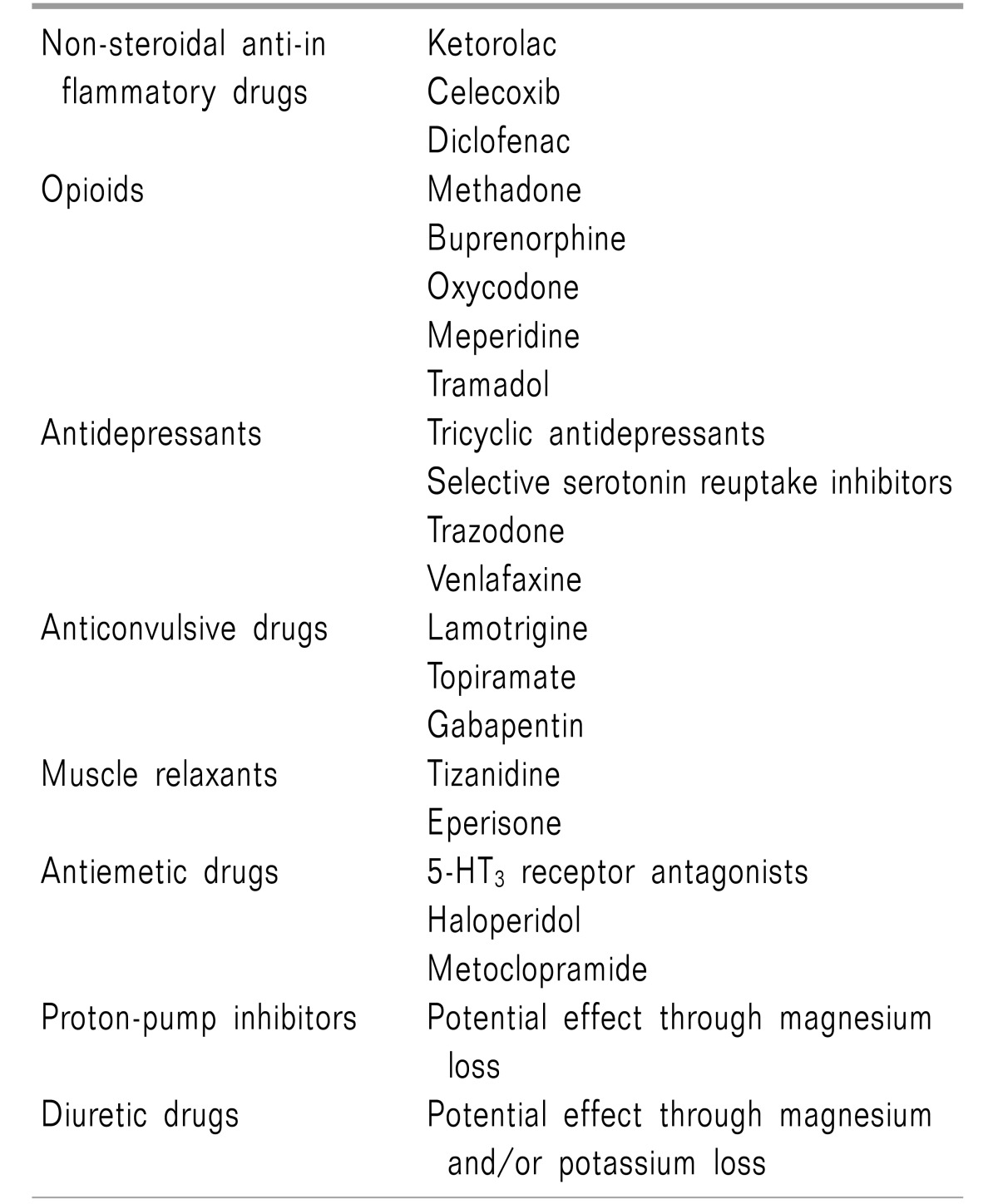
There are three pivotal strategies for reducing the risk of QT prolongation. First, awareness should be raised regarding possible circumstances or preexisting comorbidities that could increase the risk of QT prolongation. Being female, advanced age, hypokalemia, hypomagnesemia, a history of heart failure, and bradycardia are often mentioned in this context. Second, awareness should be increased regarding medications associated with an increased risk of ECG changes. In the field of pain medicine all the major drug classes contain agents that have an increased risk of QT prolongation. Other substances, not used in the treatment of pain, such as proton pump inhibitors, antiemetics, and diuretics are also associated with long QT syndrome (Table 1). Third, when risk factors are identified, alone, or even worse in combination, alternative treatment options should be considered. When the possible benefits of therapy outweigh the associated risks, slow dose titration and ECG monitoring are recommended.
 XML Download
XML Download