

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
The U.S. Food and Drug Administration (FDA)-approved pharmacologic options for osteoporosis include bisphosphonates (zoledronate, alendronate, ibandronate, and risedronate, in order of affinity for binding to the bone mineral matrix), calcitonin, estrogen agonist/antagonist (raloxifene), estrogens and/or hormone therapy, tissue-selective estrogen complex (conjugated estrogen/bazedoxifene), human parathyroid hormone 1-34 (teriparatide), and the receptor activator of nuclear factor kappa B ligand (RANKL) inhibitor (denosumab) [1].
Bisphosphonates (BPs) are currently the most widely used antiresorptive therapies [12]. They act by binding the mineral component of bone and interfere with the action of osteoclasts. The nitrogen-containing bisphosphonates, such as alendronate, act as inhibitors of farnesyl-pyrophosphate synthase, which leads to inhibition of the prenylation of many intracellular signaling proteins [3].
Denosumab (60 mg of Prolia® or 120 mf of Xgeva®, Amgen Inc., Thousand Oaks, CA) is a fully human monoclonal antibody (IgG2) that binds the RANKL and blocks the binding of the RANKL to the RANK. It finally inhibits the formation, function, and survival of osteoclasts, decreases bone resorption, and increases bone density, mass, and strength, similar to the endogenous effects of osteoprotegerin (OPG) [456].
This narrative review examines when this novel immune-related antiresorptive agent, denosumab, is indicated or may be substituted for current anti-osteoporotic drugs, based on its mechanism of action and adverse events compared with other drugs [7].
MAIN BODY
1. History for approved indications
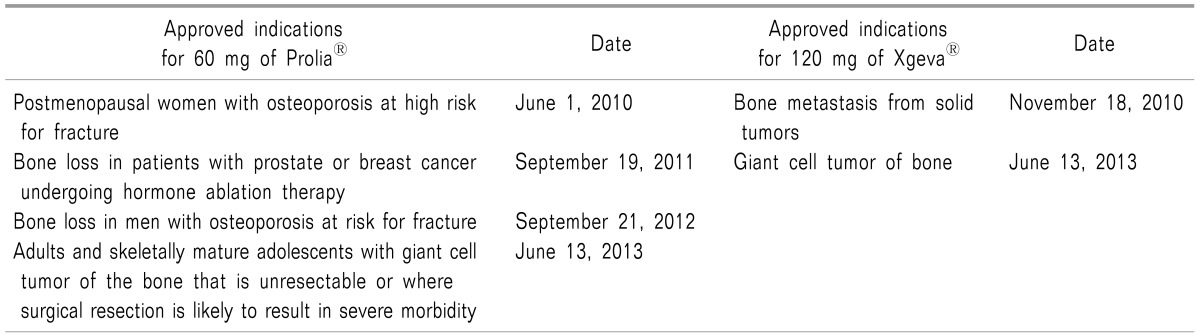
The U.S. Food and Drug Administration (FDA) approved denosumab for the treatment of postmenopausal women with osteoporosis at high risk for fracture on June 1, 2010 after a study entitled Fracture Reduction of Denosumab in Osteoporosis Every 6 Months (FREEDOM) [6].
It also approved new indications for denosumab for the treatment of bone loss in patients with prostate or breast cancer undergoing hormone ablation therapy on September 19, 2011, for the treatment of bone loss in men with osteoporosis at risk for fracture on September 21, 2012, and for the treatment of adults and skeletally mature adolescents with a giant cell tumor of the bone that is unresectable or where surgical resection is likely to result in severe morbidity on June 13, 2013 (Table 1) [89].
The representative bone metastasis symptoms are called skeletal-related events (SREs). They are a devastating consequence of bone metastasis due to radiation of the bone, pathologic fracture, bone surgery, or spinal cord compression due to metastasis, producing intolerable pain, devastating physical and emotional burdens, longer hospital stays, and increased mortality [10111213]. Bone-targeted agents, such as BPs and denosumab, offer both pain reduction and SREs in the metastatic bone diseases [14].
2. Mechanism of action matching with bone remodeling cycle
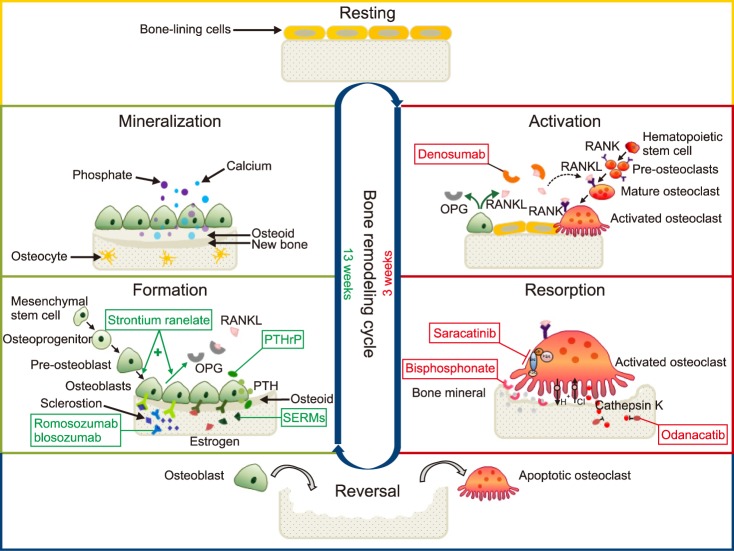
Bone is a dynamic tissue that undergoes continual adaptation through remodeling to maintain its integrity. Old bone is resorbed by the osteoclasts (bone-resorbing cells) and is replaced with new osteoids which are secreted by the osteoblasts (bone-forming cells). It is similar to the process of pavement in road repair. These clusters of osteoblasts and osteoclasts are arranged within temporary anatomical structures, basic multicellular units (BMUs), which are responsible for bone remodeling, which requires about 4 months (16 weeks including 3 weeks for osteoclastic activity and 13 weeks for osteoblastic activity) [1516].
The bone remodeling cycle is categorized into at least 6 steps: 1) the resting (quiescence) phase, 2) the activation phase (activation of pre-osteoclasts), 3) the resorption phase (resorption by the activated osteoclasts), 4) the reversal phase (the transition from bone resorption to bone formation), 5) the formation phase (bone formation by the osteoblasts), and 6) the mineralization phase (Fig. 1) [15161718].
1) During the resting phase, the bone surface is covered with flattened bone-lining cells (inactive non-remodeling forms of osteoblasts). The osteoblasts are destined to become osteocytes, bone lining cells, or undergo apoptosis [19].
2) In the activation phase,
pre-osteoclasts from the hematopoietic cells differentiate into activated osteoclasts via mature osteoclasts under the influence of the RANKL and OPG, secreted from the osteoblasts. Denosumab, like OPG (a decoy receptor produced by osteoblasts), binds the RANKL and prevents the RANKL from binding to the RANK, inhibits the differentiation steps from pre-osteoblasts via mature osteoclasts to activated osteoclasts, and finally reduces bone resorption [2021].
3) In the resorption phase,
activated osteoclasts break down the old bone mineral and matrix in order to create an erosion cavity. This phase ranges from the time of osteoclast adherence to the bone to the release of calcium and phosphate ions into the blood stream. This osteoclastic bone resorption is controlled by 4 main hormones: calcitonin, parathyroid hormone, vitamin D3, and estrogen [22]. BPs bind to the bone mineral and take the space where activated osteoclasts attach at sites of bone resorption. Even though the disabled osteoclasts survive, they cause loss of resorptive function [3]. Odanacatib, a cathepsin K inhibitor, inhibits the osteoclastic enzyme that degrades collagens. Saracatinib, a c-src inhibitor, inhibits osteoclastic activation. Selective estrogen receptor modulators (SERMs) and hormone (estrogen) replacement therapy interfere with various osteoblast-derived factors that stimulate osteoclasts.
4) In the reversal phase (from bone resorption to formation), mesenchymal stem cells prepare the bone surface for new osteoblasts (with several steps from osteoprogenitors via pre-osteoblasts to osteoblasts) to start building bone.
5) In the (bone) formation phase, mature osteoblasts synthesize new bone matrix. Strontium ranelate stimulates pre-osteoblasts to differentiate into osteoblasts, and stimulates osteoblasts to secrete OPG in order to prevent pre-osteoclasts from becoming activated osteoclasts via mature osteoclasts, as well. Parathyroid hormone (PTH) analogues and PTH-related protein (PTHrP) analogues increase the number and activity of osteoblasts. Romosozumab (AMG 785) and blosozumab, anti-sclerostin monoclonal antibodies, bind to the sclerostin (a glycoprotein inhibitor of osteoblast Wnt signaling produced by osteocytes) and inhibit its action [23].
3. Pharmacodynamics
After subcutaneous administration of 60 mg of denosumab, the bone resorption marker, serum type 1 C-telopeptide(CTX), reduced approximately 85% after 3 days, with maximal reductions occurring at 1 month. The level decreased below the limit of assay quantitation (0.049 ng/ml) in 39% to 68% of patients in 1 to 3 months. It maintained a decreased state of a maximal reduction of 45% to 80% 6 months after administration, and returned to baseline within 12 months. The degree of inhibition of CTX in re-initiation of denosumab was similar to that of its initial use [25].
Consistent with the physiological coupling of bone formation and resorption in bone remodeling, the bone formation markers, such as osteocalcin and procollagen type 1 N-terminal peptide (P1NP), are also reduced subsequently.
4. Pharmacokinetics
After a single subcutaneous injection of 60 mg of denosumab in healthy volunteers, the mean maximal serum concentration was reached at 10 days, and the mean half-life was 25.4 days, and declined over a period of 4 to 5 months [9]. There was no accumulation or change in the pharmacokinetics of denosumab over time in those who take it every 6 months. It did not show any differences in pharmacokinetics related to age, race, body weight, or hepatorenal function. Carcinogenesis, mutagenesis, or impaired fertility has not reported [26].
5. Precautions related to contraindications and complications
1) Contraindications
The known common contraindications of denosumab are hypocalcemia, pregnancy, and hypersensitivity to denosumab, such as anaphylaxis, facial swelling, and urticaria [27].
Hypocalcemia should be corrected before using denosumab, because it exacerbates preexisting hypocalcemia for weeks or months. If hypocalcemia persists, intravenous or oral calcium with/without vitamin D should be supplied. Therefore, monitoring of calcium with phosphorus and magnesium levels is strongly recommended.
In addition, in cases of mineral metabolism disturbances, such as a history of hypothyroidism, thyroid surgery, parathyroid surgery, malabsorption syndrome, excision of the small intestine, or severe renal impairment (creatinine clearance < 30 ml/m or receiving dialysis), frequent monitoring of calcium and other electrolytes is required.
2) Complications
The known complications related to denosumab are hypersensitivity, hypocalcemia and mineral metabolism abnormality, osteonecrosis of the jaw, atypical femoral fractures, serious infections such as cellulitis, musculoskeletal pain, and suppression of bone turnover [28].
The risk of osteonecrosis of the jaw (ONJ) may increase in invasive dental procedures with duration of exposure to denosumab. Atypical subtrochanteric and diaphyseal fractures were also reported in patients receiving denosumab.
Serious skin, abdomen, urinary tract, or ear infections were frequently reported in denosumab-treated patients. It is important to consider the risk of serious infections in patients with immunosuppressed states or on concomitant immunosuppressant agents. The incidence of dermatologic adverse reactions, including dermatitis, eczema, and rashes, increased.
Musculoskeletal pain, such as bone, joint, and/or muscle pain, has been reported from 1 day to several months after taking denosumab.
The most common adverse reactions leading to discontinuation of denosumab in patients with postmenopausal osteoporosis have been back pain and constipation.
6. Preparation and administration methods
Denosumab (60 mg/1 ml of Prolia® or 120 mg/1.7 ml of Xgeva®) is a clear, colorless to pale yellow (not discolored or cloudy) solution, however, it may contain some trace of translucent and white proteinaceous particles. Before administration, it should be kept at room temperature for 15 to 30 minutes after removal from the refrigerator. This single-use prefilled syringe with a green safety guard has a 27-gauge needle with a cap [29].
A subcutaneous injection, not into the skin or muscle, should be given into the upper anterior thigh, arm, or abdomen every 6 months. It is recommended that all patients receive 1000 mg of calcium and at least 400 IU of vitamin D daily [30].
7. Future development in the use of denosumab
It would be ideal to develop a hybrid molecule in which BPs may serve as a vehicle for the delivery of denosumab selectively to the bone in order to reduce the effect on the immune system along with an increased antiresorptive activity [31].
It is promising to use denosumab in rheumatoid arthritis with focal pathologic bone resorption due to excessive activity of the osteoclasts, combined with an anti-tumor necrosis factor (TNF) agent or with disease modifying anti-drugs (DMARDs) [32].
CONCLUSIONS
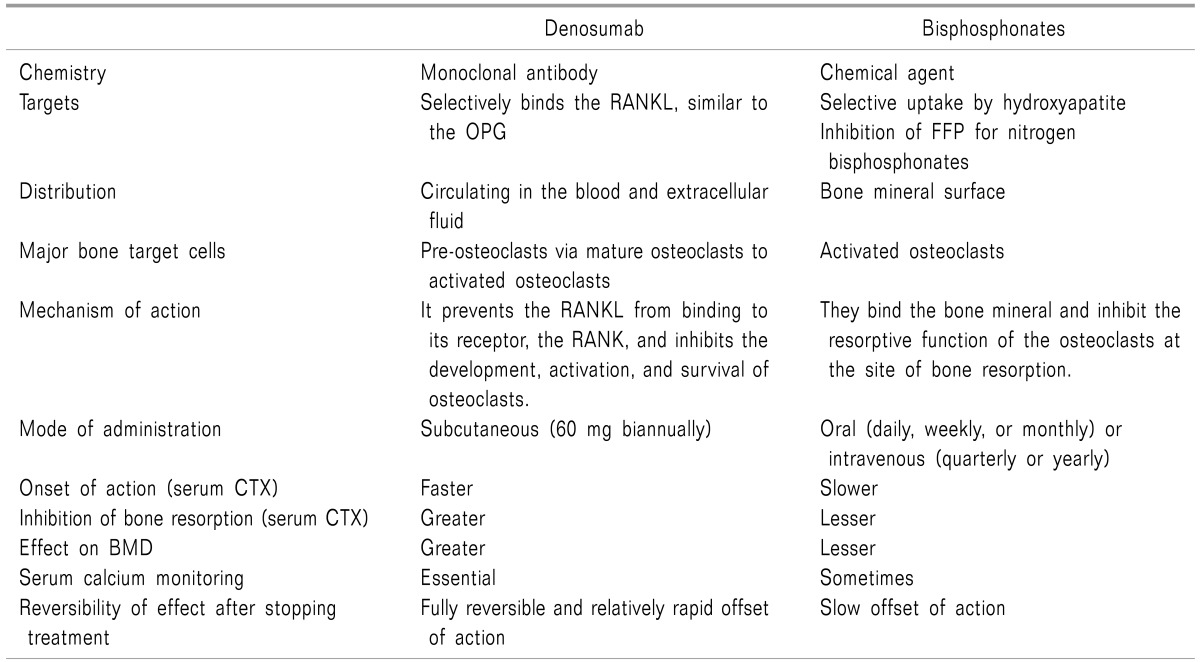
Denosumab prevents the RANKL from binding to its receptor, the RANK, thereby inhibiting the development, activation, and survival of osteoclasts; however, the familiar antiresorptive agents, BPs, bind to the bone mineral and inhibit the resorptive function of osteoclasts by being taken up by osteoclasts at the site of resorption, though the disabled osteoclasts may persist. The two antiresorptive agents are unlikely to be used in combined treatment due to the inhibitory action of osteoclasts in the same pathway. It is more reasonable to use combined anabolic and anti-catabolic treatment [33].
Therefore, even though denosumab has better compliance (a single subcutaneous injection every 6 months) with rapid onset, strong inhibition of osteoclastic activity, reversibility of its action after discontinuance, and advantages to patients with gastrointestinal trouble and impaired renal function, the economic status and cost/benefit comparison, the immune status with infection susceptibility, and compliance with taking calcium/vitamin D supplements and frequent monitoring of calcium or other minerals should be considered (Table 2).
 XML Download
XML Download