

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Lumbar sympathetic ganglion block (LSGB) and neurolysis have been used for more than 70 years to manage patients with complex regional pain syndrome, vascular disease and hyperhidrosis of the lower extremity [1]. This procedure is considered safe, but practitioners should be aware of the anatomy to avoid complications [2].
The paramedian approach is a usual technique that can be used in either the prone or lateral position. The needle is inserted 5-8 cm lateral to the midline at the L2-4 level [3]. Rotating fluoroscopic images of the affected side until the spinous process reaches the contralateral margin of vertebral body would help make the procedure easier [4]. Previous studies recommended an entry angle of 35-45° during the paramedian approach [5]. However, there are no reports on the safe entry angle on Korean adults. Entry angle of about 25-30° has been used in our institution by experience. The purpose of this study is to determine the safe and accurate entry angle and entry point in Korean using the abdominal CT scan images. In addition, this study analyzed the differences of entry angle and entry point among the L2, 3, and 4 levels, between males and females, between right and left approach, differences according to age, and correlation with body mass index (BMI).
MATERIALS AND METHODS
The study was approved by the Institutional Review Board of our institution. Eighty-five outpatients who previously had their abdominal CT images taken were enrolled in this study. A picture archiving and communication system was used to view the images in this retrospective study between June 2008 and December 2008. Patients with an intraperitoneal mass or those with a history of spinal surgery, which led to anatomical variation, were excluded.
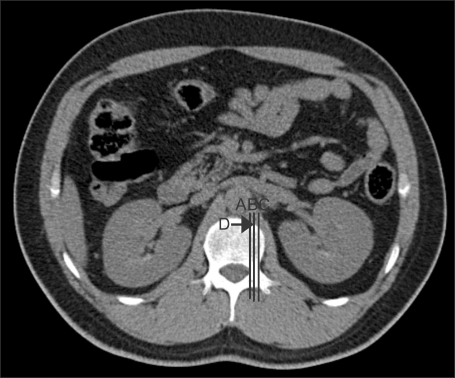
This study was performed on the assumption that the target point was aimed at the lateral border of vertebral body using an oblique position of fluoroscopy by tunnel vision technique. The entry angle on the L2, L3, and L4 levels, where the lumbar sympathetic ganglion resides, was obtained using the abdominal CT images of the patients to avoid the contact with the transverse process. The usual location of lumbar sympathetic ganglion is the anterolateral aspect of vertebral body at inferior one-third of L2 level, upper one-third of L3 level, and lower one-third of L4 level [6]. Therefore, the entry angle of the right and left presumed location of the sympathetic ganglion was measured in each level on the cross-sectional CT images. Because it is ideal to position the needle tip in the shadow of pedicle in the anterior-posterior view of fluoroscopy [3], the target was pointed at the anterolateral surface of vertebral body met by the bisecting line of two lines bordering the pedicle medially and laterally (Fig. 1).
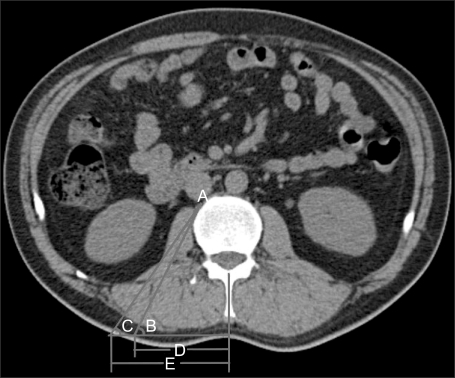
The entry angle between the skin of the back and the needle tip that was aimed at the target point was measured. Since the angle was in a constant range, the minimal and maximal angle and mean angle between the two were obtained. The entry minimal angle is the smallest angle in contact with lateral surface of vertebral body to reach the target point. The entry maximal angle is the largest angle that passes through the psoas muscle and avoids the retroperitoneal space where the kidney or ureter might be punctured. The right and left entry angle on L2, L3, and L4, and the entry distance, which is from the midline to entry point, were measured in each patient (Fig. 2).
For statistical analysis, all data was analyzed using SPSS software (version 12, SPSS Inc., USA). The measured variables were expressed as mean ± standard deviations. The difference between right and left entry angle and entry point was analyzed with Mann-Whitney test. The difference between males and females was also analyzed with this test. The Kruskal-Wallis test was used to compare the entry point and entry angle on the L2, L3, and L4 levels. This test was also used to compare among age groups. A value of P < 0.05 was considered significant. The correlations between the BMI and entry angle or entry point were analyzed using the Pearson's correlation test.
RESULTS
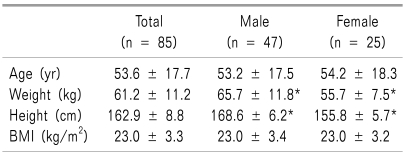
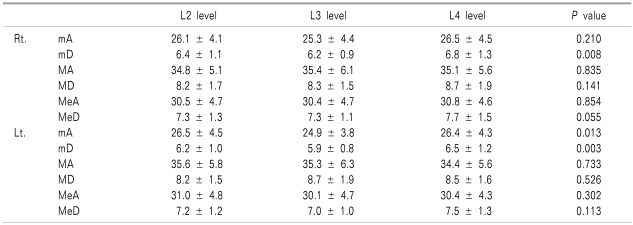
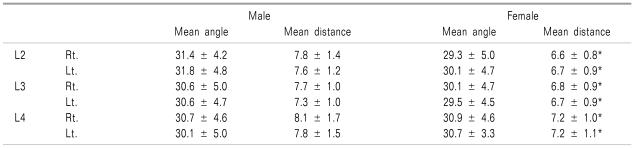
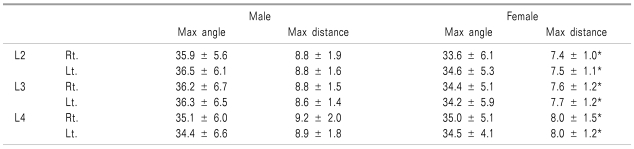
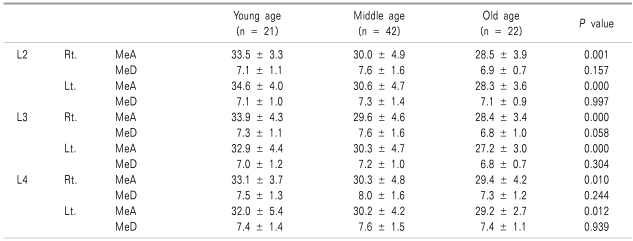
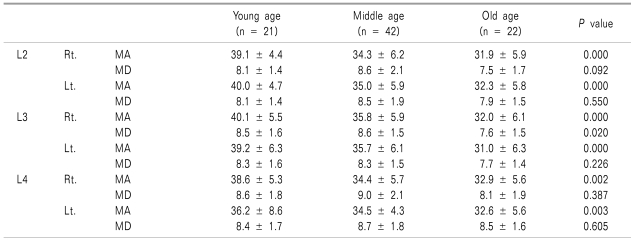
Table 1 lists the demographic data of the patients. Table 2 shows the entry angle and entry distance on the right and left levels of L2, L3, and L4. There was no significant difference among the levels of entry angle and entry distance. In addition, there was no significant difference between the right and left approaches. Table 3-6 show the entry angle and entry distance according to gender or age. The entry mean angle and distance of gender and age groups are shown in the Table 3 and 5. The entry maximal angle and distance of the same groups are shown in the Table 4 and 6.
The entry angle was similar in males and females. However, the entry distance at the L2-4 level was significantly longer in males (Table 3 and 4). The 95% confidence interval of entry mean angle was 30.5 ± 0.4° and the mean entry distance from midline was 7.7 ± 0.2 cm and 6.9 ± 0.1 cm lateral in males and females, respectively. The entry angle showed a significant difference among age groups on the L2 and L3 levels (Table 5 and 6). A significant correlation was observed between the age groups and the entry angle, which was analyzed using the Spearman's correlation test, but the correlation was low (P = 0.004, correlation coefficient = 0.310).
In addition, according to the Pearson's correlation test, there was no correlation between the BMI and entry angle but the entry distance showed a significant correlation with 5 out of 6 entry point that showed a low correlation.
DISCUSSION
Lumbar sympathetic ganglion is located on the level of L2, L3 and L4 [6] anterior to the origin of psoas muscle and anterolateral to the vertebral body in the retroperitoneal space [7].
The kidneys are located on the level of L2 and L3 vertebral body in the retroperitoneum, and the ureters are located on the level of L4 vertebral body. Therefore, there is an increased risk of puncturing the kidney and ureter if the entry angle of the needle tip is increased [2]. Normally, the somatic nerves are located posterior to the sympathetic ganglion. The majority of somatic lumbar plexus are located posterior to the psoas muscle but the genitofemoral nerve runs anteromedial to the psoas muscle. In the L2 to L5 levels, the psoas muscle separates the sympathetic chains and somatic nerves that are connected by the rami communicantes, which forms a fibrous tunnel running lateral to the vertebral body. Care must be taken because this tunnel might allow the neurolytic agent that is injected around the sympathetic ganglion to flow into the somatic nerve [8]. The drug can be injected in the epidural space or intrathecally because the intervertebral foramen is located in the posteromedial border of sympathetic ganglion. In addition, intravascular injections are possible because the inferior vena cava lies at the right side and the abdominal aorta lies at the left side anterior to the ganglion, and the copious large number of lumbar arteries and veins develop around the sympathetic chains [2,8].
There was no difference between the entry angle of males and females in this study. However, there was a significant difference in the entry distance because the distance from skin to the target point might be longer in males due to the effect of the larger volumes of paraspinal muscles and subcutaneous tissue, even though the actual distance was not measured in this study. These results about entry distance may be an additional indicator for practitioners because the entry angle is more important than the entry point when using fluoroscopy, which is currently the standards for the safety and accuracy in performing LSGB.
If the vertebral body forms a bony spur, the entry angle was measured at a section of the image that avoids contact with the bony spur. In this case, the margin of safety in the entry angle decreases due to an increase in accessible minimal angle, and the maximal angle does not change if a bony spur is formed. This is also similar when the width of the vertebral body is wide. However, the margin of safety increases with increasing entry maximal angle if the volume of psoas muscle increases. The formation of bony spur of the vertebral body is related to ages [9]. The entry angle decreased with age probably because the volume of the muscles decreased as a result of the progression of the degenerative changes and atrophy as the patients age [10], and these changes in the paraspinal muscle may have a larger effect than those with bony spur.
The BMI and average entry angle were not associated with each other in this study. The relationship between the BMI and volume of paraspinal muscle has not been reported. However this study suggests that there is an increase in the volume of tissue that lies from the skin to the paraspinal muscles instead of the paraspinal muscle itself when the BMI increases. This increase would not affect the entry angle during LSGB.
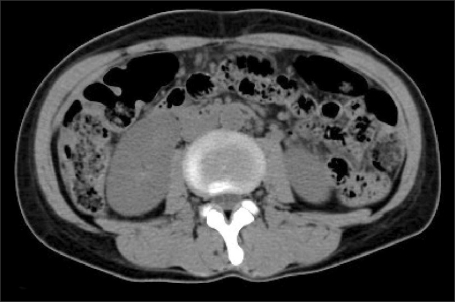
There are reports about injuries after LSGB in patients with complex regional pain syndrome. According to one report, the right proximal ureter was injured, and a ureteroureterostomy had to be performed and a ureter stent was inserted [11]. Furthermore, many other ureter injuries after LSGB have been reported [12,13]. In addition, a massive subcapsular hematoma was observed after LSGB [14]. In this study, four patients excluded had CT images indicating that the kidney would be punctured, even if the entry angle was made as small as possible in the L2 and L3 levels. These patients had peritoneal malignant carcinoma or ascites, which compressed the kidneys deep into the retroperitoneal space so the injury to the kidney during LSGB would not be avoided if abdominal CT image was unavailable (Fig. 3).
The maximal entry angle was measured to determine the optimal angle for the accurate procedure of LSGB in this study. But, if the mean value of maximal entry angle is suggested, the risk of complications increases for patients with a small maximal entry angle. Therefore the mean entry angle, which is the average of the minimal and maximal entry angles, was measured. Based on this background, the 95% confidence interval of entry mean angle was 30.5 ± 0.4°. And there was no risk of puncturing the kidney in all patients enrolled in this study using this entry mean angle. And the 95% confidence interval of entry mean distance was 7.7 ± 0.2 cm and 6.9 ± 0.1 cm for males and females, respectively.
Seo et al. [15] performed LSGB on the L3 level under the same conditions as this study using a tunnel vision technique and fluoroscopy. They reported that the oblique angle of fluoroscopy was 22.0 ± 3.8° and distance from the spinous process to the entry point was 6.5 ± 1.0 cm. They measured that the oblique angle when the transverse process of the affected side reaches the margin of the vertebral body in the prone position using fluoroscopy. The bony contact was made at almost halfway in the lateral surface of vertebral body when the needle is inserted in this angle using a tunnel vision technique to pass through the margin of vertebral body. The needle was advanced further to reach the target with stimulating the periosteum. The suggested angle in this study was larger than this angle, so there would be advantages in decreasing the stimulation of periosteum, thereby allowing further advances near the target point, and minimizing the changes in the entry angle according to the length of transverse process.
There were several limitations in this study. The reproducibility of the angle measurement decreased because the imaginary target point of LSGB was not designated accurately as a single point. However, the error was not extensive because there was a large number of subjects.
In addition, there may be differences in anatomy between the prone or lateral position when performing the procedure and supine position when the abdominal CT was taken. However, this difference was negligible because only lordosis of the spine decreases in the prone position compared to the supine position, which has little effect on the entry angle.
In conclusion, the entry angle is similar regardless of the level or whether it is performed on the right or left during LSGB in Korean adults. With a 30° oblique view of fluoroscopy to the affected side, the approach of the needle using a tunnel vision technique to the lateral margin of vertebral body would be safe and accurate, and minimize the level of patients' discomfort. Although the suggested entry angle is considered safe for all ages, it is important to consider that the entry angle decreases with age. Practitioners should be aware of the increased risk of puncturing the kidneys or ureters if the kidneys are positioned deep inside the retroperitoneum because of the possible presence of tumors in the peritoneal cavity. The success rate can be increased and complications decreased by measuring the entry angle and entry distance of the patients who had taken abdominal CT scans before the procedure regardless of the existence of abdominal tumor.
 XML Download
XML Download