

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sleep disturbances such as insomnia, nightmare, or sleepwalking are commonly reported in children and adolescents, with its prevalence ranging from around 11% to 40%, depending on the reported symptom.12 Research has shown that insufficient sleep and sleep disturbances can cause decreased cognitive and behavioral functions.345 In addition, long-term sleep disturbances in youth are often associated with negative consequences, such as decreased neurobehavioral functioning, behavior, mood, and mental health problems throughout adolescence.678
However, only a number of children are properly diagnosed and receive treatment. For example, one study investigated medical charts for 2 years of children that reported sleep problems. While aspects about their sleep qualities have been addressed in some cases, the study reported effective intervention for only 3 cases among 103 reported disturbances. This result was attributed to parents’ concerns about other development factors such as language development, causing sleep problems to go largely unnoticed.9 Symptoms such as sleep disturbance require careful observations and communications with the child. Therefore, if parents fail to notice their sleep disturbances, such symptoms are likely to go undetected and left unattended.
Parent-child discrepancy in reporting psychiatric symptoms is common. Research in this area has revealed multiple contributing factors, such as parents’ psychological distress,10 type of reported behavior,11 and child’s sex.12 For example, depression and anxiety in children and adolescents showed substantial levels of parent-child discrepancies.131415 In adolescents, a significant proportion of parents were unaware of suicidal thoughts and plans.16 In addition, parents’ occupations, and subsequently, time spent with child had indirect effects on discrepancy scores in children with mood disorder symptoms.17 Despite numerous research on parent-child discrepancies, only a number of research has focused on parent-child discrepancies regarding sleep.18
In this study, our goal was to investigate the association between diagnosis and mother-adolescent discrepancy in reporting sleep disturbances in psychiatric clinic. We additionally aimed to evaluate whether this association is affected by sex and mother’s occupation.
METHODS
Data collection
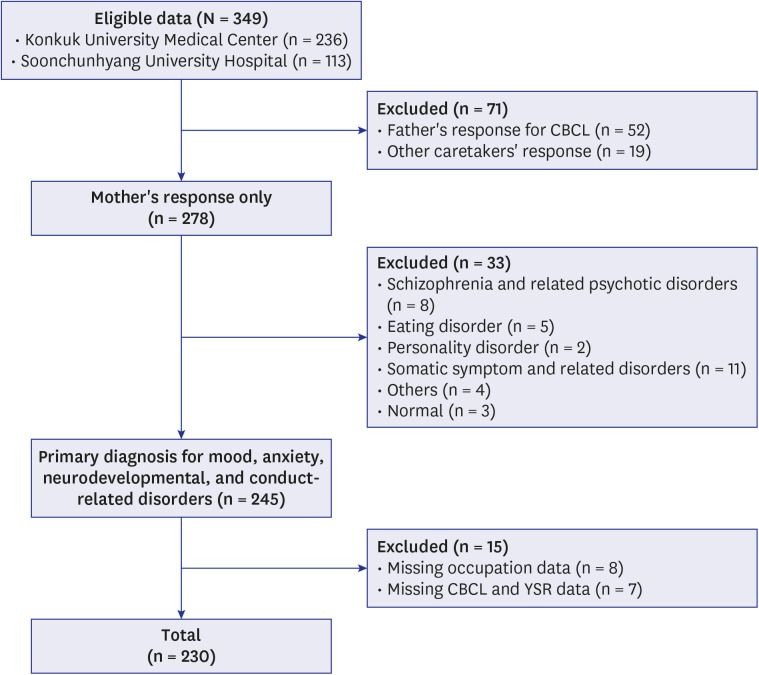
This study was a multi-center retrospective study on patient data from 2014 to 2020 August at Konkuk University Medical Center and Soonchunhyang University Hospital, both located in Seoul, Korea. Patients included male and female adolescents from age 12 to 18 who visited psychiatric outpatient clinic. Data were obtained from the patients’ electronic medical records. Exclusion criteria included 1) Child Behavior Checklist (CBCL) response from caretaker other than the mother; 2) adolescents diagnosed with disorders other than mood, anxiety, neurodevelopmental, or disruptive, impulse-control, and conduct disorder; and 3) missing data needed for analysis, such as mother’s occupation or Youth Self-Report (YSR) and CBCL items related to sleep. A total of 230 data were analyzed as a result. Data selection process is summarized in Fig. 1.
Measures
Diagnosis
Diagnoses were made by psychiatrists through a clinical interview, based on DSM-5.19 The diagnoses were grouped into 4 categories. Diagnoses of bipolar and related disorders and depressive disorders were grouped and coded as mood disorder. Diagnoses of anxiety disorders, obsessive-compulsive and related disorders, and trauma- and stressor-related disorders were grouped and coded as anxiety disorders. Diagnoses of neurodevelopmental disorders include attention-deficit hyperactivity disorder, autism spectrum disorder as well as motor disorders such a tic disorder. Diagnoses of disruptive, impulse-control, and conduct disorders include oppositional defiant disorder, conduct disorder, and intermittent explosive disorder.
YSR and CBCL
YSR and CBCL are parallel tests that assess the same variables. YSR is completed by children in a self-report form, while CBCL is completed by parents or other caretakers. To control for type of informant, only mother’s responses were collected. YSR and CBCL were developed by Achenbach and Rescorla20 and it was translated and validated in Korean by Oh et al.21 Responses are measured by three-point Likert scale, indicating whether the item is not true (0), sometimes/somewhat true (1), or very/often true (2). Sleep-specific items (items 47, 76, 77, and 100) included nightmares, sleep less than most kids, sleep more than most kids during day and/or night, and trouble sleeping. Their scores were summed to produce a composite score to indicate overall sleep disturbance,22 ranging from 0 to 8. To produce parent-child discrepancy scores, YSR sum was subtracted by CBCL sum. Therefore, discrepancy scores could range from −8 to 8, where positive scores indicate child’s reported sleep disturbance to be larger than parent’s report, and vice versa. Larger absolute scores indicate the magnitude of the discrepancy.
Data analysis
Data was first screened for normality. The residual plot supported the normality of the data.23 The skewness was 0.25 (standard error [SE] = 0.16) and kurtosis was 0.42 (SE = 0.32). Results for Levene’s test supported homogeneity of variance (F(15, 214) = 0.87, P = 0.600).
As all assumptions were met, a 2 × 4 × 2 analysis of variance (ANOVA) was conducted for sex (male/female), primary diagnosis type (mood/anxiety/neurodevelopmental/conduct-related), and mother’s occupation (working/homemaker). Significance was evaluated for main effects of sex, primary diagnosis type, and mother’s occupation status. As for interactions, significance was evaluated for both two-way (e.g., sex × primary diagnosis type) and three-way (e.g., sex × primary diagnosis type × mother’s occupation status) interactions. In cases of significant interactions, further comparisons were performed using t-tests to elucidate the simple effects between cells. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 20.0. (IBM Corp., Armonk, NY, USA), with P values ≤ 0.05 considered statistically significant.
RESULTS
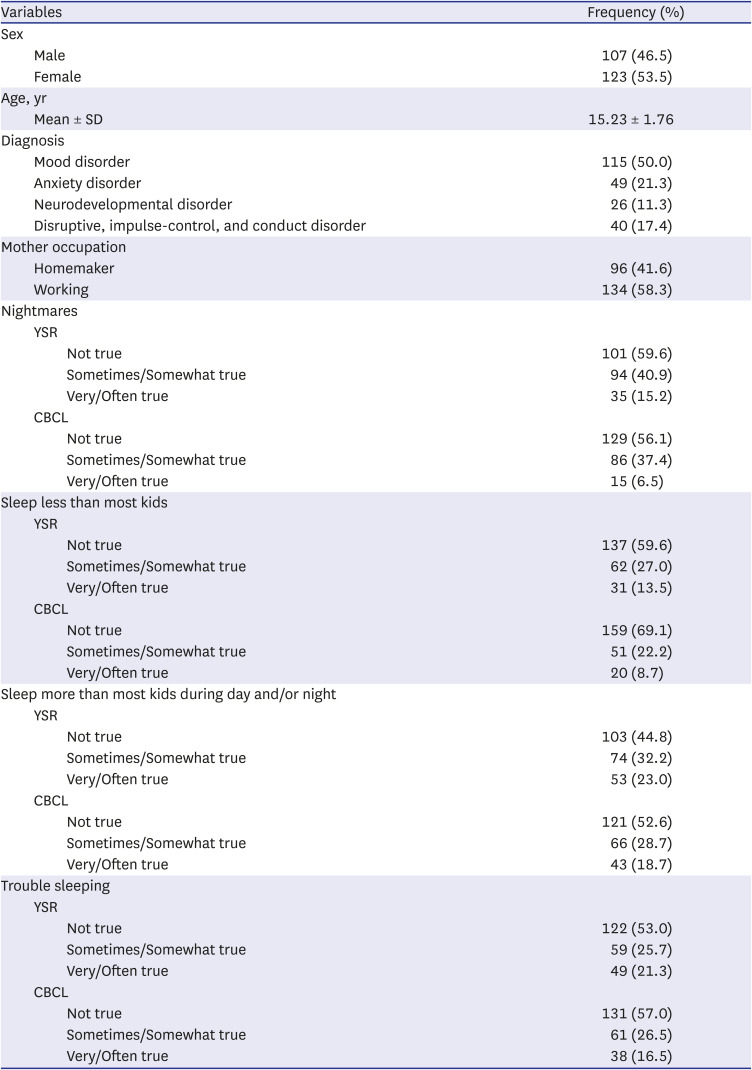
A total of 230 subjects were included in the analyses. Their age ranged from 12 to 18 (mean = 15.23, standard deviation [SD] = 1.76). The 47% were aged 16 or above (n = 108) and 53% (n = 122) were aged 12 to 15. The 46.5% (n = 107) of the participants were male and 53.5% (n = 123) were female. The 50% of children/adolescents were primarily diagnosed with mood disorder (n = 115), 21.3% with anxiety disorder (n = 49), 11.3% with neurodevelopmental disorder (n = 26), and 17.4% with disruptive, impulse-control, and conduct disorder (n = 40). As for mother’s occupation, 41.6% was homemaker (n = 96) and 58.3% were currently working (n = 134). Table 1 summarizes the demographic information of sample data and frequency of response on each sleep-related items on YSR and CBCL.
Table 1
Demographic information of the sample
Prior to the main analysis, an independent samples t-test was conducted to check for any significant differences between those age 16 or above and those aged 12 to 15. The result revealed the difference to be non-significant (t = − 0.77, P = 0.443). Therefore, age was excluded from the analysis.
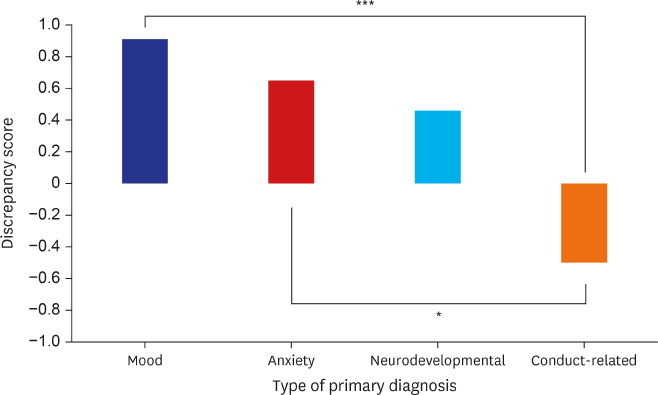
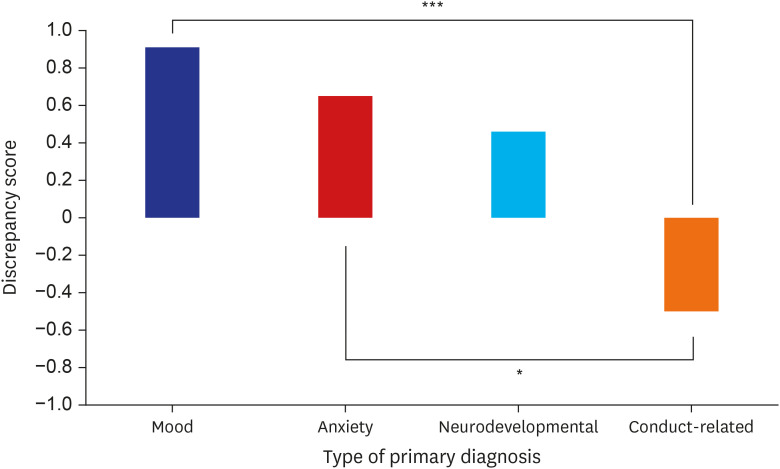
The 2 (sex: male/female) × 4 (diagnosis: mood/anxiety/neurodevelopmental/conduct-related) × 2 (mother occupation: homemaker/others) ANOVA revealed main effect of diagnosis (F(3, 214) = 3.51, P = 0.016, η2
= 0.047). Pairwise comparisons revealed significant differences of parent-child discrepancy scores between mood and conduct-related disorder (t(153) = 3.58, P < 0.001), where scores for mood disorder (mean = 0.91, SD = 2.07) was 1.41 points greater than that of conduct-related disorder (mean = −0.50, SD = 2.39). Difference between anxiety and conduct-related disorder was also significant (t(87) = 2.51, P = 0.014), where scores for anxiety disorder (mean = 0.65, SD = 1.94) was 1.15 points greater than that of conduct-related disorder (mean = −0.50, SD = 2.39). These results indicate that for adolescents with mood or anxiety disorders, their parents rated their sleep disturbances to be less problematic than those with conduct-related disorders, where their parents rated their sleep disturbances to be more problematic. Table 2 summarizes the composite scores for sleep-related items on YSR and CBCL and their discrepancy scores by each diagnosis type. The main effect of primary diagnosis type is illustrated in Fig. 2.
Table 2
Frequency of scores for sleep-related items on YSR and CBCL

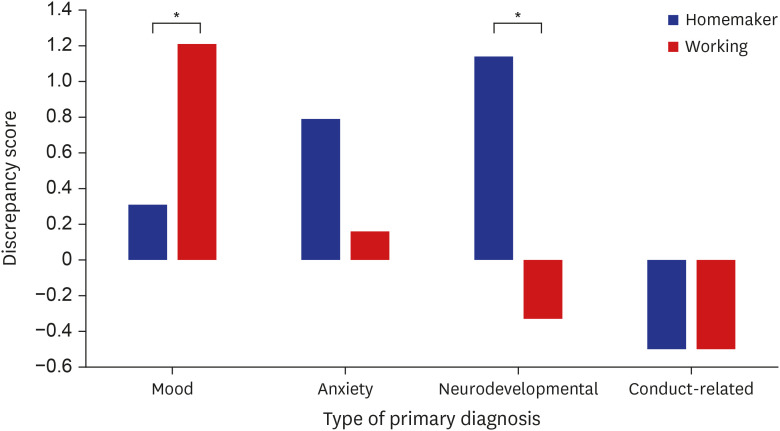
In addition, the diagnosis × mother occupation interaction was significant (F(3, 214) = 3.21, P = 0.024, η2
= 0.043). To elucidate this interaction, discrepancy scores were compared using t-tests for each diagnosis type. For mood disorder, the discrepancy scores were significantly smaller (t(115) = −2.32, P = 0.022) for those with homemaker mothers (mean = 0.31, SD = 2.07) compared to those with working mothers (mean = 1.21, SD = 2.00). For neurodevelopmental disorder, the discrepancy scores were significantly greater (t(24) = 2.08, P = 0.049) for those with homemaker mothers (mean = 1.14, SD = 1.99) compared to those with working mothers (mean = −0.33, SD = 1.56). Differences for anxiety and conduct-related disorders were not significant. The summary of interaction effect is visualized in Fig. 3.
DISCUSSION
The current research retrospectively analyzed factors affecting parent-adolescent discrepancy of sleep disturbance ratings. Results showed main effect of primary diagnosis type, indicating higher discrepancy scores for adolescents with mood and anxiety disorders, such that parents rated sleep disturbances to be less problematic than the adolescents. On the other hand, for adolescents with conduct-related disorders, parents rated their sleep disturbances to be more problematic than they did. Furthermore, this effect also interacted with mother’s occupation status. For adolescents with mood disorders, working mothers rated their sleep disturbances to be less serious compared to homemakers. An opposite relationship was found for adolescents diagnosed with neurodevelopmental disorder, where homemaker mothers underrated their sleep disturbances.
Differences in discrepancy scores by diagnosis type is largely consistent with previous research showing larger discrepancies for adolescents with internalizing disorders.111315 Internalizing disorders are characterized by disordered mood and emotion, such as mood and anxiety disorders. Therefore, internalizing disorders tend to possess symptoms that are relatively quiet, such as withdrawal or inhibition than externalizing disorders.24 This makes it more difficult for parents to attend to and recognize internalizing symptoms.15 In addition, many adolescents sleep separately from parents. Therefore, unless parents pay keen attention to their children’s sleep quality, it is difficult to recognize when sleep disturbances are present. Combined with subtle symptoms of internalizing disorders, this explains larger adolescent-report scores compared to parent-report scores.
On the other hand, externalizing disorders such as conduct-related disorders are characterized by dysregulated behavior, including aggression and disinhibited behaviors. Compared to internalizing disorders, externalizing disorders are easily observable and thus show better parent-child agreements.2526 This was supported by smaller deviation from 0 discrepancy score for conduct-related disorders compared to mood and anxiety disorders in this study. Research has indicated sleep disturbances to be significantly more common in children with conduct-related disorders.27 Furthermore, sleep disturbances have been shown to be associated with conduct problems28 and may predict emotion dysregulation29 and poor school adjustment.30 Behavioral symptoms easily observed in children with externalizing disorders can lead to increased parental monitoring and sensitivity regarding children’s conditions. Therefore, parents may be more attentive towards children’s overall sleep quality.
The results also showed interaction effect of primary diagnosis type and mother’s occupation on parent-child discrepancy scores. For adolescents diagnosed with mood disorder, working mothers underrated their sleep disturbances compared to homemaker mothers. In cases of internalizing disorders, more time and effort are needed for parent-child communication regarding its symptoms. To this regard, homemaker mothers may naturally be more advantageous than working mothers, as they would spend more time with their children. A previous research also has shown that time spent with child is significantly related to mothers’ reports of internalizing behavior.17 This finding offers considerations for clinical practice regarding mother’s occupation and its possible contributions to parent-child discrepancies in reporting child’s symptoms. Practitioners must explore any self-reported sleep disturbances in adolescents with internalizing disorders, as they are likely to go undetected by parents, especially in cases where parent-child communications may be difficult. As sleep disturbances and disorders present as symptoms and overlap with depression and anxiety disorders,31 it is important to recognize when such disturbances are present in children. Furthermore, research has shown children’s self-reports of sleep to be valid,18 indicating that meaningful information can be extracted from children regarding their sleep conditions.
For adolescents diagnosed with neurodevelopmental disorder, an opposite effect emerged. Homemaker mothers significantly underrated children’s sleep disturbances compared to working mothers. A few factors may have contributed to this result. First, adolescents with neurodevelopmental disorders have been reported to experience various sleep disturbances due to pathophysiological factors or physical and psychiatric comorbidities associated with neurodevelopmental disorders.32 This can lead to developing sleep habits such as co-sleeping, especially in Korean culture where co-sleeping is common and traditional.33 Co-sleeping can affect the discrepancy scores, although proper investigation is needed to elucidate this effect and the role of mother’s occupation in this relationship. Second, as adolescents with neurodevelopmental disorders require additional help to function, parenting stress levels may differ by mother’s occupation, and thus differentially impact parent-child discrepancy. Studies show symptoms of neurodevelopmental disorders, such as hyperactivity or behavioral disabilities, can cause larger than normal parenting stress.3435 Parenting stress increases the risk of developing depression,36 which can in turn impair accurate ratings of current child conditions.37 As sleep disturbances can put adolescents at further risk for impaired cognition and learning abilities,32 how these factors can interact should be investigated. For example, behavioral measures for sleep can be used to provide objective and more accurate measures of sleep for comparing parents’ and adolescents’ reports. Parents’ stress levels should also be taken into account when evaluating parent-child discrepancy. Finally, self-report issues can be more significant in adolescents with neurodevelopmental disorders. Previous research on adolescents with neurodevelopmental disorders has attributed the discrepancies to their low adaptive functioning38 and abnormal self-perceptions.39 These factors can affect YSR scores and subsequently overall discrepancy scores.
The study has several limitations. First, the sample size may have been limited to generalize the results across general population. Second, as co-sleeping habits are frequent in Korean culture,33 it would have been useful to take into account as a control variable. Moreover, co-sleeping is also affected by financial status and number of children within the family such that co-sleeping would increase with lower financial status4041 and increased number of children. Therefore, additional factors such as financial status and number of children should be taken into account. Third, the current study only measured self-reports of parents and adolescents. This makes it difficult to evaluate whether their reports accurately reflect adolescents’ sleep disturbances. To this end, future studies may also employ behavioral measures of sleep. The use of objective measures would allow for evaluating accuracy of parents’ and adolescents’ reports. In addition, the current study did not consider mother’s job nor work type. For example, mothers with relatively low-demanding jobs that do not require going to work every working day may be more advantageous than those with demanding jobs. Finally, as discrepancy scores are also affected by parents’ scores, it is important to consider their psychiatric evaluations alongside the adolescents’ diagnosis. Also, with regards to clinical diagnosis, future studies may employ a variety of diagnostic methods other than clinical diagnosis used in the current study. These improvements may yield meaningful results in future studies.
This study illustrates differential patterns of parent-child discrepancies of sleep ratings by primary diagnosis. The results extend from previous research regarding parent-child discrepancy for internalizing disorders to adolescents’ sleep disturbances. This holds clinical implications for practitioners, emphasizing the need to further explore self-reported sleep disturbances in adolescents, especially in those with mood disorders. In addition, mother’s occupation should also be taken into account when evaluating parents’ and adolescents’ reports of sleep. Future studies may investigate other variables that can also affect such discrepancies, such as maternal psychopathology.37
 XML Download
XML Download