

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Total hip arthroplasty (THA) is an effective and favored surgery procedure to treat advanced degenerative arthritis in the hip joint.1 As the aging population increases, the frequency of performing THA for hip arthritis and hip fracture is increasing.234 Also, the frequency of THA at a young age is increasing due to the increase in steroid-induced osteonecrosis of femoral head.56 Therefore, securing the longevity of THA and decreasing postoperative complications rate are important issues in hip arthroplasty.
Cementless THA has been popularized worldwide.789 However, postoperative bone loss of the proximal femur and thigh pain remain matters of concern of cementless THA.1011 Thigh pain is an annoying problem to patients, which compromises their activity and satisfaction. Theoretically, a more physiologic load transfer to the proximal metaphysis of the femur can be obtained by shortening the stem length.12 With an expectation to reduce the stress shielding and the thigh pain, various short stem designs with different shape, length and taper angle, have been introduced over the last two decades and are currently in use.8131415
In the literature, short stems provided excellent clinical and radiological results.8131516 However, the incidence of thigh pain after the use of short stems widely varied from 1% to 24%,111718 and there is a serious debate as to whether these short stems really reduce the incidence of thigh pain.1920 While earlier studies reported that the use of short stems reduced the thigh pain incidence compared to standard-length stems,2122 a recent study showed no significant difference between the two stem designs.11
Khanuja et al.23 classified short stem designs into 4 categories: 1) femoral neck only, 2) calcar loading, 3) calcar loading with lateral flare and 4) short tapered. In North America, the most favored short stem design is type 4 short tapered stem, which is shorter than their counterpart standard length stem by 30 to 35 mm.1124 There is a paucity of studies comparing the thigh pain incidence of type 1, 2, 3 short stems with standard length stems.
Therefore, we conducted a systematic review and meta-analysis to determine whether short tapered stems reduce the incidence of thigh pain compared to the standard-length tapered stems.
METHODS
The current review and meta-analysis were done according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.25 This protocol has been registered in the International Prospective Register of Systematic Reviews (PROSPERO Number CRD42021231240).
Study eligibility criteria
Studies were selected by means of the following criteria:
(1) Study design: retrospective comparative studies, prospective comparative studies, randomized controlled trials (RCT)s;
(2) Study population: patients with total hip arthroplasty or hemiarthroplasty for hip diseases or hip fractures;
(3) Intervention: hip arthroplasty using type 4 short tapered stems according to the classification by Loppini et al.8 and Khanuja et al.23 and standard tapered stem;
(4) Outcomes: postoperative thigh pain, demographic factors, and other clinical results.
(5) Studies were excluded if they 1) did not meet the above criteria or 2) were posters, letters, or review articles.
Search methods for identification of studies
We used PubMed Central, OVID MEDLINE, Cochrane Collaboration Library, and Embase for a comprehensive search for all relevant studies, up to January 2021. We used the following search terms: (“short” [All Fields] OR “shorts” [All Fields]) AND (“stems” [All Fields] OR “stem” [All Fields]) AND (“conventional” [All Fields] OR “conventionals” [All Fields]) AND (“arthroplasty” [MeSH Terms] OR “arthroplasty” [All Fields] OR “arthroplasties” [All Fields]) AND (“hip” [MeSH Terms] OR “hip” [All Fields]) (Supplementary Table 1). We also did a manual search of possibly related references. Two of us reviewed the titles, abstracts, and full texts of all potentially relevant studies independently, as recommended by the Cochrane Collaboration.26 Any disagreement was resolved by the third reviewer. We performed full-text review of screened studies according to the predefined inclusion/exclusion criteria, and then selected eligible articles. The reviewers were not blinded to authors or institutions of the studies.
Data extraction
The data that were extracted from the articles included: authors, date of publication, design of the study, demographic features (number of hips, age, sex), postoperative follow-up period, specific interventions (hip arthroplasty with short tapered stem versus standard tapered stem), definition and incidence of thigh pain.
Data analysis
For dichotomous results, we calculated the risk ratio (RR) and the confidence interval (CI) of 95%. The heterogeneities of the studies were tested using Higgins I2 statistics and the χ2 test.27 When P value was < 0.10 and I2 was > 50%, the studies were considered heterogeneous. Otherwise, the studies were considered not to have definite heterogeneity. When there was little evidence of heterogeneity, the risk of thigh pain was assessed using fixed-effects models. Otherwise, random-effects models were used.2829 Sensitivity analysis was conducted by omitting a single study each time and building data from the remaining studies to explore possible high heterogeneity and to assess the outcome stability.
We used subgroup meta-analysis on comparative studies or RCTs between short tapered stem and standard tapered stem. The trim and fill method was used for estimating and adjusting for the number and outcomes of missing studies in the meta-analysis.30 Statistical analysis was done using R software 3.02 (R Foundation for Statistical Computing, Vienna, Austria) and the meaning was set to P < 0.05.
Methodological quality assessment
Two authors independently evaluated the risk of bias. In RCTs, biases of 5 elements: selection, performance, detection, attrition, and reporting were assessed using the Cochrane Risk-of-Bias Tool and crossover design according to the Cochrane Handbook.31 For assessing of non-RCT studies, the risk of bias was assessed using Joanna Briggs Institution (JBI) critical-appraisal checklist adapted for case control.32 Studies were considered as low risk when the quality assessment of the checklist criteria was 50% or above. A trim-and-fill plot was used for the estimation and adjustment of publication bias.30
RESULTS
Search results
Among the 250 articles, which were identified at the initial search, 200 duplicates were excluded. By the screening process, 24 references: no comparative studies (n = 16), review articles or comments (n = 6), article written in language other than English (n = 1), unrelated subject (n = 1), were excluded. The remaining 26 studies underwent full-text review, and we excluded 20 studies: 11 studies, which did not evaluate thigh pain, and 9 studies, which involved short stems other than type 4 short tapered stem.23 Finally, 6 studies: 4 RCTs and 2 retrospective comparative studies were included in this meta-analysis (Fig. 1, Tables 1 and 2).101121223334
Fig. 1
PRISMA flow diagram outlining the clinical study selection process.
PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
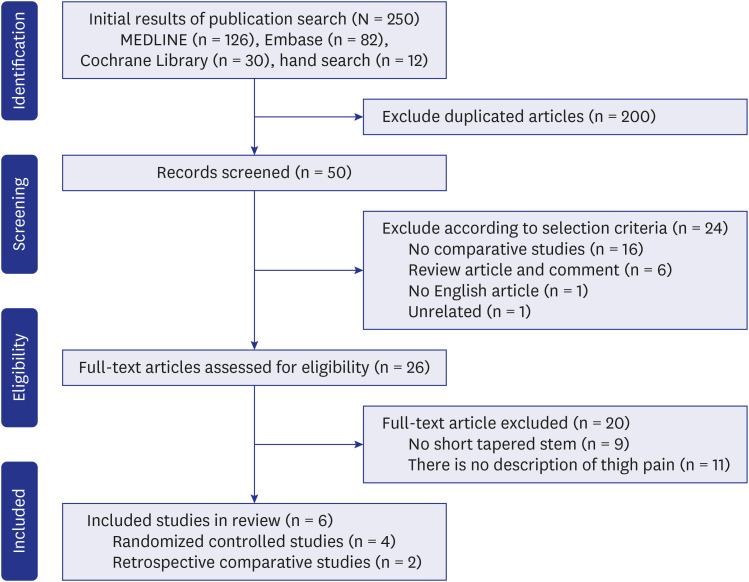
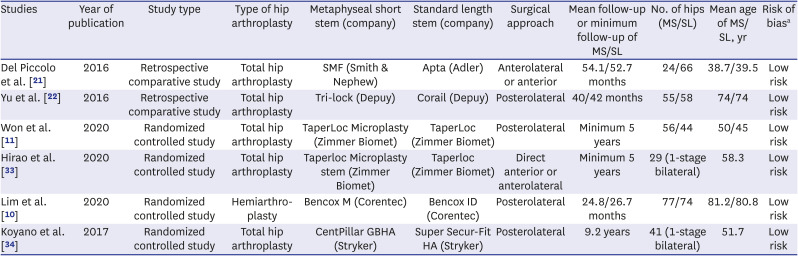
Table 1
Characteristics of the included studies
| Studies | Year of publication | Study type | Type of hip arthroplasty | Metaphyseal short stem (company) | Standard length stem (company) | Surgical approach | Mean follow-up or minimum follow-up of MS/SL | No. of hips (MS/SL) | Mean age of MS/SL, yr | Risk of biasa |
|---|---|---|---|---|---|---|---|---|---|---|
| Del Piccolo et al. [21] | 2016 | Retrospective comparative study | Total hip arthroplasty | SMF (Smith & Nephew) | Apta (Adler) | Anterolateral or anterior | 54.1/52.7 months | 24/66 | 38.7/39.5 | Low risk |
| Yu et al. [22] | 2016 | Retrospective comparative study | Total hip arthroplasty | Tri-lock (Depuy) | Corail (Depuy) | Posterolateral | 40/42 months | 55/58 | 74/74 | Low risk |
| Won et al. [11] | 2020 | Randomized controlled study | Total hip arthroplasty | TaperLoc Microplasty (Zimmer Biomet) | TaperLoc (Zimmer Biomet) | Posterolateral | Minimum 5 years | 56/44 | 50/45 | Low risk |
| Hirao et al. [33] | 2020 | Randomized controlled study | Total hip arthroplasty | Taperloc Microplasty stem (Zimmer Biomet) | Taperloc (Zimmer Biomet) | Direct anterior or anterolateral | Minimum 5 years | 29 (1-stage bilateral) | 58.3 | Low risk |
| Lim et al. [10] | 2020 | Randomized controlled study | Hemiarthroplasty | Bencox M (Corentec) | Bencox ID (Corentec) | Posterolateral | 24.8/26.7 months | 77/74 | 81.2/80.8 | Low risk |
| Koyano et al. [34] | 2017 | Randomized controlled study | Total hip arthroplasty | CentPillar GBHA (Stryker) | Super Secur-Fit HA (Stryker) | Posterolateral | 9.2 years | 41 (1-stage bilateral) | 51.7 | Low risk |
MS = metaphyseal short stem, SL = standard length stem.
aRisk of bias; For assessing the risk of bias in the randomized clinical trial study using the Cochrane Risk-of-Bias Tool and the randomized clinical trial study using the Joanna Briggs Institution (JBI) critical appraisal checklist adapted for case–control.
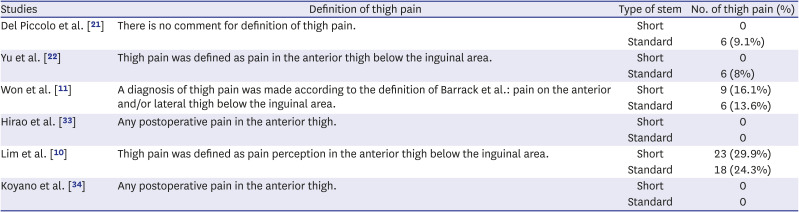
Table 2
Definition of thigh pain in included studies
| Studies | Definition of thigh pain | Type of stem | No. of thigh pain (%) |
|---|---|---|---|
| Del Piccolo et al. [21] | There is no comment for definition of thigh pain. | Short | 0 |
| Standard | 6 (9.1%) | ||
| Yu et al. [22] | Thigh pain was defined as pain in the anterior thigh below the inguinal area. | Short | 0 |
| Standard | 6 (8%) | ||
| Won et al. [11] | A diagnosis of thigh pain was made according to the definition of Barrack et al.: pain on the anterior and/or lateral thigh below the inguinal area. | Short | 9 (16.1%) |
| Standard | 6 (13.6%) | ||
| Hirao et al. [33] | Any postoperative pain in the anterior thigh. | Short | 0 |
| Standard | 0 | ||
| Lim et al. [10] | Thigh pain was defined as pain perception in the anterior thigh below the inguinal area. | Short | 23 (29.9%) |
| Standard | 18 (24.3%) | ||
| Koyano et al. [34] | Any postoperative pain in the anterior thigh. | Short | 0 |
| Standard | 0 |
Comparison of the incidence of thigh pain between short stem and standard-length stem
The 6 articles analyzed the incidence of thigh pain in 594 hips of 524 patients (282 hips with short tapered stems and 312 hips with standard tapered stems) (Table 1).
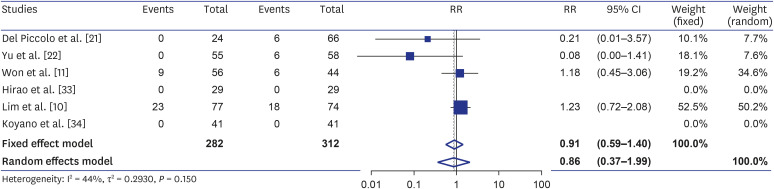
Overall incidence of thigh pain in all studies
There was little evidence of heterogeneity across the studies (I2 = 44%; P = 0.150) and the fixed-effects model was used for the comparison. There was no significant diffenrece in the risk of thigh pain between the short tapered stem group and the standard tapered stem group (RR = 0.91; 95% CI, 0.59–1.40; Z = −0.44; P = 0.663) (Fig. 2).
Sensitivity analyses according to the study design
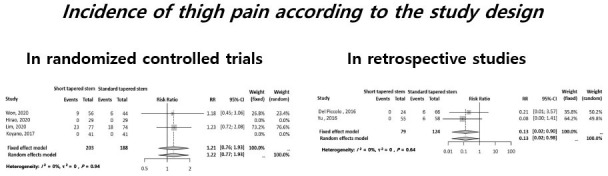
(1) Incidence of thigh pain in RCTs
Four RCTs evaluated the incidence of thigh pain in a total of 391 hips: 203 hips with short tapered stems and 188 hips with standard tapered stems.10113334 There was little evidence of heterogeneity across the studies (I2 = 0%; P = 0.940) and the fixed-effects model was used. There was not significant difference in the risk of thigh pain between the two groups (RR = 1.21; 95% CI, 0.76–1.93; Z = 0.82; P = 0.410) (Fig. 3).

(2) Incidence of thigh pain in retrospective studies
Two retrospective reviews evaluated the incidence of thigh pain in a total of 307 hips: 79 hips with short tapered stems and 124 hips with standard tapered stems.212235 There was little evidence of heterogeneity across the studies (I2 = 0%, P = 0.640) and the fixed-effects model was used. The risk of thigh pain development was significantly lower in the short tapered stem group than in the standard tapered stem group (RR = 0.13; 95% CI, 0.02–0.09; Z = −2.07; P = 0.039) (Fig. 4).

DISCUSSION
Main findings of this meta-analysis are: 1) in the overall analysis, the short tapered stem did not reduce the incidence of thigh pain, 2) in the subgroup analysis of the retrospective studies, the short tapered stem reduced the risk of thigh pain compared to the standard-length tapered stem, and 3) in the subgroup analysis of RCTs, there was no difference in the risk of thigh pain between the two stem designs.
Currently, cementless stems are in wide use due to excellent long-term results.78 Nevertheless, stress-shielding and thigh pain are remaining concerns of cementless stems.1011 Thigh pain is a source of dissatisfaction of the patient and sometimes it is persistent and disabling. The etiology of thigh pain after cementless hip arthroplasty is unrevealed, yet, but it seems to be multifactorial. Bone-prosthesis micromotion, stress concentration at the tip of the stem, periosteal irritation, or a mismatch of Young’s modulus of elasticity between the prosthetic stem and the femur have been suggested as possible causes.3637
Short cementless stems provide more physiologic loading to the proximal femur than conventional stems and have been expected to preserve bone stock of the proximal femur and reduce the rate of thigh pain.13 However, we found no substantial difference between short- and standard tapered stem designs in the rate of thigh pain.
One interesting finding of our review is that the short stems had a lower incidence of thigh pain compared to the standard length stem in retrospective studies, but the risk was not different between the two stem designs in RTCs. The difference could be explained by two reasons. First, the differences in the structural rigidity of various stem designs might have affected the incidence of thigh pain. Stress transfer from stem to femur might be a cause of pain based on the concept of a mismatch in structural rigidity between stem and femoral bone.36 The structural rigidity of stem is determined by its geometry, size, and implant material (modulus of elasticity).36 The stress at the stem tip-anterior femoral cortex interface was higher in cobalt-chromium stems than in the titanium alloy stems.14 Thus, the titanium alloy stems had a lower incidence of thigh pain compared to the cobalt-chromium stems.38 It is ideal to compare two stem designs with identical proximal geometry but different lengths for the detection of difference in the thigh pain incidence according to the stem length.1920 The stems compared in retrospective studies were from different manufacturers and had various shapes. However, in RTCs, the manufacturer was the same in each study and compared stem designs had similar proximal geometries. Second, reporting bias in the data collection of thigh pain might have affected the evaluation of thigh pain. In retrospective studies, there was no description on the definition of thigh pain.2133 In addition, it is possible that these retrospective studies lacked in the differentiation of thigh pains due to other etiologies. However, in RTCs, the diagnostic criteria of thigh pain were pre-defined and the development of thigh pain was prospectively assessed in serial follow-up evaluations.
There are several limitations in our study. First, the diagnostic criteria of thigh pain might be different in each study. Radiating pain on lateral thigh due to spinal problems might have been counted as stem-related thigh pain. There is no unified definition or diagnostic criteria of thigh pain, yet. Brown et al.36 defined thigh pain as the pain that occurs in well-fixed femoral components after primary cementless hip arthroplasty, and pains due to other origins should be differentiated.20 Second, bone quality of the proximal femur was not counted. Engh et al.37 reported that the incidence of thigh pain was higher in patients with poor bone quality than in those with good bone quality. Moreland and Bernstein39 also reported that patients with preoperative osteopenia had high incidence of thigh pain and argued that it was caused by the difference of elastic modulus between stem and proximal femur. On the other hand, Burkart et al.38 and Bourne et al.40 reported that Dorr’s femoral morphology was not associated with thigh pain.14 Third, patient factors were not adjusted. Several studies have reported an association between thigh pain and age. Amendola et al.17 and Nam et al.41 reported that younger patients experienced thigh pain more frequently than older patients, because young patients had high activity and more demand after hip arthroplasty. However, we included only comparative studies, and the mean ages between the two stem design groups were similar or same in the involved studies. Thus, we thought the effect of patient factor was negligible. Fourth, we analyzed only type 4 short-tapered stems and our results might not be generalized to other short stem designs.
In conclusion, we found no substantial difference in the incidence of thigh pain between short tapered stem and standard-length tapered stem in hip arthroplasty. The design of cementless stems should be more developed to reduce this annoying complication.
 XML Download
XML Download